
Abstract
Background
The performance of thyroidectomies has been increasing over the last decade due to the growing prevalence of thyroid diseases. The purpose of this study was to investigate the clinical significance of preoperative vocal cord paralysis (VCP) associated with thyroid disease and other incidences of malignant or benign lesions, as well as different thyroid pathological features. Additionally, the epidemiological changes of thyroid diseases with preoperative VCP were investigated.
Methods
Ninety-nine out of 12,530 patients with preoperative VCP who had undergone thyroid surgery for various diseases in the Zhejiang Cancer Hospital from January 2007 to December 2015 were identified. Their clinicopathological data was recorded and case distributions from different years and intraoperative recurrent laryngeal nerve statuses were retrospectively analyzed.
Results
The incidence of preoperative VCP in 2007 was reported to be 1.53% (9/590) and had decreased to 0.53% (12/2,247) by 2015 (P < 0.05). Among the 99 patients with preoperative VCP, 81 had malignancies (81.82%), while 18 (18.18%) had benign thyroid diseases. The incidences of preoperative VCP in malignant and benign diseases were 1.13% (81/7,159) and 0.35% (18/5,371), respectively (P < 0.05). There were only 5 (0.04%, 5/12,530) cases of papillary thyroid microcarcinoma with preoperative VCP. There was no statistical difference between the incidence of preoperative hoarseness in malignant 69.14% (56/81) and benign diseases 61.11% (11/18) with preoperative VCP.
Conclusions
The preoperative VCP incidence rate had gradually decreased with an increased proportion of papillary thyroid cancer. Preoperative voice symptoms do not necessarily suggest a malignancy. Selective rather than routine preoperative laryngoscopic examinations should be performed on papillary thyroid microcarcinomas. The probability of preoperative VCP in malignancy was significantly higher than in benign lesions.
Introduction
Thyroid diseases are becoming increasingly prevalent worldwide due to various reasons1,2. Benign thyroid disease includes simple or nodular goiter, thyroid adenoma, Hashimoto’s thyroiditis, hyperthyroidism, and hypothyroidism. As for thyroid malignancies, the papillary thyroid carcinoma showed a steady increase in the incidence rate among the four pathological types of thyroid carcinoma. The thyroidectomy has been the mainstay of treatment for thyroid diseases, and its performance has shown a sharp upward trend over the last decade. During a thyroidectomy, the surgeon’s primary focus should be on the functions of the vocal cord and the recurrent laryngeal nerve on the premise of complete removal of all the thyroid tumors. 3 The prevalence of preoperative vocal cord paralysis (VCP) in both thyroid malignancy disease and other benign disease varies greatly throughout different studies.4-7 From review of the relevant literature, the incidence of preoperative VCP ranges from 8% to 11% for thyroid malignancy and from 0.7% (8/1156) to 1.0% for benign thyroid diseases in large surgical series. Chiang et al. reported the incidence of preoperative VCP was 10% (15/156) among thyroid malignancy and 0.2% (1/ 466) among benign lesions.4-7 While Wang et al. 4 reported a VCP rate of 5.52% (8/145) in patients with benign thyroid diseases. The relationship between preoperative VCP with different histopathologies and the necessity of a preoperative laryngoscopy during a routine examination still remains unclear.8-10
Preoperative VCP was previously considered a significant marker in malignant conditions, but some studies have reported VCP in benign nodules.4,6 However, the number of cases in most of the published studies was less than 30, and similarly, the preoperative symptom of hoarseness was observed in very few patients. The distributional trend of preoperative VCP in recent years has not been reported, and the level of evidence that supports selective rather than routine preoperative laryngoscopic examinations was weak.11-13 Therefore, more research is warranted on preoperative VCP and the incidence rates of malignant tumors and benign diseases.
