
Abstract
Cholesterol granulomas are rare cystic inflammatory lesions characterized by the formation of cholesterol crystals. They are the most prevalent lesions of the petrous apex and when symptomatic, hearing loss, vertigo, tinnitus, headache, and facial pathology can be present. Surgical management is recommended in symptomatic patients. There are different surgical approaches to cholesterol granulomas. The aim of this article is to present and describe an endoscopic endonasal nasopharyngeal approach to a cholesterol granuloma and explain the advantages and disadvantages.
Introduction
The petrous apex is the most medial portion of the temporal bone and has a pyramid-shaped structure. 1 Disease involving the petrous apex is uncommon but if present, it is a challenge to manage due to the presence of near critical structures such as the cochlea, intratemporal carotid artery, jugular bulb, and eustachian tube. 2 Lesions of the petrous apex are often silent, and cholesterol granulomas are the most prevalent pathology, representing 40% of all the benign lesions found. 3
Cholesterol granulomas are rare cystic inflammatory lesions characterized by the formation of cholesterol crystals. These lesions are secondary to chronic obstruction of air cells within the petrous pyramid and appear in pneumatized petrous portions of the temporal bone, pneumatized in 30% of the population. 3 -5 Jackler and Cho introduced a new theory that gained greater acceptance related to the pathophysiology of cholesterol granulomas. They defend that pneumatized petrous apex exposes marrow-filled spaces, and this relationship produces a tendency to hemorrhage. This results in obstruction of the petrous apex outflow tract. 6 Cholesterol granulomas are often asymptomatic but, when symptomatic, they often present with hearing loss, vertigo, tinnitus, headache, and facial pathology. 6 Unilateral serous otitis can occur, causing eustachian tube dysfunction. 7 Surgical management is recommended in symptomatic patients, and different approaches have been described to access the petrous apex, such as open, endoscopic, and combined techniques categorized into anterior, lateral, and posterior. 8 The aim of this article is to present and describe an endoscopic endonasal nasopharyngeal approach to a cholesterol granuloma and its outcomes.
Case Report
A 27-year-old woman with Von Willebrand disease and neurofibromatosis type I was sent for an Otorhinolaryngology appointment because of a cholesterol granuloma on the left petrous apex. The pathology was incidentally discovered through magnetic resonance imaging (MRI), performed as a neurofibromatosis follow-up. The otoscopic examination showed a blue eardrum on the left ear with a mild conductive hearing loss. Later, during follow-up, there was a sudden onset of peripheral facial paralysis and worsening of the left ear sensorineural hearing. A new MRI was performed and showed a lesion with 25 × 20 × 27 mm in the left petrous apex with high signal on T1- and T2-weighted images without evidence of bone erosion; molding of the left internal auditory canal along with the membranous labyrinth; a high T2 signal in the middle ear and left mastoid related to tube dysfunction and a normal internal carotid caliber (Figure 1). An audiologic evaluation revealed a mixed hearing loss on the left side, with an air-bone gap of 40 dB in all frequencies and a pure tone average of 105 dB and a type B tympanometry (Figure 2).
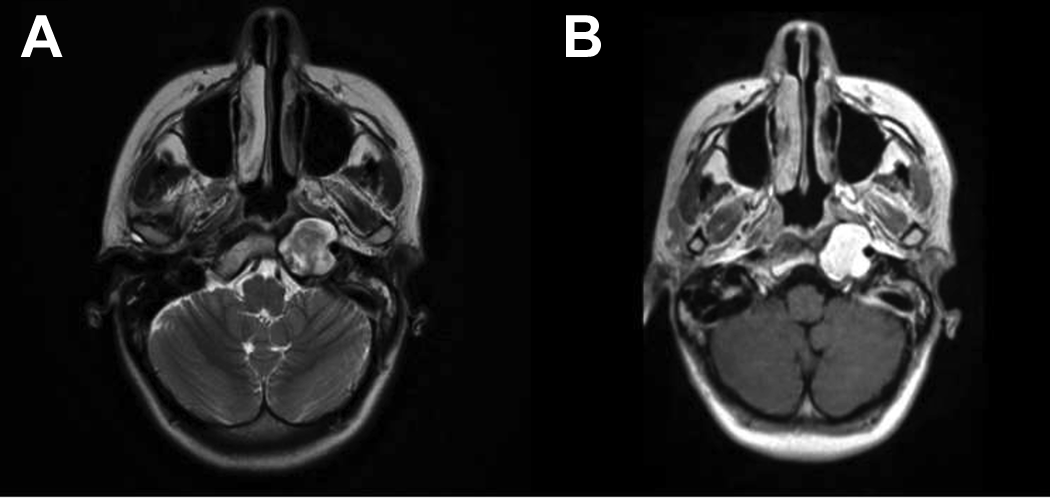
(A) and (B) are T2- and T1-weighted, respectively, magnetic resonance imaging (MRI) images demonstrating an expansile lesion in the left petrous temporal bone.
