
Abstract
Primary intraosseous hemangiomas of the maxillofacial region are rare lesions that comprise less than 1% of all osseous tumors. A review of the literature on primary intraosseous hemangiomas of the facial bones revealed a limited number of publications, much of which was largely limited to case reports. This case report summarizes the workup and surgical treatment of a 37-year-old female with a primary intraosseous hemangiomas of the left maxillary bone. The image, histology, treatment, and literature are reviewed.
Introduction
Primary intraosseous hemangiomas, also referred to as hemangiomas of the bone, are benign tumors characterized by the presence of small and large vascular channels within the bone tissue. They are most commonly observed in the vertebrae and skull. 1 Primary intraosseous hemangiomas occurring in the maxillofacial region are rare, typically presenting as painless, slow-growing lesions. Patients may remain unaware of these lesions unless there is noticeable asymmetry, tenderness, epistaxis, or pain. Here, we present the case of a young girl diagnosed with a primary intraosseous hemangioma affecting the left maxillary bone.
Case Report
A 37-year-old woman presented with a gradually enlarging, painless mass on her left cheek over the past 2 years, primarily causing cosmetic concern. Physical examination revealed a bony, hard, well-demarcated mass measuring approximately 2 × 1 cm on the left maxilla, just inferolateral to the left ala nasi. The mass exhibited limited motion, with normal and mobile overlying skin. Aside from slight inward bulging of the left inferior turbinate, no abnormal findings were observed in the nasal cavity. The patient denied any tenderness, history of trauma, or familial occurrence of similar lesions.