The purpose of this study was to investigate the clinical significance of preoperative VCP associated with thyroid diseases. The incidences of preoperative VCP in malignant and benign lesions were compared, and the incidence of preoperative VCP in papillary thyroid microcarcinoma was also calculated. In addition, this study focused on the epidemiological changes of thyroid diseases with preoperative VCP.
Methods
Clinical data
Clinical records of 15,248 patients who had undergone thyroid surgery in the Zhejiang Cancer Hospital between January 1, 2007 and December 31, 2015 were retrospectively analyzed. Patients with other malignancies, such as hypopharyngeal cancer or invading thyroid cancers, were excluded from the study. Patients who had a history of thyroid, cervical, and thoracic surgeries were also excluded from the study. Finally, the cases of 12,530 patients who had received primary thyroid surgery were selected for this study.
All patients had accepted preoperative fibro-laryngoscopic examinations. Among the 12,530 patients with preoperative ipsilateral VCP, 99 were selected according to their fibro-laryngoscopy results. Analysis of the left or right side VCP was conducted according to the different pathological results. The patients’ clinical characteristics, including gender, age, body mass index, family history of cancer, year of diagnosis, and other items, were recorded in detail; symptoms of hoarseness and duration, as well as imaging data from ultrasounds and computer tomography scans of the thyroid, neck, and chest, were also recorded.
Preoperative consent was obtained from each patient, which included information regarding the associated surgical risks, with particular emphasis placed on the possibility of a recurrent bilateral laryngeal nerve injury. Nearby anesthesiologists and related personnel were accessible to administer first aid in cases of postoperative dyspnea. Intraoperative procedures were systematically recorded, which included the RLN invasion status and the anatomic conditions. The surgical range of the central compartment and neck dissection were also recorded in detail.
