
Abstract
Pulmonary fungal balls are caused by long-term fungal infection of the lung. They are sometimes a complication of previous cavitary pulmonary tuberculosis. Pulmonary fungal balls caused by Trichophyton are extremely rare. A 65-year-old man who worked in a leather recycling factory was admitted because of a productive cough and shortness of breath. He had a history of tuberculosis with lung destruction. A chest radiograph showed an opacity surrounding an air lucency over the left lung field, and chest computed tomography showed a mass within a cavity, producing a ball-in-hole appearance, over the left upper lung lobe. Bronchoalveolar lavage was performed, and fungal culture of the lavage fluid yielded Trichophyton. After 6 months of treatment with oral itraconazole, the patient’s general condition improved. This case emphasizes the importance of awareness of fungal infection within cavitary lesions of the lung and shows that Trichophyton may be the etiologic organism in such cases. Itraconazole is a recommended treatment of pulmonary fungal balls.
Introduction
Pulmonary fungal balls are caused by chronic fungal infection of the lung and often develop within pre-existing cavities caused by tuberculosis and other conditions. The fungal ball contains fungal material, inflammatory cells, and tissue debris within the pre-existing lung cavity. 1 Symptoms are variable and range from asymptomatic to life-threatening. The most common pathogen of pulmonary fungal balls is Aspergillus, and such fungal balls are called aspergillomas. 2 Trichophyton is a very rare pathogen of pulmonary fungal balls, and only one case has been reported to date. 3 We herein report the second case of a pulmonary fungal ball due to Trichophyton.
Case report
A 65-year-old Chinese man who worked in a leather recycling factory was admitted because of a 3-month history of a productive cough and shortness of breath. He also had a history of tuberculosis 10 years previously with resultant lung destruction.
Physical examination revealed coarse crackles over the left lung. Laboratory data showed a white blood cell count of 13,500/µL with 80.3% neutrophils, 9.2% lymphocytes, and 6.6% monocytes; other findings were within normal limits.
A chest radiograph showed a large opacity over the left hilum with an air bronchogram surrounding a crescentic air lucency. Reticulation with multiple cystic formations was observed over the left lower lobe, and extensive pleural thickening was present (Figure 1). Chest computed tomography showed a mass within a cavity, producing a ball-in-hole appearance, over the left upper lung lobe (Figure 2).

Chest radiograph showed a large opacity over the left hilum with an air bronchogram surrounding a crescentic air lucency (arrow). Reticulation with multiple cystic formations was observed over the left lower lobe, and extensive pleural thickening was present.
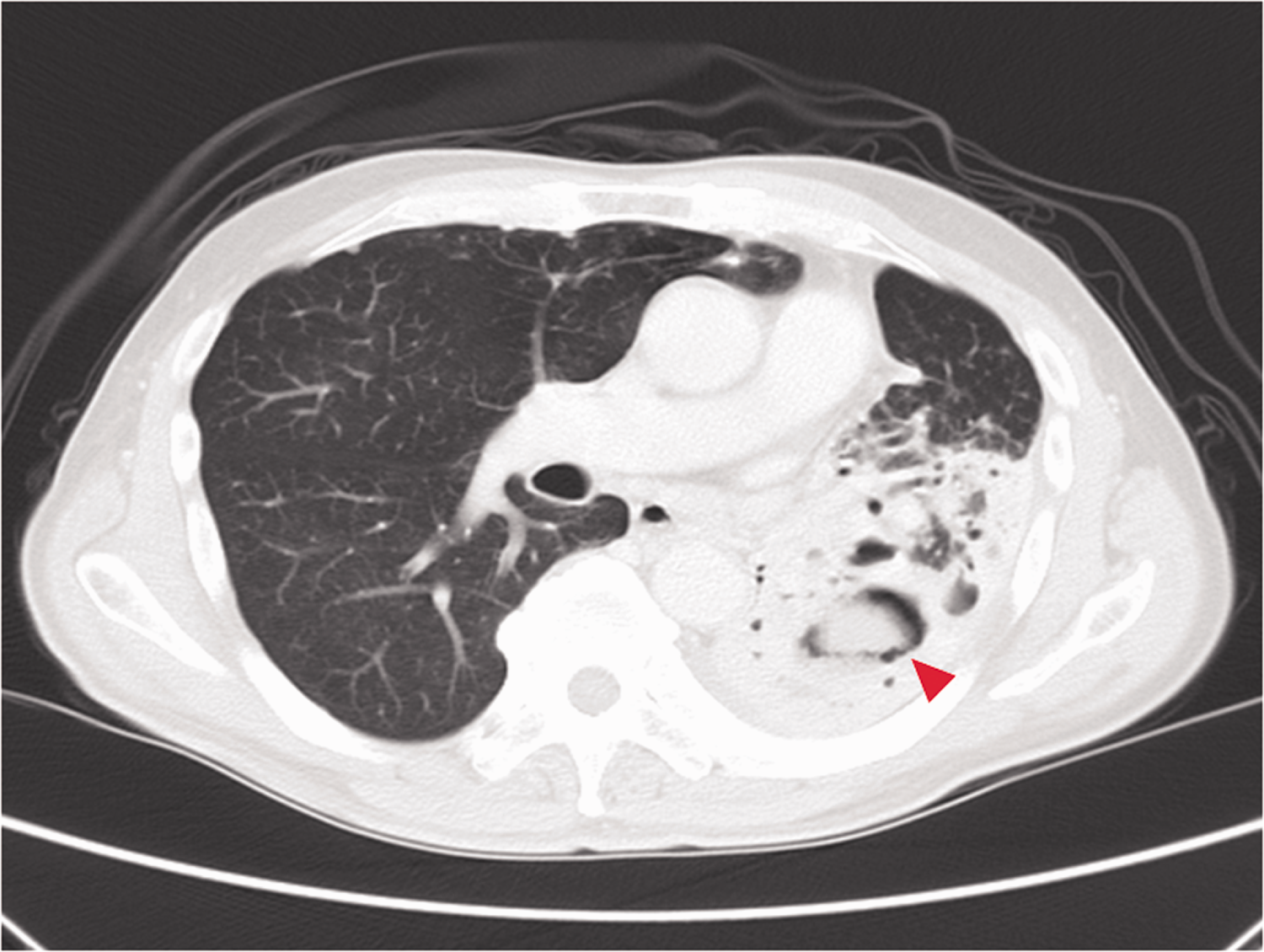
Chest computed tomography showed a mass within a cavity, producing a ball-in-hole appearance (arrowhead), over the left upper lobe.
