
Abstract
Cholesterol granulomas are typically identified by their histological features, including cholesterol crystals, giant cells, fibrosis, and inflammation. They occur predominantly in the middle ear, petrous apex, and orbital region, with rare occurrences in the labyrinth. Diagnosis of these lesions is challenging due to their imaging similarities with endolymphatic sac tumors, particularly in preoperative differentiation. In the present case, a 60-year-old woman diagnosed with an endolymphatic sac tumor through preoperative magnetic resonance imaging underwent a transmastoid surgical procedure, and subsequent postoperative histopathological analysis confirmed a cholesterol granuloma. We report this rare case of granuloma confined within the labyrinth, highlighting the importance of radiological and histopathological diagnoses in determining the appropriate therapeutic approach.
Keywords
Introduction
Cholesterol granulomas are histologically characterized by the presence of cholesterol crystals surrounded by foreign body giant cells, fibrosis, and varying degrees of inflammation. They can occur at various anatomical locations, such as the middle ear, petrous apex, and orbital region; however, in rare cases, some cholesterol granulomas have been observed in close association with the labyrinth. 1 The prevalence of cholesterol granulomas confined to the labyrinth is not well-defined, with the existing literature suggesting a relatively low incidence compared to other locations within the temporal bone. Diagnostic challenges arise in the preoperative phase, as differentiating between cholesterol granulomas and endolymphatic sac tumors poses difficulties. This complexity stems from the shared characteristics of both entities, including the manifestation of high intensity on T1-weighted magnetic resonance imaging (MRI) findings. 2 These lesions are often discovered incidentally during imaging studies conducted for unrelated complaints, necessitating a deeper understanding of their clinical significance. In this paper, we describe the imaging characteristics and surgical approach used for a patient with a cholesterol granuloma confined to the labyrinth.
Case Presentation
A 60-year-old woman visited our hospital with left-sided hearing loss that began 10 years ago and left-sided weakness that had occurred intermittently for 6 months. The patient initially visited the neurosurgery department for a brain MRI. Subsequently, owing to the suspicion of an endolymphatic sac tumor, the patient was referred to the otolaryngology department.