Computed tomography (CT) imaging demonstrated expansive bony destruction at the junction of the anterior and medial walls of the maxillary sinus, measuring approximately 1 × 2 cm (Figure 1). The lesion showed heterogeneous internal density, with a polka-dot appearance on axial images and the corduroy sign on coronal and sagittal images. Enhanced CT revealed significant enhancement of the mass without surrounding tissue invasion.
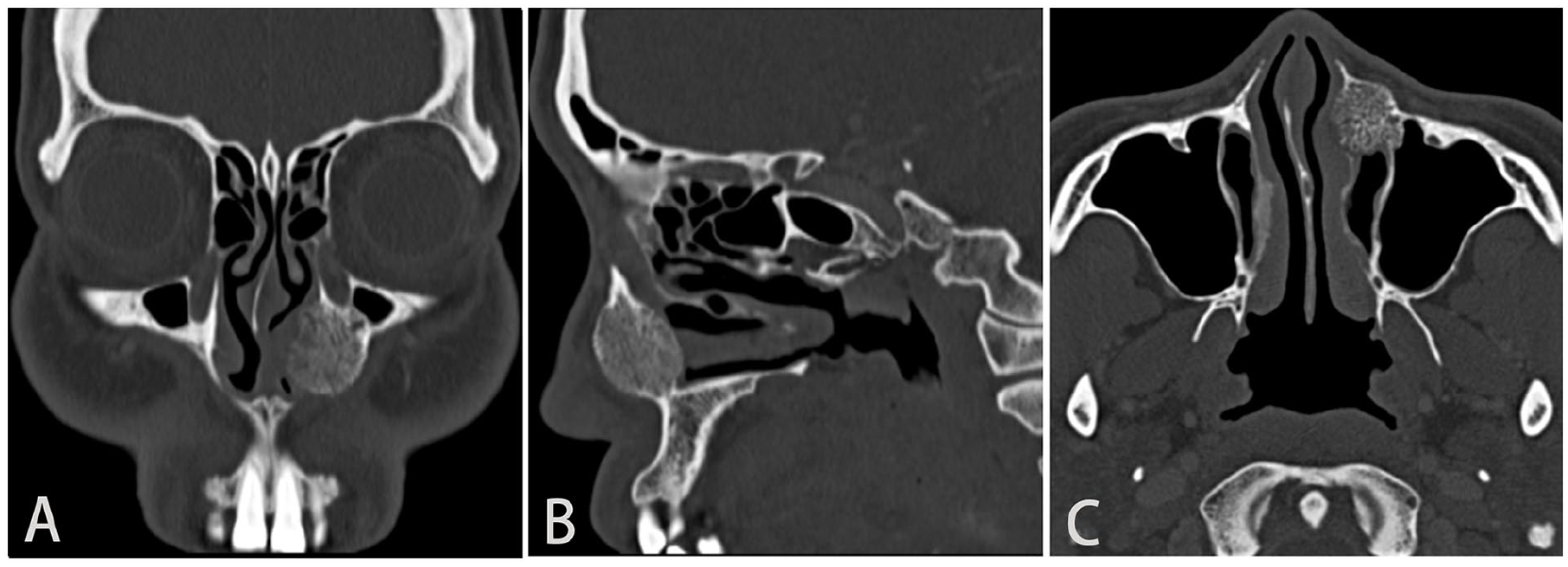
CT scan shows the expansile lesion with thickened vertical trabeculation giving the “corduroy sign” on coronal (A) and sagittal (B) images and the “polka-dot appearance” on axial images (C).
Following thorough preoperative preparation, surgical exploration and lesion removal were performed under general anesthesia via a combined nasolabial groove and prelacrimal recess approach. The tumor exhibited a bluish tinge and bled easily, requiring bone wax for hemostasis. Once the tumor’s connection to normal bone was severed, bleeding significantly decreased. The tumor was excised in sections, revealing a spongy bony structure within the mass (Figure 2A). To facilitate postoperative care and prevent secondary maxillary sinusitis, the maxillary sinus ostium was enlarged through the middle meatus. Two weeks postoperatively, follow-up CT showed complete tumor resection with no residual tumor. At 1 month, the nasal mucosa appeared smooth, with no recurrence or cosmetic deformity. The patient continues to be monitored.
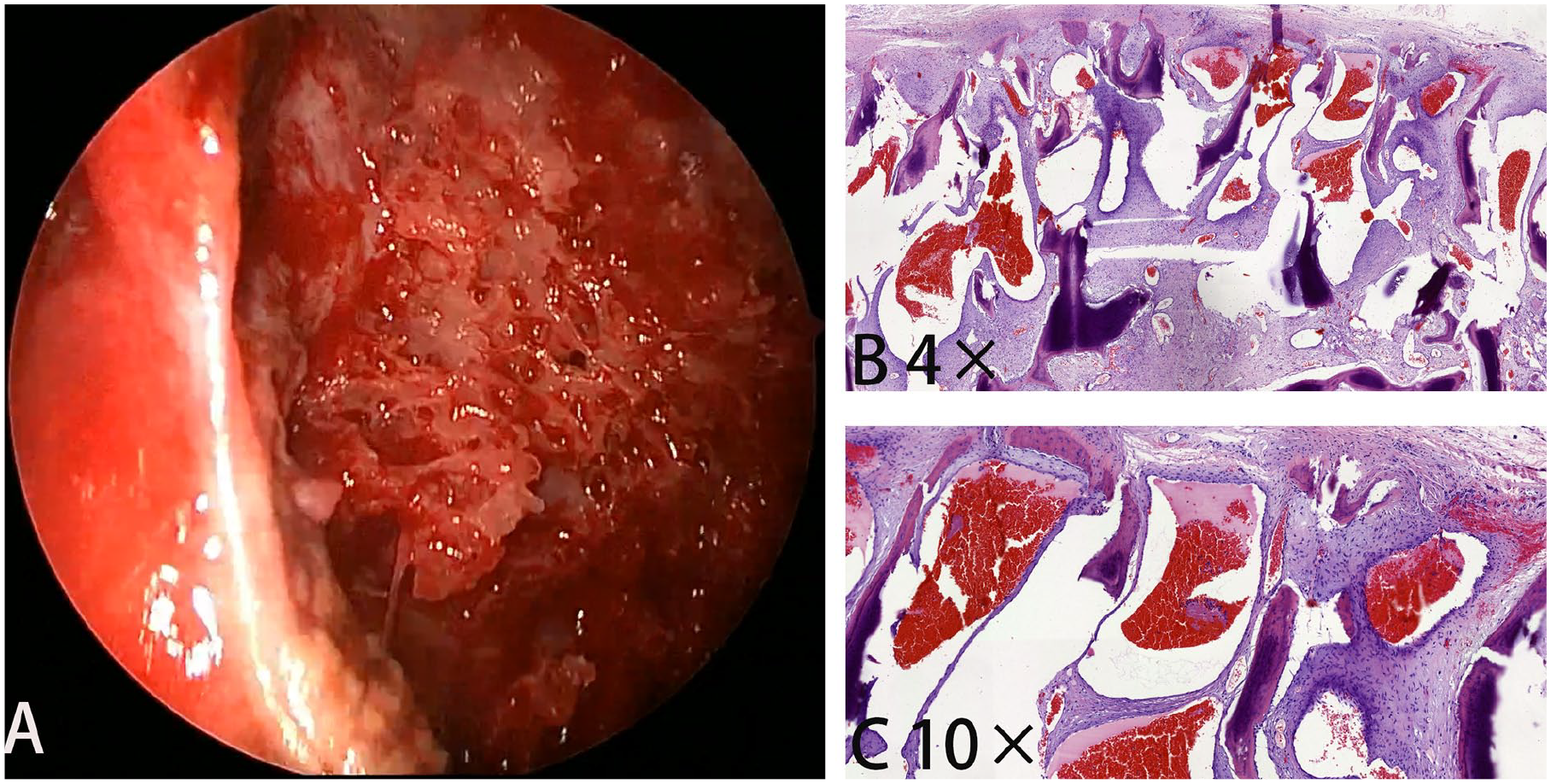
Intra-operative view of intraosseous hemangioma, a spongy bony structure within the mass (A). Cavernous vascular channels separated by trabeculae of cancellous bone. H&E 2× (B). The vascular channels are lined by a single layer of flat endothelial cells and are engorged with erythrocytes H&E 10× (C).