The patient underwent bronchoalveolar lavage with normal saline, and fungal culture of the lavage fluid yielded Trichophyton. Three rounds of acid-fast staining were performed, but the results were negative. About 2 months later in the outpatient department, tuberculosis culture yielded no tuberculosis pathogen growth. After 6 months of treatment with oral itraconazole at 200 mg daily, the patient’s productive cough and shortness of breath were gradually ameliorated, the coarse crackles were reduced, and the onychomycosis of his toes resolved.
Discussion
Occasionally, the term “pulmonary mycetoma” is erroneously used to refer to a pulmonary fungal ball. However, a mycetoma refers to a subcutaneous fungal infection; pulmonary fungal balls should not be referred to as mycetomas.
Pulmonary fungal balls usually develop in a pre-existing cavity using caused by tuberculosis, bronchial cysts, bronchiectasis, a neoplasm, or a pulmonary infection.2,4 Fungal balls and ball-in-hole lesions have occasionally been described. 3 Data on the exact incidence of pulmonary fungal infection in Taiwan are not available. Chen et al. 5 reported an increasing annual incidence of pulmonary fungal infection during a 10-year period in National Taiwan University Hospital. Aspergillus is the most common pathogen of pulmonary fungal balls, and such fungal balls are called aspergillomas. 2 Fungal balls caused by Nocardia asteroides, Allescheria boydii, Candida albicans, Streptomyces, and Mucorales have also occasionally been described. 3 Weese and Helms 3 reported the first case of a pulmonary Trichophyton fungal ball in 1973. Our case is the second reported case of a pulmonary fungal ball due to Trichophyton.
Rapid diagnosis and accurate identification of the causative organisms is important for proper treatment of pulmonary fungal balls. The diagnosis is usually made clinically in endemic areas. A definitive diagnosis is often made by grain examination (morphological features, size, color, and consistency), microscopy (cytological and histopathological examinations), imaging (radiography, ultrasonography, computed tomography, or magnetic resonance imaging), and cultures as well as by molecular-based techniques such as polymerase chain reaction amplification and sequencing analysis for causative organisms.6–8 Various serological tests may be used; however, no reliable test exists.6,9 Fungal culture is still the most important method for the diagnosis of pulmonary fungal balls. 10 The diagnosis in our case was based on a combination of the patient’s clinical history (previous tuberculosis and worker in a leather recycling factory), imaging (cavitary lesion on a chest radiograph and ball-in-hole lesion on chest computed tomography), and microbiological confirmation of the Trichophyton pathogen by bronchoalveolar lavage and culture.
Treatment of fungal balls is often unsatisfactory and associated with a low cure rate and high recurrence rate; in addition, treatments are expensive and difficult to maintain because of the prolonged course of the disease.7,10,11 Identification of the causal microorganism is important to guide the treatment, and the treatment should be designed to decrease the pathogen load. 9 A combination of surgical excision and antifungal agents is currently recommended as the standard treatment for pulmonary fungal balls. 11 Itraconazole at 200 to 400 mg/day is recommended as the drug of choice to treat pulmonary fungal balls because of its low toxicity and few adverse effects; however, the treatment duration is long.9,10 Because of the avascular nature of pulmonary fungal balls, intravenous antimicrobials may provide less therapeutic benefit. Instead, adequate saline lavage either by percutaneous pigtail drainage or bronchoalveolar lavage might be an effective alternative therapy. 12
In our case, after 6 months of oral itraconazole treatment, the patient’s productive cough and shortness of breath were gradually ameliorated; the coarse crackles also decreased. This outcome reconfirms that itraconazole, despite its long treatment duration, still is the treatment of choice for pulmonary fungal balls.
Awareness of this disease is needed for early diagnosis and proper treatment, which will help to reduce its high morbidity and improve patient outcomes. This case highlights the importance of awareness of fungal infection in cavitary lesions of the lung and shows that Trichophyton may be the etiologic organism. Itraconazole is recommended as the treatment of choice; however, an effective and safe antifungal with a short treatment duration is urgently needed.
Footnotes
Acknowledgement
We would like to thank Fang-Ching Yeh, a microbiologist, for providing us with information regarding Trichophyton.
Availability of data and materials
The information used during the current report is available from the corresponding author on reasonable request.
Authors’ contributions
HLL collected the data and wrote the manuscript. CCC checked the figures. GLC and LMC revised the manuscript. All authors approved the final version of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The study protocol was approved by the institutional review board of Tri-Service General Hospital (approval number C202105155). Written informed consent was obtained from the patient for treatment and publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor-in-chief of this journal. The reporting of this study conforms to the CARE guidelines. 13
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.