Physical examination revealed normal findings on both sides of the tympanic membrane. A pure-tone audiogram showed profound sensorineural hearing loss on the left side. MRI revealed an enhanced irregularly shaped mass located in the endolymphatic sac area measuring 2.0 × 1.5 cm in size. The mass lesion showed a high signal intensity on T2-weighted imaging. Additionally, the lesion displayed a low-to-intermediate signal on T1-weighted imaging, and mild rim enhancement was observed on the enhanced image. The mass involved the left jugular foramen (upper portion), left vestibule, and left posterior semicircular canal (Figure 1). Computed tomography (CT) was performed to assess the mass extension and bone destruction, revealing a permeative lytic lesion with posterior rim calcification in the left petrous temporal bone, involving the vestibular aqueduct.
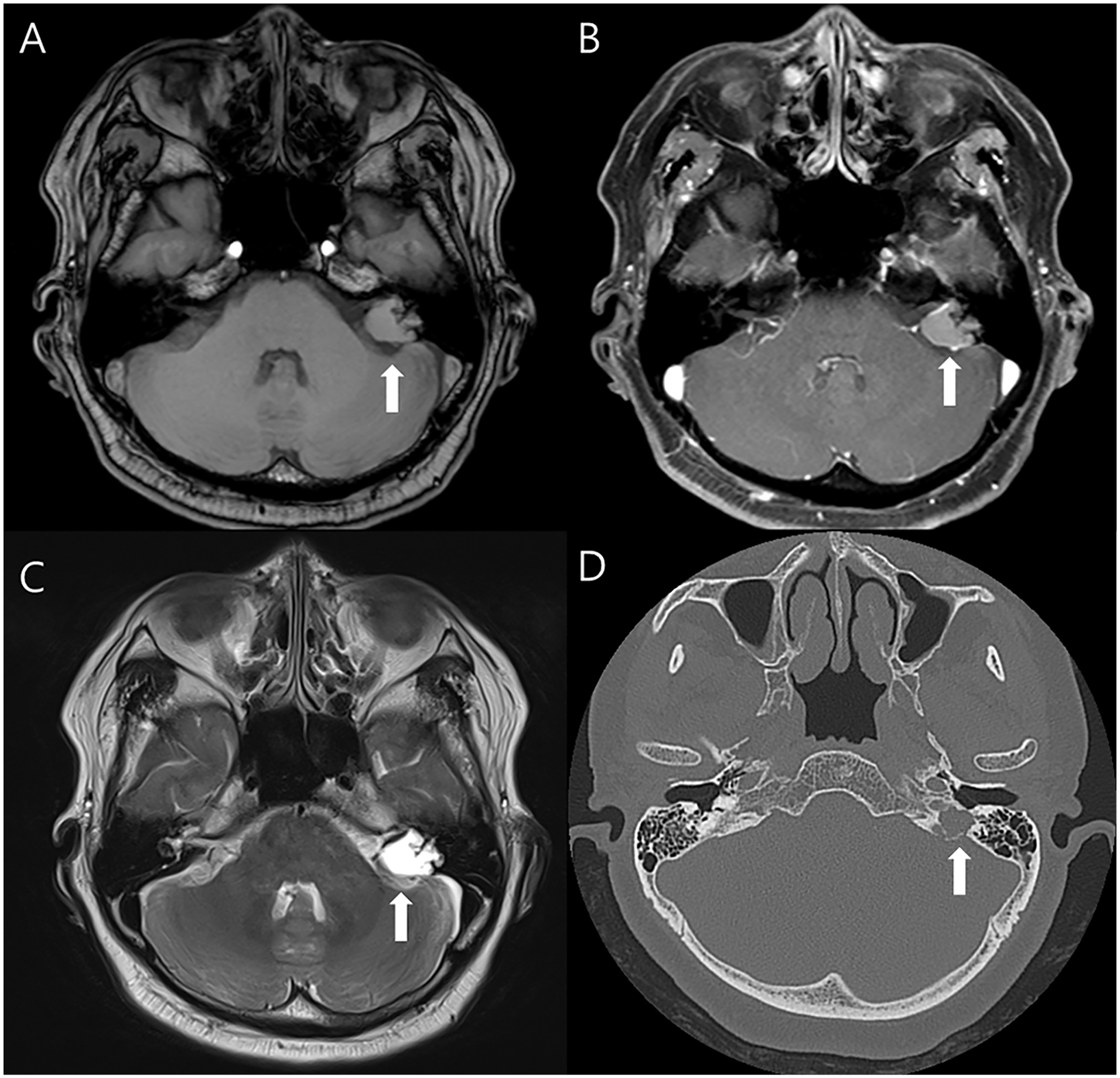
Preoperative (A) T1-weighted, (B) T1-weighted image with gadolinium-enhanced, and (C) T2-weighted magnetic resonance imaging scans showing a 2.0-cm irregularly shaped mass (arrow) in the left petrous temporal bone. (D) Axial computed tomography image showing a permeative lytic lesion (arrow) with posterior rim calcification in the left petrous temporal bone.
Based on the aforementioned findings, surgical resection using the translabyrinthine approach was planned for the diagnosis and treatment of the lesion, considering the possibility of an endolymphatic sac tumor. To rule out glomus jugular, four-vessel angiography was performed to assess the tumor-feeding vessels preoperatively, revealing no discernible tumor-feeding vessels or abnormal vasculature.
The surgical procedure was performed under general anesthesia utilizing a postauricular approach. We performed a mastoidectomy, identified the sigmoid sinus, and dissected the area around the sigmoid sinus using a drill. Using a nerve monitor, we checked the facial nerve tract and drilled it to perform the labyrinthectomy. Preexisting defects were observed in the posterior and lateral semicircular canals. The semicircular canal membrane was exposed, and some serous discharge was aspirated when approached. Fibrotic changes in the membrane were observed in the superior semicircular canal. A labyrinthectomy confirmed that the internal auditory canal was displaced due to the mass cavity. The mass was removed by careful dissection using micro scissors and forceps to avoid damaging the facial nerve. The mass, originating from the endolymphatic sac and extending to the jugular bulb, was successfully removed (Figure 2). Surgery was completed after packing the temporalis fascia and abdominal fat in the tumor removal site. Following surgery, the patient exhibited left facial palsy of House–Brackmann grade III.