Gross examination revealed a brownish-red, unencapsulated lesion. Histological analysis of decalcified sections stained with hematoxylin and eosin showed numerous thin-walled cavernous vascular channels interspersed with bony trabeculae. The vascular channels were lined by a single layer of flat endothelial cells, frequently filled with erythrocytes (Figure 2B and C). A diagnosis of primary intraosseous hemangioma was confirmed.
Discussion
Primary intraosseous hemangiomas are exceedingly rare, benign vascular anomalies that account for approximately 0.5% to 1% of all osseous tumors. Typically, they are situated within the medullary cavity and initially manifest as bulging before causing erosion of the inner and outer cortical tables. 2 The etiology and pathogenesis of these lesions remain unknown. 2 They most commonly occur in the vertebrae of the thoracic spine, 3 followed by the skull and facial bones, with a predilection for the metaphysis or diaphysis of long bones. 2 Among the facial bones, the mandible, maxilla, nasal bones, and zygoma are the most frequently affected sites, in decreasing order of frequency. 4 While these lesions are generally classified as benign, they may rarely exhibit local aggressiveness.
Hemangiomas can be subdivided into 4 histologic types: intraosseous cavernous hemangioma, intraosseous capillary hemangioma, intraosseous arteriovenous hemangioma (which may represent congenital arteriovenous malformations), and intraosseous venous hemangioma, 5 with the cavernous type being the most common. 6 Histologically, intraosseous hemangiomas exhibit hamartomatous vascular tissue with endothelium surrounding bone trabeculae and permeating the marrow. They may also contain fat, smooth muscle, fibrous tissue, and thrombi. 2 It is important to note that distinguishing between the various histological types on imaging is challenging, except for those with a significant arterial component.