Postoperative pathological results of all cases were divided into seven main pathological categories, according to the World Health Organization disease classification. 14 The incidence of VCP in each pathological category and the VCP distribution from different years were analyzed and recorded. The tumor lymph node and metastasis staging system was applied in malignant cases. Furthermore, postoperative treatment conditions were collected. The voice function recovery status of patients who had an RLN invasion during the operation was also observed.
The percentage of papillary cancer and papillary thyroid microcarcinoma cases during the observed years was calculated to explore reasons for the gradual decrease in the incidence rates of preoperative VCP. Additionally, the incidence of VCP among different malignant histopathologies was compared.
Statistical analysis
The data were presented as categorical variables. Statistical analyses were performed using the SPSS 23.0 Mac software (IBM Corp.). The chi-square test was used to compare the differences between the groups. A P-value of ≤ 0.05 in a two-tailed test was considered statistically significant. The Prism 6.0c software (Graph Pad Software, Inc.) was used for basic statistical analysis of the figures.
Results
The incidence rate of preoperative VCP in 2007 was reported to be 1.53%, and by 2015, it had decreased to 0.53% (P < 0.05). Concurrently, the percentage of papillary cancer cases had increased gradually from 30.34% in 2007 to 72.36% in 2015 (P < 0.05). The percentage distribution of VCP and thyroid papillary carcinoma observed over the course of different years is summarized in Figures A and B, respectively. Figure 1 shows that the average incidence rate of VCP was 0.79% between 2007 and 2015, and a sharp decrease occurred in 2011. The average percentage of papillary cancer cases in all thyroid malignancies was 57.13%, and the proportion of papillary cancer had gradually increased, especially in 2011 (Figure 1). We found it interesting that there were only 5 (0.04%, 5/12,530) cases with preoperative VCP in papillary thyroid microcarcinomas. The curve for distribution of vocal fold paralysis and thyroid papillary carcinoma in different years. (A) curve of vocal fold paralysis probability. (B) curve of papillary carcinoma probability.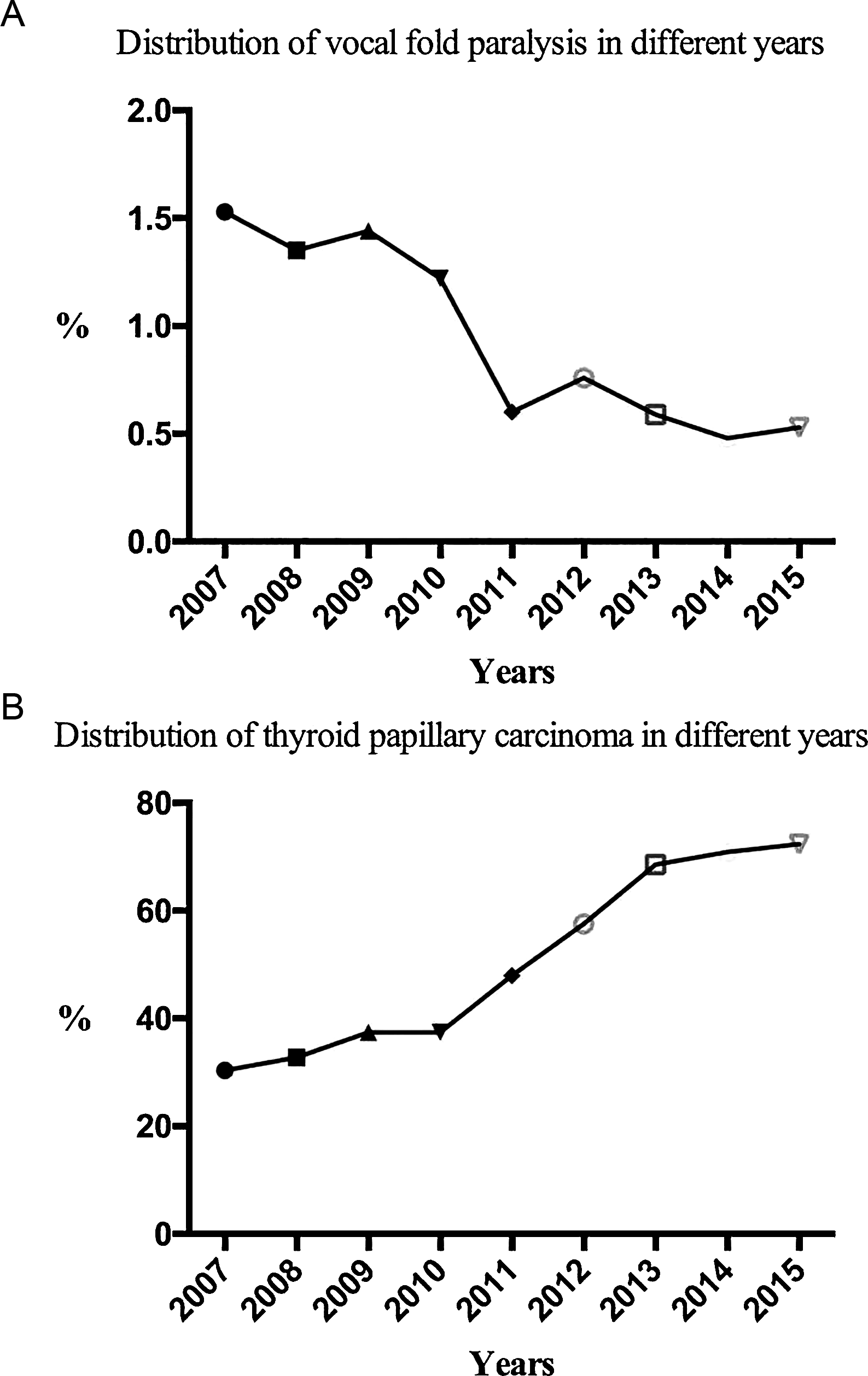
Clinicopathologic features of 99 patients with preoperative vocal cord paralysis in different pathologies during 2007 through 2015.