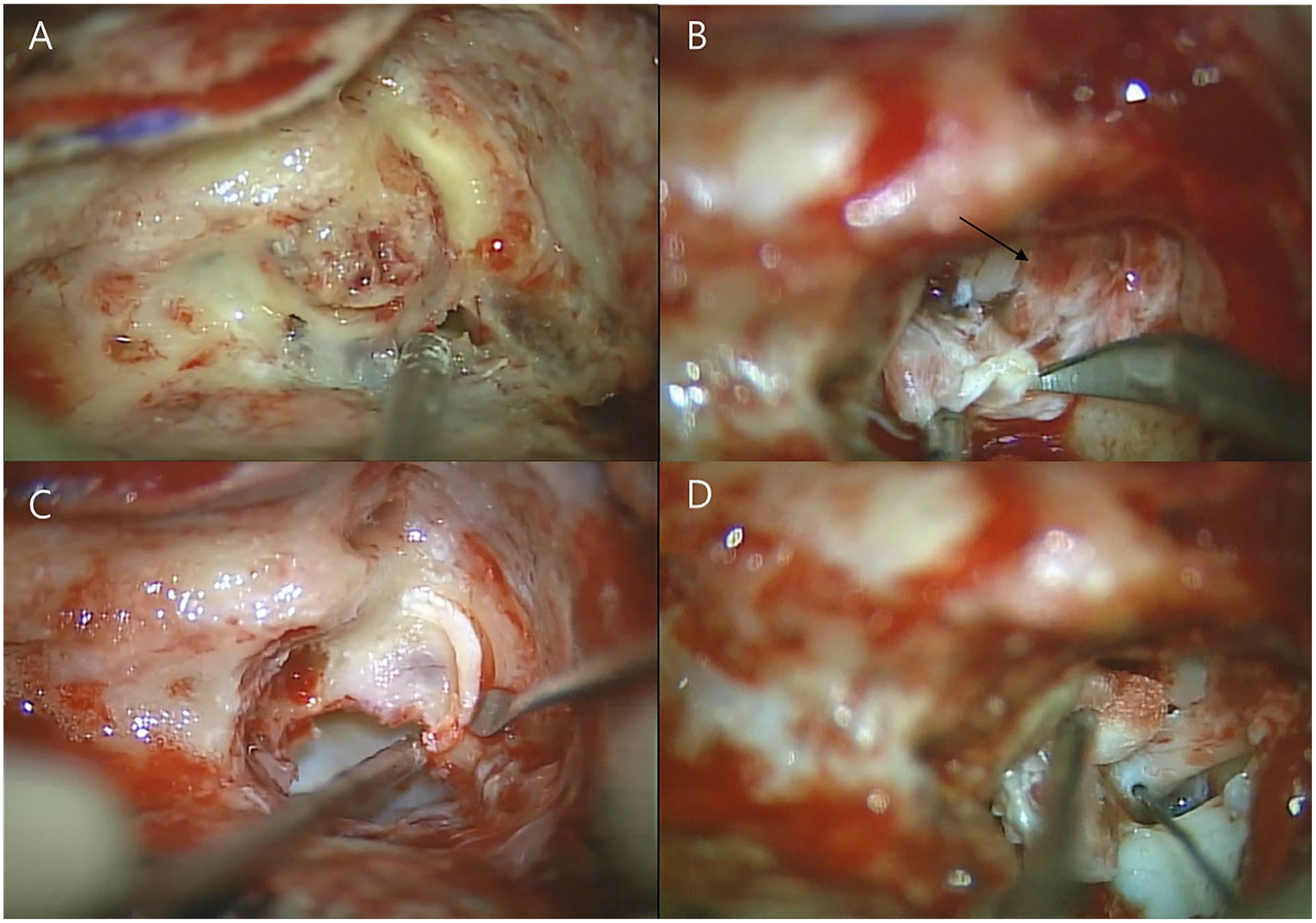
Intraoperative images during cholesterol granuloma removal. (A) Initial exposure of the labyrinthine structure, showing the granuloma. The granuloma appears as a whitish-yellow mass, indicating the presence of cholesterol deposits. (B) Dissection and identification of the facial nerve tract (arrow). Careful dissection is performed to prevent nerve damage. (C) Removal of the granuloma from the semicircular canal. (D) Final inspection of the surgical site after granuloma removal.
Histopathological analysis of the excised mass revealed a cholesterol granuloma with chronic inflammation (Figure 3). Twelve months postoperatively, the patient’s left facial palsy improved to House–Brackmann grade I, with no recurrence detected on the follow-up MRI.