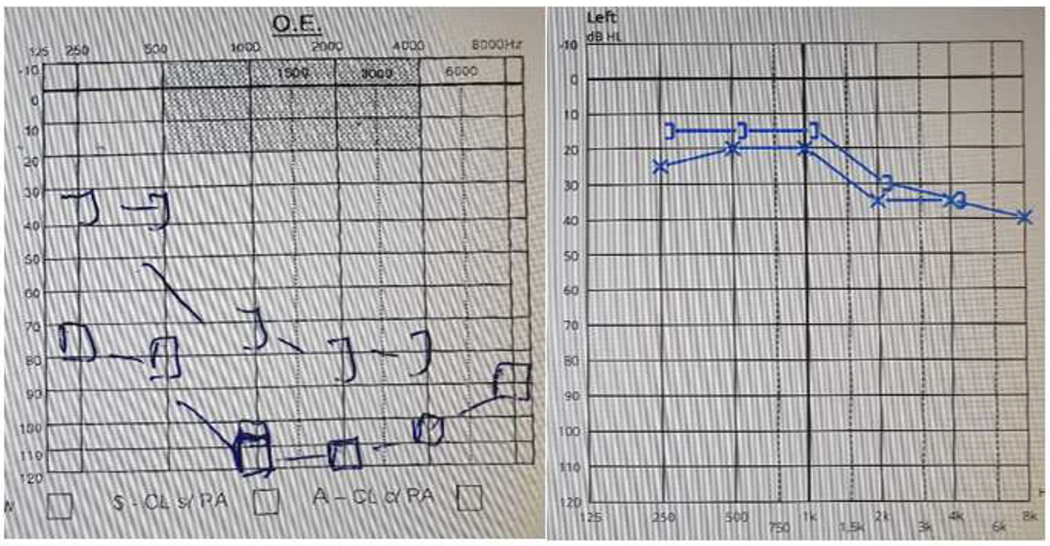
Audiologic evaluation before and after surgery.
After assessing the location of the lesion, an endoscopic approach by nasopharynx was decided. An incision on the left fossa of Rosenmuller was performed, followed by dissection until reaching the granuloma capsule. A nasoseptal flap was executed and placed around the granuloma cavity opening and a silastic drainage stent was positioned (Figure 3). One month after the surgery, the patient recovered from peripheral facial paralysis and hearing loss (Figure 2). At 1-year follow-up, the mucosa of the nasopharynx had healed completely, and there is no evidence of recurrence and a drainage pathway for the granuloma remained.