Primary intraosseous hemangiomas occur 3 times more frequently in women than in men. Although they do not show a specific age predilection, they are more commonly observed in the third and fourth decades of life. 7 These tumors are slow-growing and are typically asymptomatic (~99%) unless they exert a mass effect on sensitive structures. They may present as a swelling or palpable mass, particularly in the skull, or, when large and strategically located, they may cause a pathological fracture. 2 In our case, the patient sought medical attention due to facial swelling without significant symptoms such as pain, nasal congestion, purulent nasal discharge, or epistaxis.
Imaging studies for hemangiomas include plain radiography, CT, and magnetic resonance imaging (MRI). Plain radiographs are often the first imaging modality used and may suffice for vertebral or calvarial lesions, revealing a prominent trabecular pattern, sclerotic vertebrae with vertical trabeculae (corduroy sign), lytic calvarial lesions with a spoke-wheel appearance, and irregular lytic lesions in long bones with a honeycomb appearance. CT is the most commonly utilized imaging method, typically showing a mixed or sclerotic bone lesion with internal fat. It allows better visualization of thickened vertical trabeculation, which appears as a polka-dot pattern on axial images and the corduroy sign on coronal and sagittal images. 3 The polka-dot sign, or salt and pepper sign, results from the replacement of normal cancellous bone by thickened vertical trabeculae surrounded by fat marrow or vascular lacunae. 5 On CT, the dots appear white on a black fatty background, whereas on MRI, they are black dots on a white background on non-fat-suppressed T1-weighted images (T1WI) or T2-weighted images (T2WI). The corduroy sign, also known as the jail bar sign, is similarly caused by this replacement process. 8
MRI is highly effective in visualizing the morphology and tissue composition of hemangiomas, making it essential for both diagnosis and differential diagnosis. Typically, hemangiomas exhibit slightly low signal intensity on T1WI and slightly high signal intensity on T2WI, with mild to moderate enhancement observed on contrast-enhanced scans. The signal intensity can vary, largely influenced by the amount of fat content within the lesion.
When internal fat is present and the imaging findings are atypical, the differential diagnosis may include intraosseous lipoma, Paget’s disease, fibrous dysplasia, and non-ossifying fibroma (NOF). Intraosseous lipomas are rare benign lesions, accounting for about 0.1% to 2.5% of all bone tumors. These tumors are composed of mature adipocytes without hematopoietic tissue or bony trabeculae. 9 On imaging, they typically appear as benign-appearing osteolytic bone lesions with well-defined margins and exhibit a homogeneous hyperintense fat signal on T1- and T2-weighted magnetic resonance images. Paget disease of the bone is a common chronic metabolic bone disorder characterized by excessive and abnormal bone remodeling. Radiologically, it typically presents as expanded bone with a coarsened trabecular pattern. The pelvis, spine, skull, and proximal long bones are most frequently affected. Diagnostic markers include elevated serum alkaline phosphatase, normal calcium and phosphorus levels, and increased urine hydroxyproline. 10 Fibrous dysplasia is a developmental benign medullary fibro-osseous process characterized by the failure to form mature lamellar bone, arresting as woven bone that can be multifocal. It can affect any bone and may occur in a monostotic form (involving only 1 bone) or a polyostotic form (involving multiple bones). If the imaging features are characteristic, the lesion does not require histology. 2 Essential imaging features include a bone lesion with compatible imaging characteristics, an osseous part consisting of irregular curvilinear branching trabeculae of woven bone without apparent osteoblastic rimming, and a fibrous part consisting of bland fibroblasts. 11 NOFs are benign and generally self-limiting osteoclastic giant cell-rich bone tumors typically found in the metaphyses of long bones. They are very common in children and adolescents and are considered the most common benign bone tumor. 2 Characteristic radiographic appearances of NOFs include a polycyclic, multiloculated, lucent lesion that is eccentrically located in the metaphysis near the physis, with its long axis parallel to the axis of the bone. They are surrounded by a thin sclerotic rim, and with increasing age, these lesions appear to migrate away from the physis. 12
Preoperative biopsy should be contraindicated due to the risk of uncontrollable hemorrhage. According to the WHO classification of soft tissue and bone tumors (5th edition), 2 diagnostic criteria include typical imaging appearances and the presence of thin-walled blood vessels lined with single, non-atypical endothelial cells on histology.