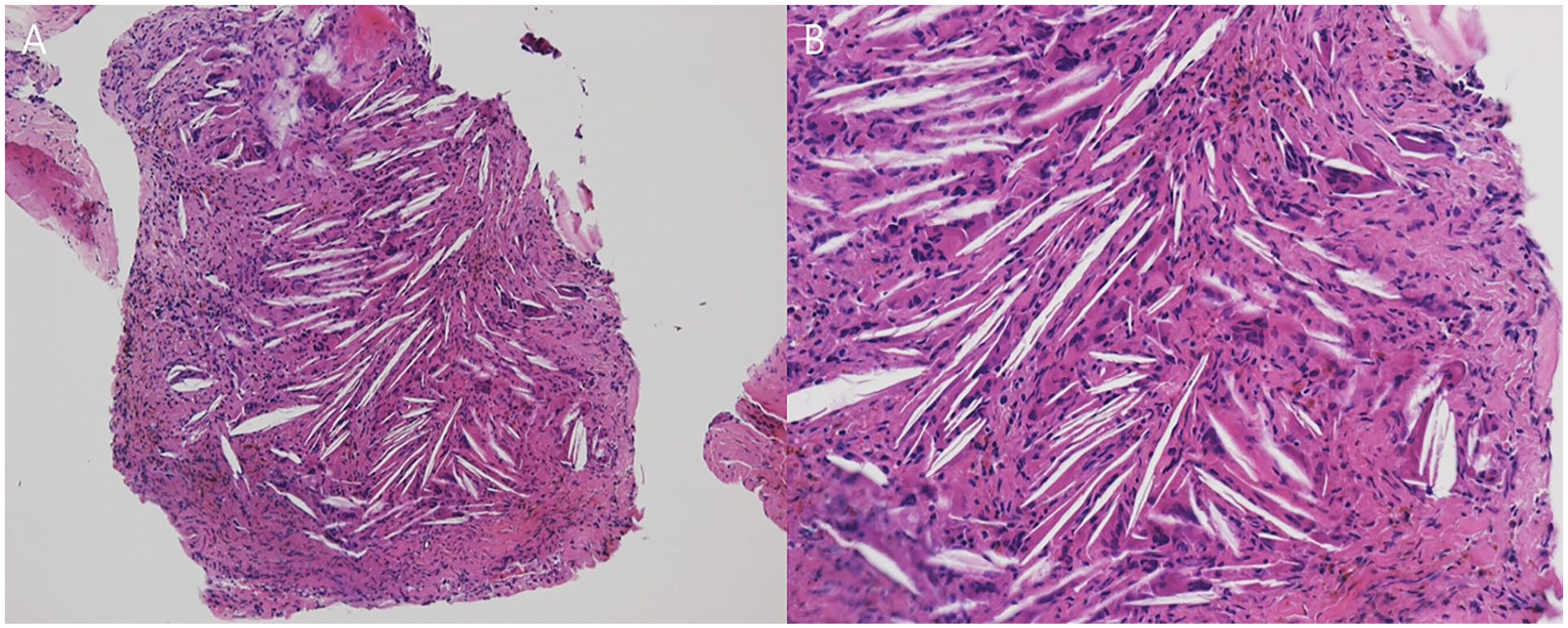
Pathological findings show fusiform clefts created by cholesterol crystals, which are surrounded by multinucleated giant cells.
Discussion
In the present case, initial radiological investigations led to the suspicion of an endolymphatic sac tumor based on the lesion’s location and imaging characteristics; subsequent surgical exploration was performed accordingly. However, postoperative histopathological examination revealed features consistent with those of a cholesterol granuloma, contradicting the preoperative diagnosis. This case underscores the importance of histopathological confirmation, especially in scenarios where imaging findings may not definitively differentiate between cholesterol granulomas and endolymphatic sac tumors.
Cholesterol granulomas most commonly occur in the petrous apex but can also manifest in the middle ear or mastoid area. When they invade the inner ear, they mainly originate from the petrous apex. 3 However, cases where cholesterol granulomas are confined to the labyrinth, as seen in this instance, are exceptionally rare. 4 Precise radiological identification is crucial for the accurate recognition and treatment of cholesterol granulomas. While several conditions resemble cholesterol granulomas, meticulous analysis of radiological signs can reveal unique traits that facilitate an accurate diagnosis. 5
Cholesterol granulomas are characterized by bony trabecular erosion on CT and appear as non-enhancing lesions on MRI, exhibiting high signal intensity on both T1- and T2-weighted sequences due to the paramagnetic effects of hemosiderin. Furthermore, they exhibit high signal intensity on fluid-attenuated inversion recovery MRI and low signal intensity on diffusion-weighted MRI. 5 Cholesteatoma is a major lesion that requires radiological differentiation from cholesterol granuloma. Unlike cholesterol granulomas, cholesteatomas show only high signal intensity on T2-weighted images. Additionally, depending on the site of occurrence, differentiation from endolymphatic sac tumors is also necessary in cases like this one. Endolymphatic sac tumors typically exhibit heterogeneous T1-weighted images with scattered signal areas and peripheral rim enhancement.2,6
The current understanding of cholesterol granuloma pathophysiology is divided into two primary hypotheses; however, a prevailing agreement exists that its formation is primarily due to a foreign body giant cell reaction to cholesterol crystals. The traditional “Obstruction–Vacuum Hypothesis” posits that Eustachian tube dysfunction leads to the generation of negative pressure within the mucosalized spaces, resulting in hemorrhage. Consequently, the accumulation of cholesterol crystals and blood degradation products triggers a foreign body reaction. Subsequently, Jackler and Cho introduced a different hypothesis, the “Exposed Marrow Hypothesis,” which argues that middle ear hemorrhage and hyperpneumatized temporal bones are uncommon in patients with chronic Eustachian tube dysfunction. 7 This hypothesis suggests that blood accumulation within air cells equilibrates the pressure, thereby inhibiting the requisite bleeding for the progression and expansion of a cholesterol granuloma. Furthermore, this alternative hypothesis elaborates on the formation of cholesterol granulomas through osseous dehiscence, allowing contact of bone marrow with pneumatized air cells, thereby providing novel insights into its etiology.