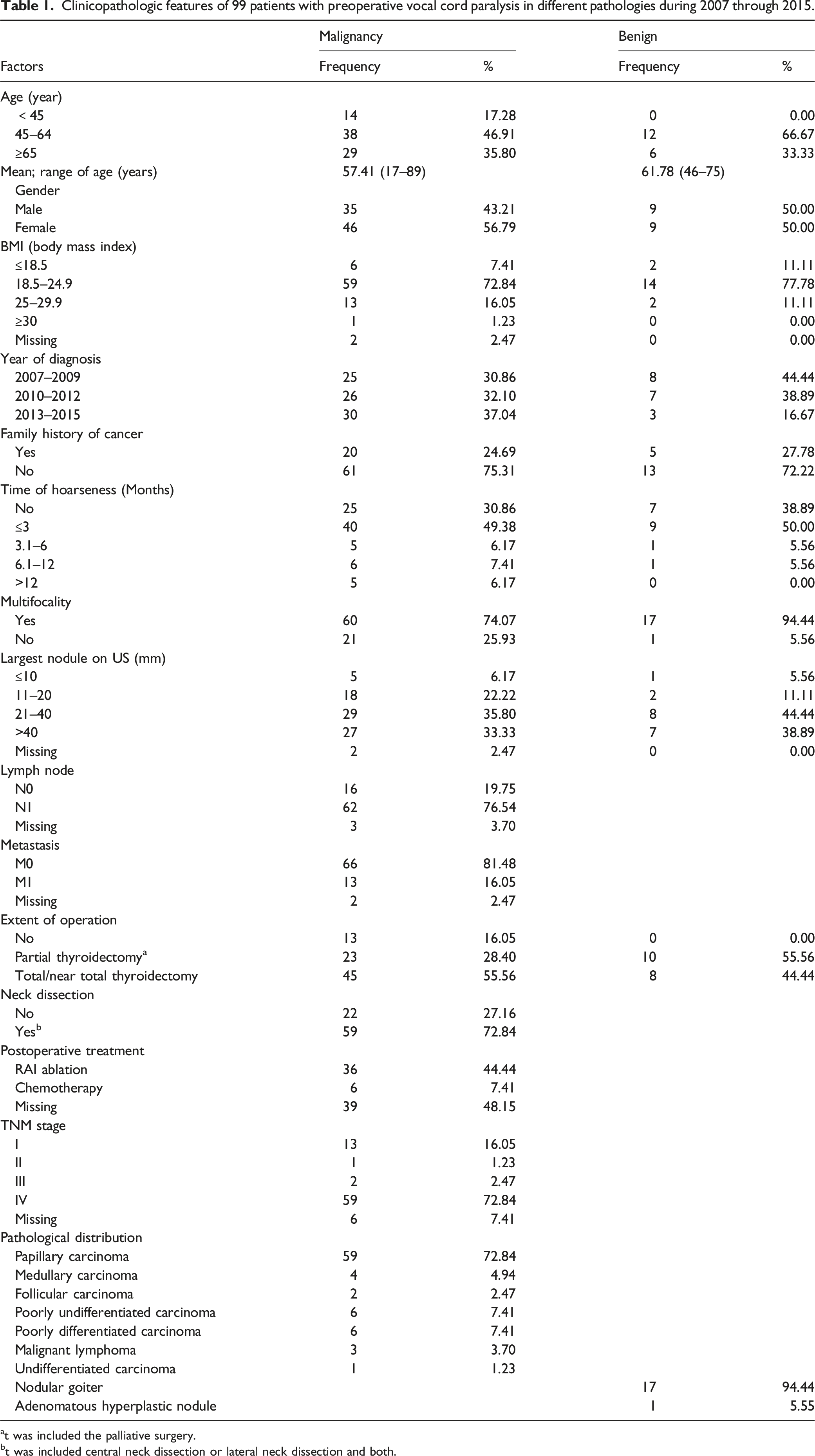
at was included the palliative surgery.
bt was included central neck dissection or lateral neck dissection and both.