The treatment method should be determined based on specific circumstances. Incidental cases with typical imaging appearances may not require further work-up or follow-up. However, treatment is necessary if the hemangioma involves or potentially impairs surrounding vital structures as the tumor progresses. This is crucial to prevent cosmetic and functional complications due to tumor growth and destruction of nearby tissues. Factors to consider in selecting treatment include the patient’s age and general health, the size of the lesion, proximity to vital structures, and arterial supply. Treatment options include surgical resection, radiotherapy, injection of sclerosing agents, and intra-arterial embolization.
In cases of maxillary hemangiomas with limited extent, en bloc resection of the lesion can be performed while preserving the morphology and function of the maxilla. However, for extensive lesions, subtotal or total maxillectomy may be necessary. Preoperative planning should thoroughly consider the surgical difficulty and expected blood loss. In cases where significant defects are anticipated, a reconstruction plan should be prepared in advance.
During the surgery in this case, the tumor itself bled profusely, However, when resection was performed along the normal bone surrounding the tumor, bleeding was significantly reduced. Following this, the tumor was excised in segments, revealing a honeycomb-like bony structure within the mass, and additional contouring of the surrounding healthy bone tissue was performed. While literature does not specify the recommended amount of free bony margins needed for en-bloc resection, studies have shown successful removal without recurrence with free margins as little as 0.5 cm. 13
We recommend that for tumors where achieving en-bloc resection is not feasible, the tumor or the majority of it can be isolated within the normal bone initially, followed by segmented resection. This strategy can minimize significant bleeding in the surgical site, as the tumor’s blood supply has been effectively diminished before excision. Alternatively, preoperative arterial embolization can be considered to reduce intraoperative bleeding.
Although surgery remains the preferred treatment modality, it may not be appropriate in cases where complete tumor removal is not achievable, removal may result in facial disfigurement, or there is a high risk of bleeding and mortality. Historically, radiotherapy and intralesional injection of sclerosing agents were attempted for treating hemangiomas of the head and neck. However, radiotherapy alone only inhibits tumor growth without eradicating lesions, and it carries a risk of carcinogenesis. 14 Therefore, this approach is now typically reserved for cases where surgery is not feasible. 15
Conclusion
In conclusion, intraosseous hemangiomas represent a rare clinical entity with an unclear pathogenesis. Patients typically present with progressively enlarging masses, although specific clinical manifestations may vary depending on the tumor’s location. While characteristic imaging findings often raise suspicion for the disease, definitive diagnosis relies on histopathological examination. Currently, complete surgical excision of the tumor is the most effective treatment, as incomplete removal of primary tumor tissue may contribute to recurrence. 16 However, in cases where tumors have a unique location or are deemed unresectable, radiotherapy may be considered as an alternative treatment option.
Footnotes
Acknowledgements
We thank the patient for granting permission to publish this information.
Author Contributions
Yan Qiao Wu conceptualized this study, Shi Chang Li made the literature review, and wrote the first draft of this paper; Ye Zhang and Hao Liu made the literature review. All authors revised the paper and approved the final version for submission.
Data Availability Statement
Original contributions presented in the study are included in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
Ethical approval is not required for this study in accordance with local guidelines. The authors declare that appropriate written informed consent was obtained from the patient for the publication of details of his medical cases and any accompanying images.