
Abstract
Since the introduction of effective chemotherapy, the development of new diagnostic tools, and raising public awareness of the devastating health, social, and economic consequences of tuberculosis (TB), the frequency of this disease has decreased. Pulmonary TB is the most common form of the disease, but TB bacilli can spread to other organs including lymph nodes, and the oral cavity especially the tongue with very unusual features. Oral lesions, although rare, are very important for early diagnosis and interception of primary TB. The bacteriological and histopathological results are important to confirm the diagnosis. Oral TB lesions may be either primary or secondary. The evolution is generally good under a medical treatment. A 35-year-old patient was admitted to our department for an ulcerous tumor in the lateral border of his tongue. The biopsy of the ulceration confirmed the diagnosis of TB. A concomitant pulmonary localization has been found. This case report aims to attract the attention of TB, which can be located in some uncommon regions, and have unusual clinical presentations.
Introduction
Pulmonary tuberculosis (TB) is the most common form of TB. Extrapulmonary involvement occurs in 10% to 15% of cases, including rare cases of oral TB that represent 0.05% to 5% of patients with TB and can be the first sign of the disease.1,2 In Tunisia, TB is still endemic, the differential diagnosis of TB must be considered in ulcerated lesions to have an early diagnosis.
Clinical Observation
A 35-year-old man with no medical history, except smoking, consulted our department for a painful ulceration of the lateral border of the tongue that had been first noticed 2 months earlier. There was no improvement in symptoms with medical treatment based on antibiotics and mouthwashes.
Careful questioning revealed that there was a history of a persistent cough with a prolonged fever, usually nocturnal, with weight loss and asthenia.
On examination, the patient was thin (body mass index = 17). Oral examination revealed an ulceroproliferative, rough, irregular-shaped ulcer on the right border of the tongue measuring 2 cm × 2 cm in size that extends anteriorly 1 cm from the tip of the tongue and laterally extends up to the margins of the tongue. The base of the ulcer appeared to be granular. The margins of the ulcer were slightly elevated and indurated. The ulcer was surrounded by a small area of erythema, which was painful to the touch (Figure 1). The oral condition was poor with multiple dental caries. Examination of the cervical region did not reveal adenopathy. Nasofibroscopy was performed and no additional lesions of the upper airway tract were found.

Oral examination revealed: an ulceroproliferative, rough, irregular-shaped ulcer on the right border of the tongue. The base of the ulcer appeared to be granular. The margins of the ulcer were slightly elevated. The ulcer was surrounded by a small area of erythema.
Blood tests did not show abnormalities except mild hypochromic microcytic anemia (hemoglobin 11.1 g/dL). The tuberculin screening test was positive (red, indurated area measuring 12 mm). Routine urinalysis was normal. Serological tests for hepatitis B virus, hepatitis C virus, human immunodeficiency virus, and syphilis were negative. The search for TB mycobacterium in the sputum was positive.
The chest radiograph showed left micronodular opacity with an alveolar interstitial infiltrate of the lung apices, confirmed by a chest computed tomography scan (Figure 2).

Chest X-ray showed a left micro-nodular opacity with an alveolar-interstitial infiltrate of the lung apices.
A deep tongue biopsy was performed. Pathological examination revealed an epithelioid and gigantocellular granuloma with caseous necrosis. These features were consistent with a diagnosis of TB (Figure 3). Acid-fast bacilli were found in sputum and tongue sections when the tissues were stained by the Ziehl–Neelsen method. The diagnosis of oral TB with concomitant pulmonary localization was made, and the patient started immediately on a daily medication: quadruple anti-TB chemotherapy (isoniazid, rifampicin, ethambutol, and pyrazinamide) for 2 months, then dual therapy for 4 months. He has been followed monthly, and his pain and ulcerated lesion of the tongue improved rapidly.