Comparison of the incidence of preoperative hoarseness in different pathological features.
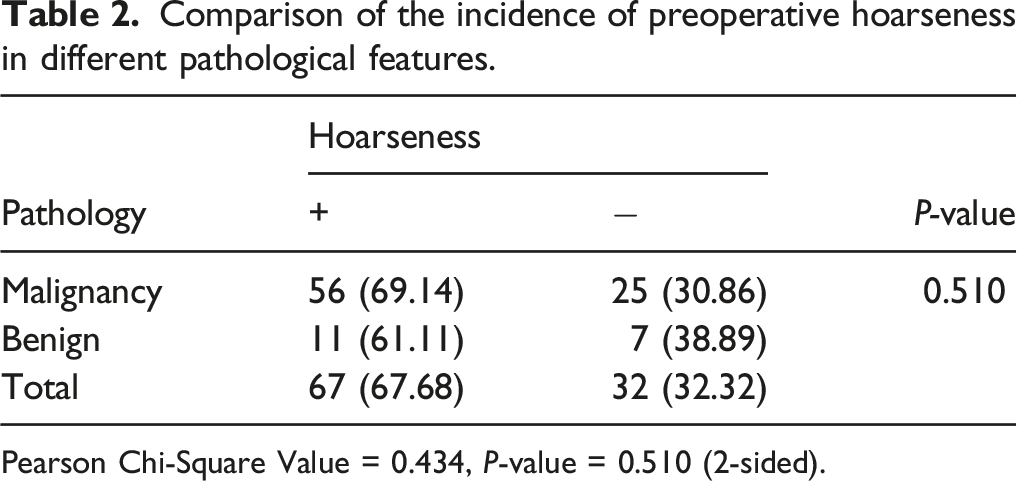
Pearson Chi-Square Value = 0.434, P-value = 0.510 (2-sided).
Condition of recurrent laryngeal nerve during the surgery in different pathological features.
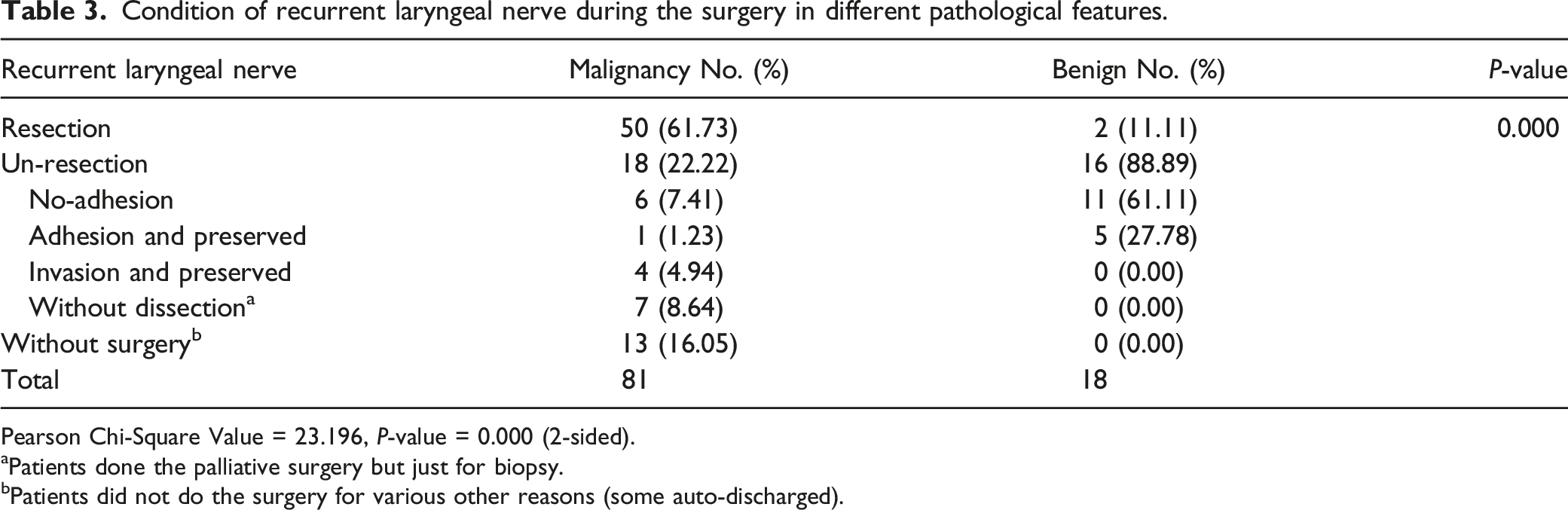
Pearson Chi-Square Value = 23.196, P-value = 0.000 (2-sided).
