
Abstract
Epidermoid cysts of the skull base are rare. We present the case of a woman with an epidermoid cyst at the root of the sphenoidal pterygoid process. She experienced tightness of the forehead skin without headache. Computed tomography (CT) scan revealed a hypodense lesion at the base of the skull in the right middle cranial fossa, which had partly eroded the pterygoid root. Magnetic resonance imaging (MRI) scan revealed a soft cystic mass that eroded the pterygoid root with hypo-/iso-intense on T1-weighted images, hyperintense on T2-weighted images, inhomogeneous hyperintense on diffusion-weighted images, a slightly low apparent diffusion coefficient, and no enhancement, suggesting a diagnosis of an epidermoid cyst. Surgical excision was performed using a nasal endoscope via the pterygoid process—root approach. A histopathological examination confirmed the diagnosis of an epidermoid cyst. At the 6-month follow-up, no recurrence was found on MRI or nasal endoscopy, and the symptoms of forehead tightness disappeared. In conclusion, epidermoid cysts at the root of the sphenoidal pterygoid process are exceptionally rare. Preoperative MRI and CT scans are necessary for the correct diagnosis and differentiation of other low-growing lesions. Nasal endoscopy is crucial for surgical excision and postoperative follow-up for potential recurrence.
Introduction
Since Mueller first described the term “epidermoid cyst” in 1839, 1 it has been recognized as a slow-expanding mass consisting of squamous epithelium and keratin.1,2 According to their location, epidermoid cysts can be divided into 3 types: intracranial epidermoid cysts, external auditory canal epidermoid cysts, and otitis media type epidermoid cysts.1,2 Extradural epidermoid cysts are rare and most commonly occur in the cranial diploic spaces of the temporal, frontal, and occipital bones.3,4 A few dozen cases of cysts in the nasal sinuses have also been documented in the literature.3,4 Intracranial epidermoid cysts represent approximately 1% of all brain tumors and commonly extend to and erode the adjacent skull base. 5 Here, we report a rare case of an epidermoid cyst at the root of the sphenoidal pterygoid process. Accurate diagnosis and complete resection are important for patient prognosis.2,6 Surgical excision and postoperative follow-up in the present case were performed via nasal endoscopy using a pterygoid root approach.
Case Report
A 53-year-old woman with no evident disease history visited our outpatient clinic. She had experienced tight skin on the forehead without headaches for 3 months. She had no history of coma, convulsions, epilepsy, cognitive impairment, cerebrovascular disease, nasal surgery, or head trauma. This study was approved by the Ethics Committee of the First Affiliated Hospital of Shandong First Medical University, and informed consent was obtained from the patient.
Radiological Findings
Cranial computed tomography (CT) scan revealed a hypodense lesion at the base of the skull in the right middle cranial fossa, which had partly eroded the pterygoid root (Figure 1A). Cranial magnetic resonance imaging (MRI) scan revealed a cystic soft lesion that had eroded the pterygoid root of the middle cranial fossa:hypo-/iso-intense on T1-weighted images (Figure 1B, C), hyperintense in T2-weighted images (Figure 1D), inhomogeneous hyperintense on both low and high b-value diffusion-weighted images (DWI, Figure 1E, F), a slightly low apparent diffusion coefficient (ADC, Figure 1G), and no enhancement on MRI enhanced scanning (Figure 1H). These findings suggested a diagnosis of an epidermoid cyst.