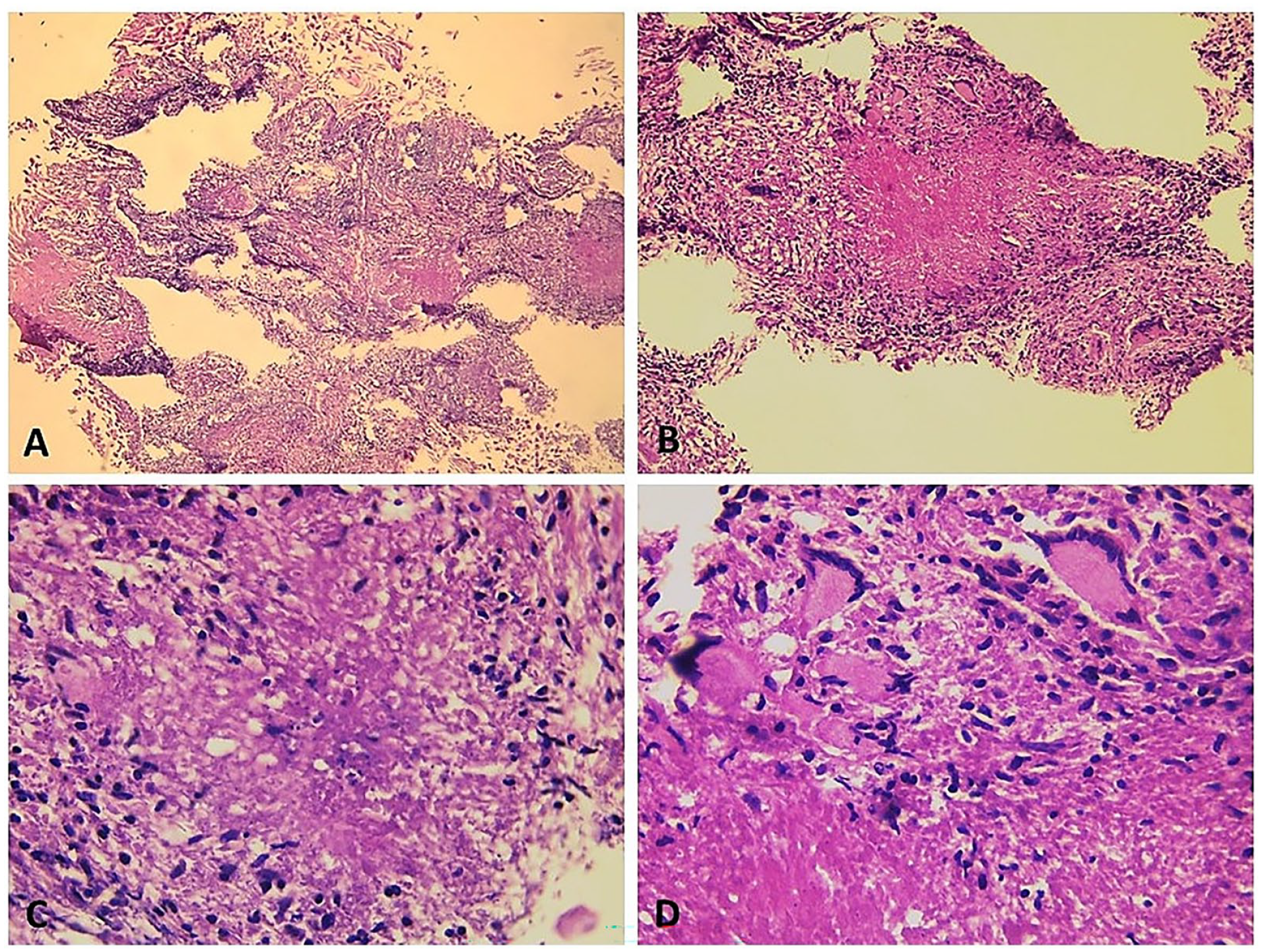
(A) (HE, ×40) and (B) (HE, ×100): Biopsy specimen obtained from the tongue lesions showing necrotizing granulomatous inflammation within the lingual mucosa (chorion). This inflammation is made by multiple granulomas composed of a central necrotic zone, which is surrounded by epithelioid histiocytes (C: HE, ×400) with varied numbers of multinucleated Langhans type giant cells and lymphocytes (D: HE, ×400). These features are consistent with TB. HE, hematoxylin and eosin; TB, tuberculosis.