aPatients done the palliative surgery but just for biopsy.
bPatients did not do the surgery for various other reasons (some auto-discharged).
Distribution of vocal fold paralysis in different pathological results.
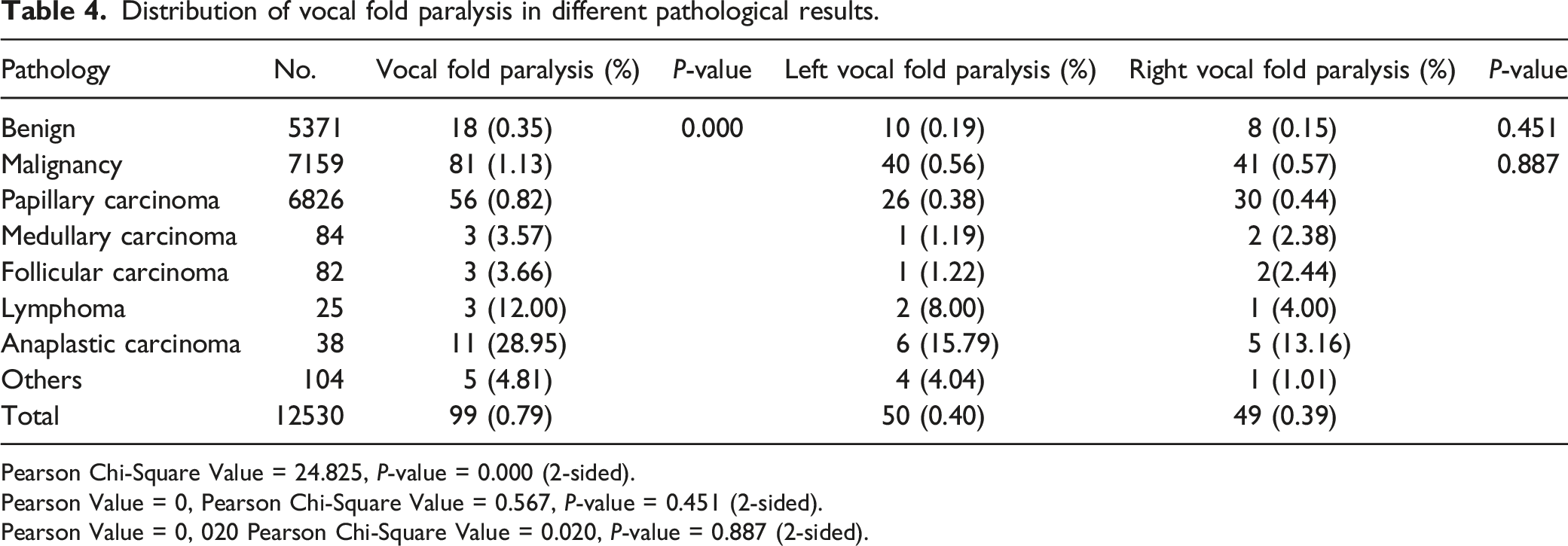
Pearson Chi-Square Value = 24.825, P-value = 0.000 (2-sided).