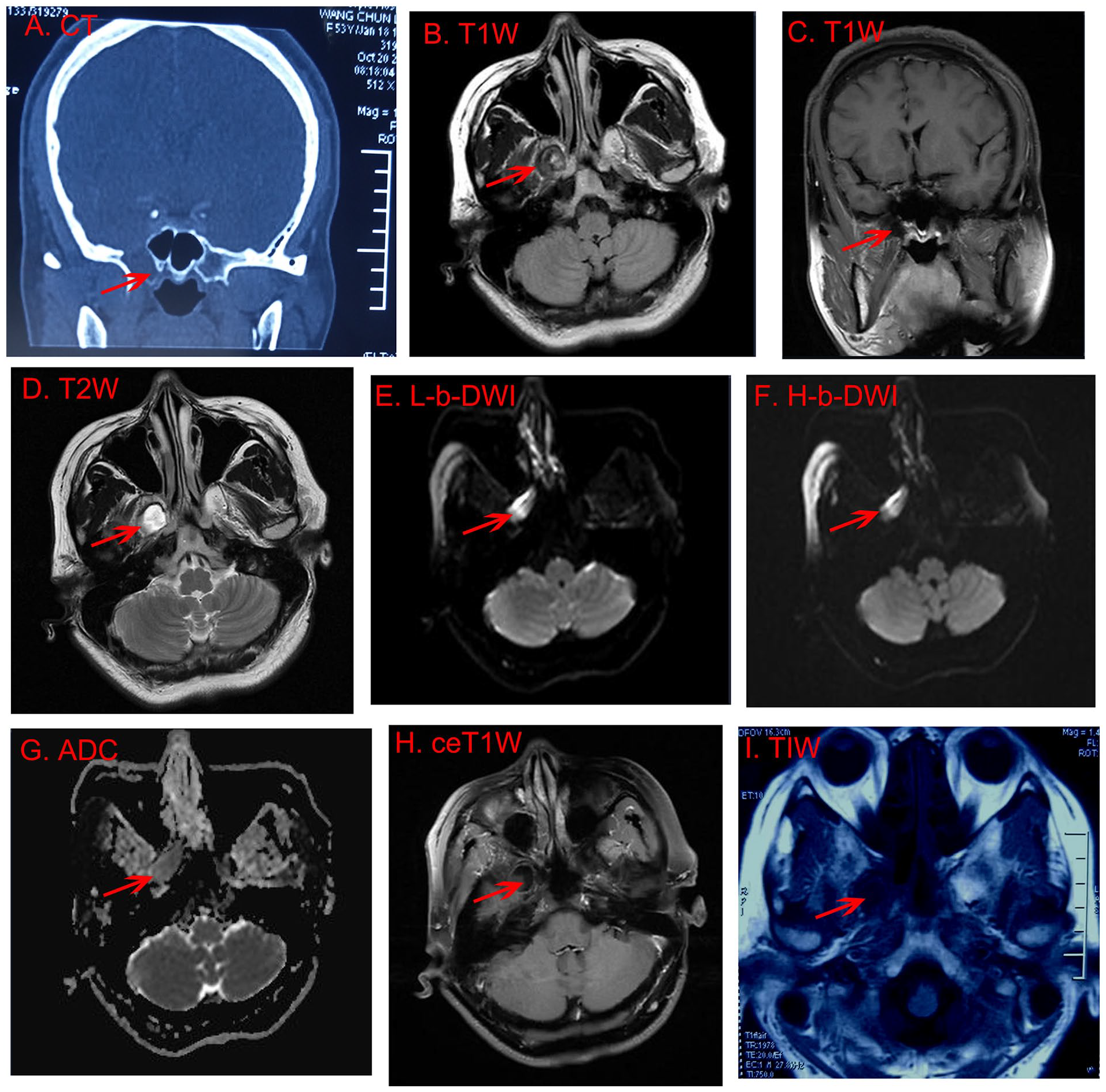
CT and MRI scans. (A) Coronal CT scan showed a hypodense lesion at the skull base of the right middle cranial fossa that had partly eroded the pterygoid root (red arrow); (B, C) horizontal and coronal T1-weighted MRI indicated a hypo-/iso-intense cystic soft lesion eroding the pterygoid root of the middle cranial fossa (red arrow); (D) horizontal T2-weighted MRI indicated a hyperintense lesion (red arrow); (E, F) the lesion appeared inhomogeneous hyperintense on both L-b and H-b value DWI; (G) the lesion had a slightly low ADC; (H) the lesion had no enhancement on MRI ce scanning; (I) 6 months after operation, brain T1-weighted MRI showed no recurrence of cyst in the pterygoid root (red arrow). ADC, apparent diffusion coefficient; ce, contrast-enhanced; CT, computed tomography; DWI, diffusion-weighted images; H-b, high-b; L-b, low-b; MRI, magnetic resonance imaging.
Operative Details
The lower middle part of the right middle turbinate was removed under nasal endoscopy. Next, the sphenopalatine foramen was dissected, and the sphenopalatine artery was electrocoagulated. The soft tissue in the pterygopalatine fossa was gradually separated to expose the pterygoid root. The right sphenoid sinus was successively enlarged through its natural ostium to expose and resect the lateral wall of the right sphenoid sinus. The next step was to separate the nerve of the right pterygoid canal (Figure 2A), outside of which the bone at the root of the sphenoidal pterygoid process was removed (Figure 2A, B). The lesion was located in the right middle cranial fossa with an amorphous yellowish-white epithelioid (Figure 2B). The lesion had partly eroded the bone of the right pterygoid root and did not extend to the skull base, without defects in the endocrine system, bleeding, or cerebrospinal fluid leakage. The contents and walls of the lesion were completely removed (Figure 2C).