Discussion
Since the introduction of effective chemotherapy, the development of new diagnostic tools, and raising public awareness of the devastating health, social, and economic consequences of TB, the frequency of this disease has decreased. TB is a mycobacterial infection that preferentially affects the respiratory tract, but can affect many other organs in almost a third of cases. Diagnosis is often difficult and late.
The involvement of the oral cavity was observed in 0.2% to 1.5% of TB cases.1,2
In addition to the palate, other sites could be included, such as the tongue, the floor of the mouth, the gums, and the lips. 3
Chronic irritation or inflammation of the mucosa may be favorable for TB of the tongue. Other predisposing factors include poor dental hygiene, dental extraction, and smoking.1,4,5
Oral involvement typically coexists with pulmonary diseases as a manifestation of a secondary form of the infection that was noticed in our patient who presented concomitant pulmonary localization. Contamination occurs directly through the inhalation of microdroplets of infected saliva or from a site of pulmonary TB. 6
The clinical manifestations are not specific, sometimes misleading other pathologies. 7
The diagnosis, suspected clinically, usually takes the form of ulceration, with irregular margins and a slightly indurated base, while in our case, the clinical appearance of the ulcer was of the ulceroproliferative type, and the margins were indurated. 6 Other clinical features may be found such as a nodular tumor-like mass, a fissure, a tuberculoma, a cold abscess, or diffuse glossitis.2,8–9
This localization is frequently associated with significant impairment of general health as a result of the eating disorders and weight loss that they cause.
Differential diagnoses to be considered are traumatic lesions, viral infections (viruses of the herpes group and HIV), bacterial infections (syphilis), deep fungal infections, and systemic diseases, such as Behçet’s, Crohn’s, and Wegener’s diseases.4,6,10,11
The diagnosis requires a histological examination that shows an epithelioid granuloma with caseous necrosis.6,7 This aspect was similar to our histological findings.
A chest radiological examination and a Mantoux skin test are mandatory to rule out pulmonary TB.
Anti-TB treatment leads to an improvement with rapid healing of the ulceration and an improvement in general condition. It consists of a medical treatment that contains 2 phases: for the first 2 months, the treatment consists of a daily dose of isoniazid, rifampicin, pyrazinamide, and ethambutol. During consolidation that lasts at least 6 months, it involves a daily dose of isoniazid and rifampicin. Once treatment begins, clinical symptoms subside in a few days, while lesions improve after a few weeks.4,9,12
This case highlights the importance of considering TB infection in the differential diagnosis of nonhealing oral lesions, especially when a suggestive epidemiological context was found in the patient’s history.
Conclusions
A large variety of extrapulmonary localizations of TB have been described. Lingual localization is rare and is more frequently secondary to pulmonary involvement. The diagnosis should be suspected in the presence of a persistent and atypical oral lesion. Detecting the disease early leads to a better prognosis for the patient.
Footnotes
Authors’ Note
Mehdi Hasnaoui, Mohamed Masmoudi, and Azer Chebil have prepared the manuscript. Sameh Jebahi has prepared and formatted the image. Khalifa Mighri and Seifeddine Ben Hammouda performed the procedure, edited, and approved the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
The data used to support the results of this study have received hospital ethical approval for use.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was conducted with the approval of the Clinical Research Ethics Review Committee of Tahar Sfar University Hospital
Informed Consent
A written informed consent was also obtained from the patient to publish this report in accordance with the journal’s patient consent policy.