Pearson Value = 0, Pearson Chi-Square Value = 0.567, P-value = 0.451 (2-sided).
Pearson Value = 0, 020 Pearson Chi-Square Value = 0.020, P-value = 0.887 (2-sided).
In addition, intraoperative neuro-monitoring was applied in 3 of the 99 cases, and all three nerves were preserved. Two patients underwent a postoperative tracheotomy.
Discussion
To our knowledge, there are several studies that have reported incidences of preoperative VCP in patients with thyroid diseases,4-7 but very few studies in recent years have described the epidemiological trends of preoperative VCP. In this study, we revealed a gradually decreased trend of preoperative VCP between 2007 and 2015. There are several possible reasons associated with this decreased condition. The steady increase in the incidence rate of papillary thyroid carcinoma largely attributed to the increased detection and improved diagnostic methods.15-17 With a growing awareness of asymptomatic thyroid cancer, an ultrasound of the thyroid glands has been considered an essential part of an annual healthcare examination. 18 With an increased detection rate of asymptomatic thyroid cancer, most incidental thyroid cancers are discovered in the early stages and are not accompanied by preoperative VCP.
The epidemiological trends of preoperative VCP cannot easily be found in existing studies, but according to various published papers, the prevalence seems to be declining. The prevalence rates of preoperative VCP with thyroid malignancies ranged from 2.8% (20/709) to 9.1% (29/319), as reported in studies dated from 2004 to 2009.19,20 The rates then dropped to a range of 0.6% (8/1,333) to 6.4% (12/187) between 2010 and 2014.4,21 A study published in 2015 by Kay-Rivest et al. 5 reported 25 cases of thyroid malignancies with preoperative VCP found in 1,923 health records between 2007 and 2014. The prevalence of preoperative VCP in the cases of malignancies that were reported in Kay-Rivest’s study was 1.3% (25/1,923), which was very close to our determination of 1.13% (81/7,159), and these two studies had enrolled patients at approximately the same time.
With a decline in the incidence rate of preoperative VCP, establishing the need for a preoperative routine laryngoscopy to determine a diagnosis 9 is now becoming an urgent issue. A preoperative routine laryngoscopy has some advantages. First, preoperative VCP can occur in patients with normal voice quality, which could indicate a malignancy. Second, it can assist with the surgery when the function of an RLN is known beforehand. Third, it provides a baseline for postoperative follow-up. Finally, the status of preoperative VCP also provides a safeguard for surgeons against potential medical disputes. All the patients in our study were examined using a direct fiberoptic laryngoscope before surgery.
Various other studies have recommended a selective use of the laryngoscopy rather than a routine use,22-25 and the authors concluded that the prevalence rate of asymptomatic VCP ranged from 0.23% to 0.7%.22-24 Similarly, the percentage of asymptomatic prevalence was 0.25% (32/12,530) in our study. Therefore, the positive diagnostic rate in the preoperative laryngoscopy was very low in asymptomatic VCP and the selective use of the preoperative laryngoscopy was deemed more acceptable. We explored methods in this study that could select low-risk patients and avoid unnecessary preoperative laryngoscopic procedures. At present, we discovered a very low proportion of preoperative VCP in patients, with the largest nodule diameter of ≤1 centimeter identified through ultrasounds. In our study, only 5 patients were found to have papillary microcarcinomas, which accounted for 0.04% (5/12,530) of the cases. Our data offered a simple and effective method to screen for low-risk patients; these patients were identified as having no symptoms of hoarseness and presenting nodule sizes of ≤1 cm.
Vocal symptoms can occur in both malignant and benign lesions. In our study, preoperative hoarseness showed no statistical significance in different pathological types. Hence, hoarseness cannot be considered a good predictor for malignancies.