Cholesterol granuloma is a slow-growing, benign, expansive, fluid lesion containing needle-shaped cholesterol crystals with giant cells and fibrous tissue reaction. 8 On histological examination, a cholesterol granuloma appears as a lymphocytic–histiocytic cellular infiltrate with abundant mononuclear cells. In addition to cholesterol, these cells comprise giant multinucleated cells, erythrocytes, or macrophages containing hemosiderin. 9 The cyst wall comprises fibrous connective tissue and lacks the keratinizing squamous epithelium observed in cholesteatomas. 10
Unlike cholesterol granulomas, cholesteatomas are keratinized multilayered formations of squamous epithelium containing desquamated keratin and characterized by aggressive enzymatic activity toward the underlying bone tissue owing to proteolytic enzymes, including elastase, trypsin-like proteinases, kallikrein, urokinase-type proteinase activator, and cathepsin B.9,11 In contrast, endolymphatic sac tumors are characterized as low-grade, locally invasive, highly vascularized, and having indistinct margins. Microscopically, these tumors exhibit two main patterns: papillary and follicular. The papillary configuration is identified by the arrangement of cuboidal or low columnar epithelial cells into papillary structures, while the follicular pattern displays cystic formations filled with protein-rich fluid, similar to those found in thyroid follicles.12,13
In cases where symptoms are present in patients with cholesterol granuloma, surgical management is recommended, whereas asymptomatic patients are typically advised to undergo nonsurgical management. The surgical management of cholesterol granulomas is primarily performed through the translabyrinthine, infralabyrinthine, middle fossa, transsphenoidal, or, more commonly, infracochlear approach. The primary objective of these procedures is to establish a permanent drainage pathway to prevent the onset or worsening of symptoms due to the expansion of the cholesterol granuloma. 5
The leading cause of recurrence is the obstruction of the drainage pathway by fibrous tissue, a complication that can occur with any surgical technique. 7 Therefore, comprehensive long-term clinical and radiographic follow-up is essential for all patients. Scheduled temporal bone CT scans, initiated 1 year postoperatively, are instrumental in monitoring cyst reduction and the presence of aeration. Although a decrease in cyst size and the presence of aeration are favorable indicators of the treatment’s long-term success, the absence of aeration should not be interpreted as an outright failure of the intervention. 14 Additionally, cases exist where patients who underwent transmastoid surgery to remove lesions presumed to be cholesterol granulomas relapsed with endolymphatic sac tumors 2 years postoperatively. Therefore, even if lesions such as cholesterol granulomas or endolymphatic sac tumors are not detected on MRI up to 12 months postoperatively, long-term follow-up of at least 24 months is necessary. 15
Distinguishing cholesterol granulomas from endolymphatic sac tumors is essential for accurate diagnosis and optimal treatment planning. Our case highlights the need to recognize the limitations of accurate differentiation in radiological evaluation and surgical approaches with various possibilities in mind. A thorough understanding of the radiological disparities and common areas of involvement is vital for guiding clinical decision-making in such challenging cases.
Footnotes
Acknowledgements
None.
Author Contributions
Dae-Yang Kim: Data acquisition and writing of the original draft. Hyun Jin Lee: Performed the surgery, and edited and revised the manuscript.
Availability of Data and Materials
The data used to support the findings of this study are available from the author or corresponding author on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) [NRF-RS-2023-00210073] to H.J.L.
Ethical Statement/Patient Consent
This study was approved by the Institutional Review Board of the authors’ institute (IRB number: OC24ZISI0069), and the requirement for informed consent from the patient was waived. A patient’s anonymity is preserved in the manuscript.