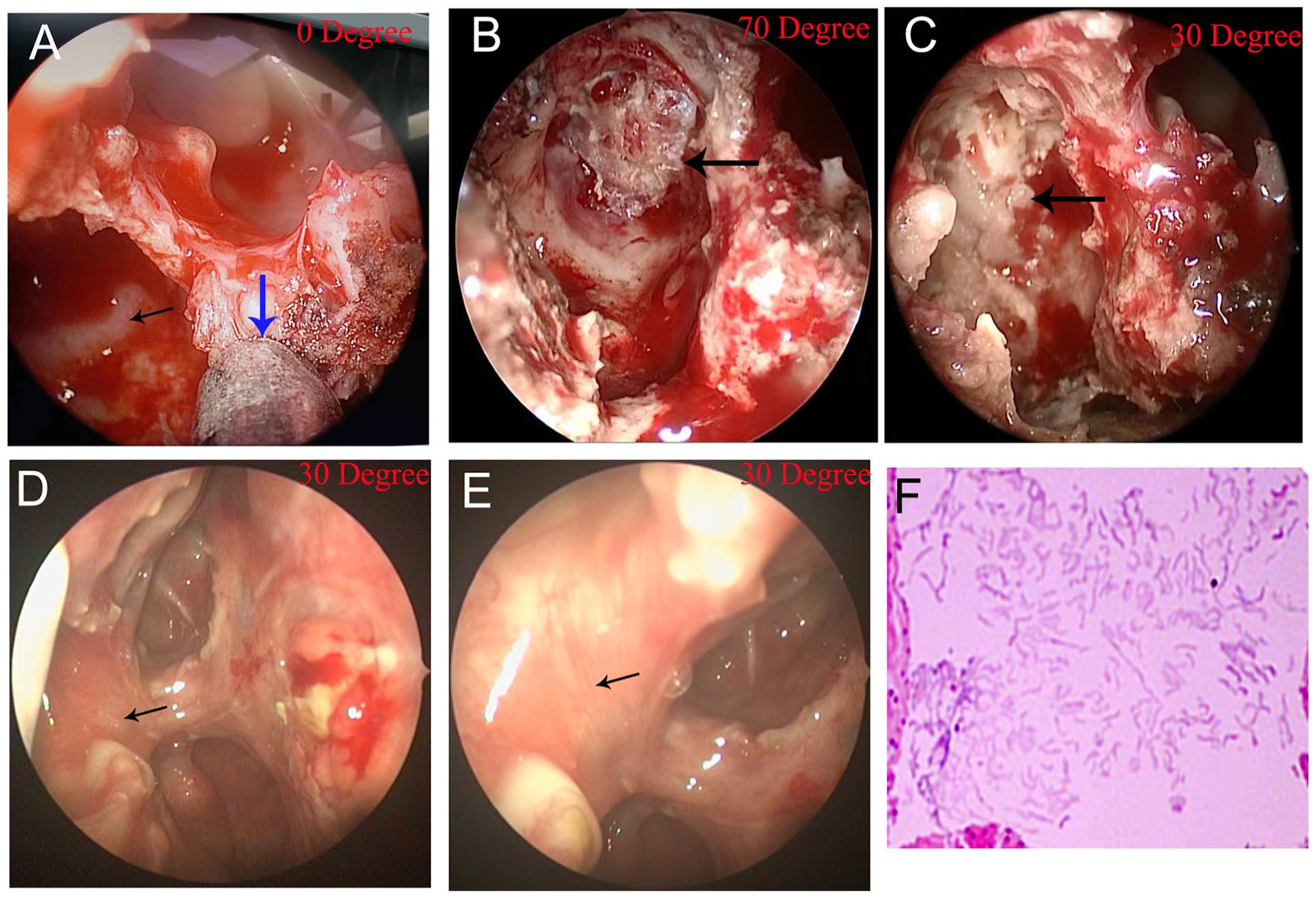
Intraoperative nasal endoscopic view. (A) Under 30° nasal endoscopy, the right pterygoid canal nerve was separated (blue arrow) to localize the sphenoidal pterygoid process root (black arrow); (B) under 0° nasal endoscopy, a yellowish-white epithelioid amorphous lesion was located in the right middle cranial fossa (black arrow); (C) the lesion was completely removed under 70° nasal endoscopy without defect of the endocranium, bleeding, or cerebrospinal fluid leakage (black arrow); (D, E) 6 months after operation, nasal endoscopy showed the mucosa at the lesion site recovered well (black arrow); (F) pathological examination confirmed a cyst filled with keratinous material.