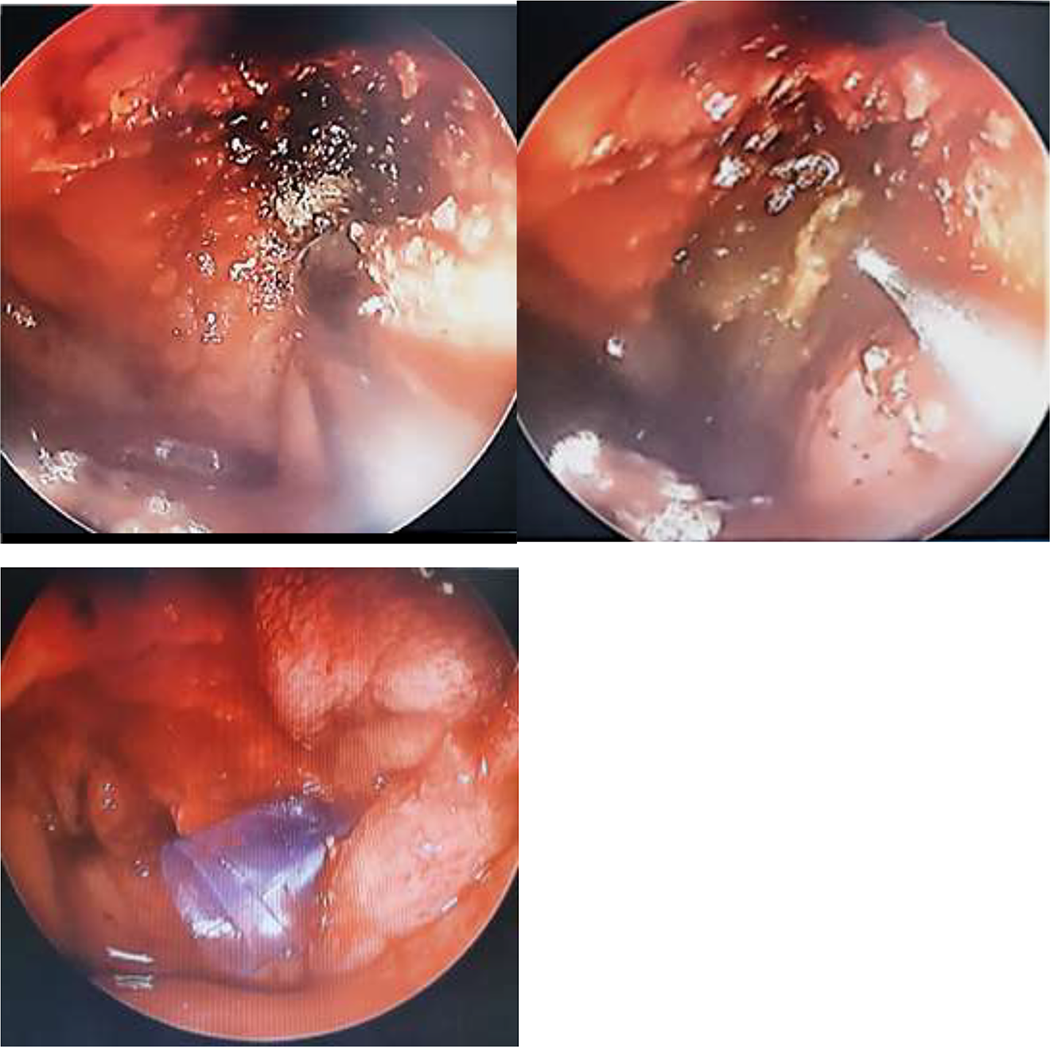
Intraoperative images.
Discussion
Primary petrous apex lesions, like cholesterol granulomas, are very often asymptomatic and rare so, diagnosis is usually late. 9 When cholesterol granulomas become large enough, the symptoms start to appear, especially due to the compression of cranial nerves and middle ear involvement.
In these cases, the best treatment is surgical drainage and the establishment of a pathway to avoid future recurrence. 4 There are different surgical approaches to cholesterol granulomas, such as transtemporal (further subdivided in infralabyrinthine, infracochlear, transcochlear, and translabyrinthine), middle fossa, or endonasal (transsphenoidal, transnasopharyngeal/transclival) approaches. 3 The best surgical approach choice should be based on symptoms, size, location, and position of vital structures and surgeon’s experience.
In this case, an endoscopic endonasal approach was selected through the superior nasopharynx, due to the lesion location. The advantage of this approach, comparatively to others, is being a low morbidity procedure with good access. The follow-up is simple, consisting of nasal endoscopy and imaging, but is important to pay attention to early signs of restenosis and, if necessary, remove the scar tissue, to reestablish drainage. 7
The petrous apex remains an area of difficult and challenging access. However, with multiple approaches, it is important to choose the best option. With this case, we aimed to report a possible, but less described surgical approach to cholesterol granuloma. This method provides good access to the lesion in selected cases.
Footnotes
Authors’ Note
The present study was approved by the Ethics Committee at Centro Hospitalar Universitário do Porto. The authors declare that all procedures were performed in line with the regulation established by the heads of Clinical and Ethical Research Committee, and in accordance with the Helsinki Declaration of the World Medical Association. Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.