Preoperative VCP has been previously regarded as a sole marker of thyroid malignancies, but some papers have described this phenomenon in benign thyroid diseases as well.6,23 Therefore, preoperative VCP may not be considered a perfect indicator. Although malignancies have higher incidence rates of preoperative VCP, benign lesions may be prone to this condition as well. Benign lesions with preoperative VCP are mainly caused by physical oppression and longtime inflammation of RLNs. 26 For malignancies, preoperative VCP is the result of a direct invasion of an RLN in most cases. The probability of preoperative VCP was associated with the degree and position of the malignancy, and its incidence in poorly differentiated and anaplastic thyroid cancer was 35 times higher than that of papillary carcinoma in our study. In a study by Chiang et al., 7 16 malignant tumors were reported to have exhibited different histopathological distributions. The preoperative VCP rates were reported to be 80% (4/5) in the anaplastic carcinomas and 5.97% (8/134) in the papillary carcinomas. 7 There was a lack of cases with different histopathological types.
The intraoperative RLN excision rate varies in benign lesions and different malignancies. The RLN excision rate had increased with the invasion of a malignancy. All nerves were excised in patients with poorly differentiated and anaplastic thyroid cancer. The RLN was even sacrificed in two cases with benign lesions. Nerve swelling was evident in two benign lesions and the RLN had degenerated after long direct compression. Hence, benign lesions with preoperative VCP need more attention. Even in the case of a benign lesion, the RLN may not be able to be retained in the operation. Patients with benign lesions should be fully informed of all risks before the operation.
An RLN should be dissected carefully and precisely in both malignant and benign lesions. If the nerve can be preserved, nerve function may be recovered postoperatively without affecting the prognosis, even in the case of an adhesion.27,28 Boucek et al. 29 developed a new algorithm for the surgical management of RLN infiltration with a different risk stratification strategy. In benign diseases and lymphoma, it has been recommended to preserve the RLN, while RLN resection had been reasonable for the medullary or anaplastic histology. In our study, all RLNs with poorly differentiated and anaplastic neoplasms were resected for infiltration.
Some studies have shown a preponderance of left-sided VCP.5,30 According to a few other studies, the proportion of VCP to date has shown no significant differences between the left and right side. 6 The left RLN is more vulnerable to injury than the right RLN due to a lower origin and a longer length. As determined in the clinical observations, VCP occurrence was more commonly associated to the left side. 31 In terms of the thyroid region, the right RLN crosses the right subclavian artery and loops posteriorly under the artery. The right RLN was initially traversed at an angle towards the tracheoesophageal groove, making it relatively farther to the esophageal tracheal groove than the left RLN. Therefore, the left and right RLNs have close to the same length in the thyroid region. The limitation of this study is that it was a retrospective analysis, although the patients enrolled were between 2007 and 2015, spanning about 10 years, it was still a single-center experience. Meanwhile, the recurrent laryngeal nerve repair and reconstruction techniques have not been applied to the cases in this study.
Conclusions
The incidence of preoperative VCP has gradually decreased with increased proportions of papillary carcinoma. The incidence of preoperative VCP was quite low in the papillary thyroid microcarcinomas. Selective rather than routine use of a preoperative laryngoscopy is acceptable in cases of papillary thyroid microcarcinoma.
The probability of preoperative VCP was significantly higher in malignant neoplasms than in benign lesions. Thyroid tumors with preoperative VCP strongly suggest malignancies and have a higher rate of intraoperative nerve sacrifice, but preoperative symptoms of hoarseness do not necessarily indicate a malignancy. The RLN should be preserved if there is no evidence of an invasion by the tumor to offer an opportunity for postoperative nerve function recovery.
Footnotes
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zhejiang Province Medical and Health Sciences Project (No. 2021KY086).
Data availability statements
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics approval and consent to participate
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of The Cancer Hospital of the University of Chinese Academy of Sciences. This study is retrospective, and patients' informed consent is allowed to be waived.