Pathological examination confirmed a cyst filled with keratinous material (Figure 2F). Postoperative nasal endoscopy showed no keratin debris at the site of injury (Figure 2D), and forehead tightness was alleviated. Six months after surgery, follow-up MRI (Figure 1I), and nasal endoscopic examination (Figure 2E) found that the mucosa at the lesion site had recovered well, with no recurrence of the epidermoid cyst.
Discussion
An epidermoid cyst is not a true tumor, but a benign cyst composed of keratinized squamous cell epithelium with a low incidence rate.2,7 Extracranial cholesteatomas are commonly found in the middle ear and mastoid region and are congenital or secondary to trauma or infection due to improper healing or epithelial invasions or invasions.2,7 However, in the field of rhinology, primary epidermoid cysts are unusual and have been rarely reported in the ethmoidal, frontal, and maxillary sinuses.3,4 In this study, MRI showed cystic soft tissue eroding the pterygoid root of the middle cranial fossa, which revealed an amorphous epithelioid in the bone marrow cavity at the root of the pterygoid process with intact endocrine tissue and no epithelioid tissue in the adjacent sinus of the sphenoid. The patient had no history of nasal surgery or head trauma. An epidermoid cyst at the root of the sphenoidal pterygoid process should be differentiated from a brain abscess. However, the latter diagnosis has clear symptoms, such as a history of infection, increased intracranial pressure, and significant focal neurological dysfunction. Furthermore, the pathological results confirmed that the resected tissue was an epidermoid cyst. To our knowledge, this is the first report of a primary epidermoid cyst at the root of the pterygoid process.
Epidermoid cysts usually grow slowly without malignant invasion. However, extracranial epidermoid cysts often compress and destroy the surrounding bones, causing symptoms in the corresponding parts; eventually, when the tumor body is too large, it protrudes into the brain, causing nervous system diseases.1-4 In the present case, the pterygoid sphenoid bone was partially destroyed, but the skull base and endocranium were undamaged. The patient felt only slight tension in the forehead skin. However, the epidermoid cyst located at the root of the pterygoid process was very close to the wall of the right middle cranial fossa. Possible invasion of peripheral tissues, including the base of the middle cranial fossa, sphenoid sinus, and pterygoid process, can cause serious complications. Therefore, it is important to treat epidermoid cysts at the time of diagnosis.
The best treatment for epidermoid cysts is surgical resection based on the MRI characteristics.1-4 In this patient, a soft cystic mass eroded the pterygoid root with hypo-/iso-intense on T1-weighted images, hyperintense on T2-weighted images, inhomogeneous hyperintense on DWI, a slightly low ADC, and no enhancement. These typical MRI characteristics provide superior diagnosis for epidermoid cysts and differentiation from tumors.1-4
Endoscopic resection with the root approach of the pterygoid process is strongly recommended because it allows for the total resection of the tumor under clear vision, with relative simplicity, ease of use, and minimal damage. The key to this operation is to dissect the sphenopalatine foramen to expose the pterygopalatine fossa and pterygoid canal nerve, grind the bone on the lateral side of the pterygoid canal nerve, and thoroughly clean the lesion. Epidermoid cysts have a recurrence rate that can be reduced by extensive and thorough surgical resection. Strict postoperative follow-up is necessary to diagnose recurrence or residual disease early using nasal endoscopy or MRI. We followed up with the patient after 6 months and found no recurrence of the epidermoid cyst on MRI or nasal endoscopy. The tightness of the forehead disappeared 6 months postoperatively.
Conclusions
Epidermoid cysts located at the root of the sphenoidal pterygoid process are rare. Preoperative MRI and CT are necessary for the correct diagnosis and differentiation of other low-growing lesions. Nasal endoscopy is crucial for surgical excision and postoperative follow-up for potential recurrences.
Footnotes
Acknowledgements
Authors’ Contributions
All authors have participated in the production of the manuscript.Consent to Participate.
Consent to Participate
Written informed consent was obtained from the patient for this case report.
Data Availability
All the data have been included in the manuscript and are available upon request from the corresponding authors.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Science and Technology Research Program of Shandong Province (ZR2020MH038) and the National Natural Science Foundation of China (81700891, 81470558, and 81100206).
Ethical Considerations
Ethical approval to report this case was obtained from the Ethics Committee of the First Affiliated Hospital of Shandong First Medical University (approval number 2023-S468).