
Abstract
Keywords
Introduction
There are several causes of conductive hearing loss in children, one of which is congenital malformations of the ossicular chain. This cause usually involves 1 or more auditory bones and has an incidence rate of 0.28/100,000. 1 Moreover, these malformations can be associated with external and inner ear malformations, resulting in varying degrees of hearing loss and challenges with hearing, language development, and social adaptability. Surgery is the primary treatment for congenital ossicular chain malformations in children. There are few case studies on auditory intervention decisions for different auditory malformations, with case reports predominating. Despite improvements in diagnostic imaging technology, it continues to be a challenge for clinicians to make the preoperative diagnosis and choose the surgical treatment plan. Therefore, in this study, we analyzed the surgical treatment and curative effect in 8 cases (10 ears) of congenital ossicular chain malformation retrospectively to provide guidance for the clinical treatment of congenital ossicular chain malformation in children. In our conclusions, we acknowledge a certain rate of preoperative imaging examination inaccuracies and emphasize the importance of selecting advanced treatment plans tailored to different types of congenital ossicular chain malformations.
Materials and Methods
Clinical Materials
From October 2019 to October 2022, 8 cases from the Department of Otorhinolaryngology-Head and Neck Surgery, Beijing Children’s Hospital were reviewed, including 5 cases of bilateral and 3 cases of unilateral congenital ossicular malformation. A total of 10 ears were treated by surgical intervention; in 3 cases of bilateral ear disease, only 1 ear was treated. There were 6 males and 2 females, aged from 5 years 9 months to 12 years 8 months, and the median age was 8.5 years. All children had no other systemic diseases and were followed for 6 months to 2 years. The investigations were carried out following the rules of the Declaration of Helsinki of 1975, revised in 2013. This study was approved by the Ethics Committee of Beijing Children’s Hospital. Ethics (Clinical Research) Review Number: [2023]-E-120-R. All children who participated in the research were accompanied by parents, who signed informed consent.
Inclusion and Exclusion Criteria
The inclusion criteria were clinical diagnosis of conductive hearing loss [pure tone measurement of bone conduction <30 dB and with an air-bone gap (ABG)] with or without external ear malformation. An intraoperative diagnosis of ossicular chain malformation was made based on abnormal morphology and structure of the auditory ossicles, absence of auditory ossicles, soft connection between joints, and poor movement of the stapes footplate. The exclusion criteria were a history of trauma, sensorineural hearing loss, mixed hearing loss, inner ear deformities, and other systemic diseases.
Grouping Scheme
Based on the results of the intraoperative exploration, auditory malformations were divided into 3 groups: Group 1, incudostapedial joint deformity (with or without stapes footplate fixation); Group 2, simple incus deformity; and Group 3, simple malleus deformity. Moreover, Group A had external ear malformations whereas Group B did not.
Evaluation Method
Imaging examination
All children underwent high-resolution computed tomography (HRCT) of the temporal bone, evaluation of the auditory ossicular chain and the middle ear in bone window, magnetic resonance imaging examinations, evaluation of the inner ear in weighted T2 imaging in oblique sagittal position. The judgment criteria were as follows: Abnormal auditory ossicular morphology, or connection anomaly seen on HRCT, was defined as positive (Figure 1), and no obvious morphological abnormality was defined as negative (Figure 2a and b).
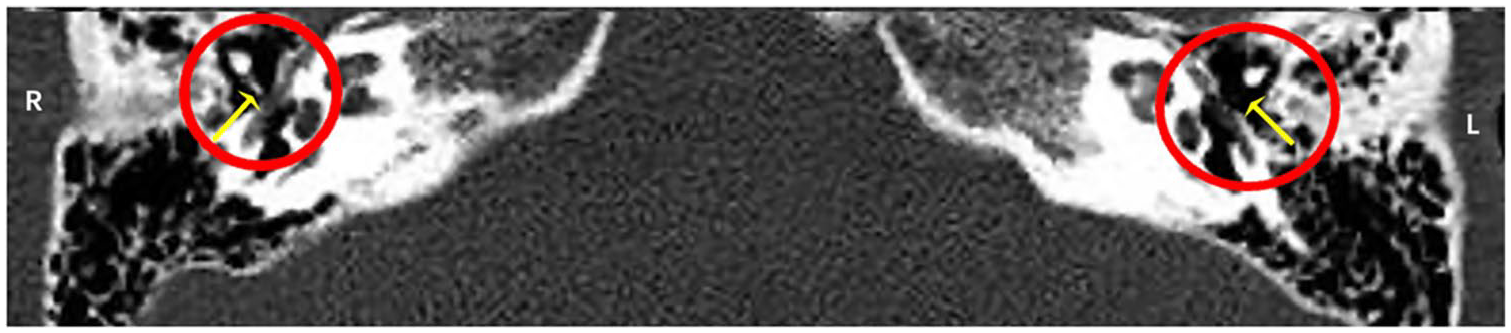
High-resolution computed tomography of the temporal bone indicated that the bilateral incudostapedial joint (yellow arrows in the picture) was abnormal and could not be clearly shown (red circle in the picture).
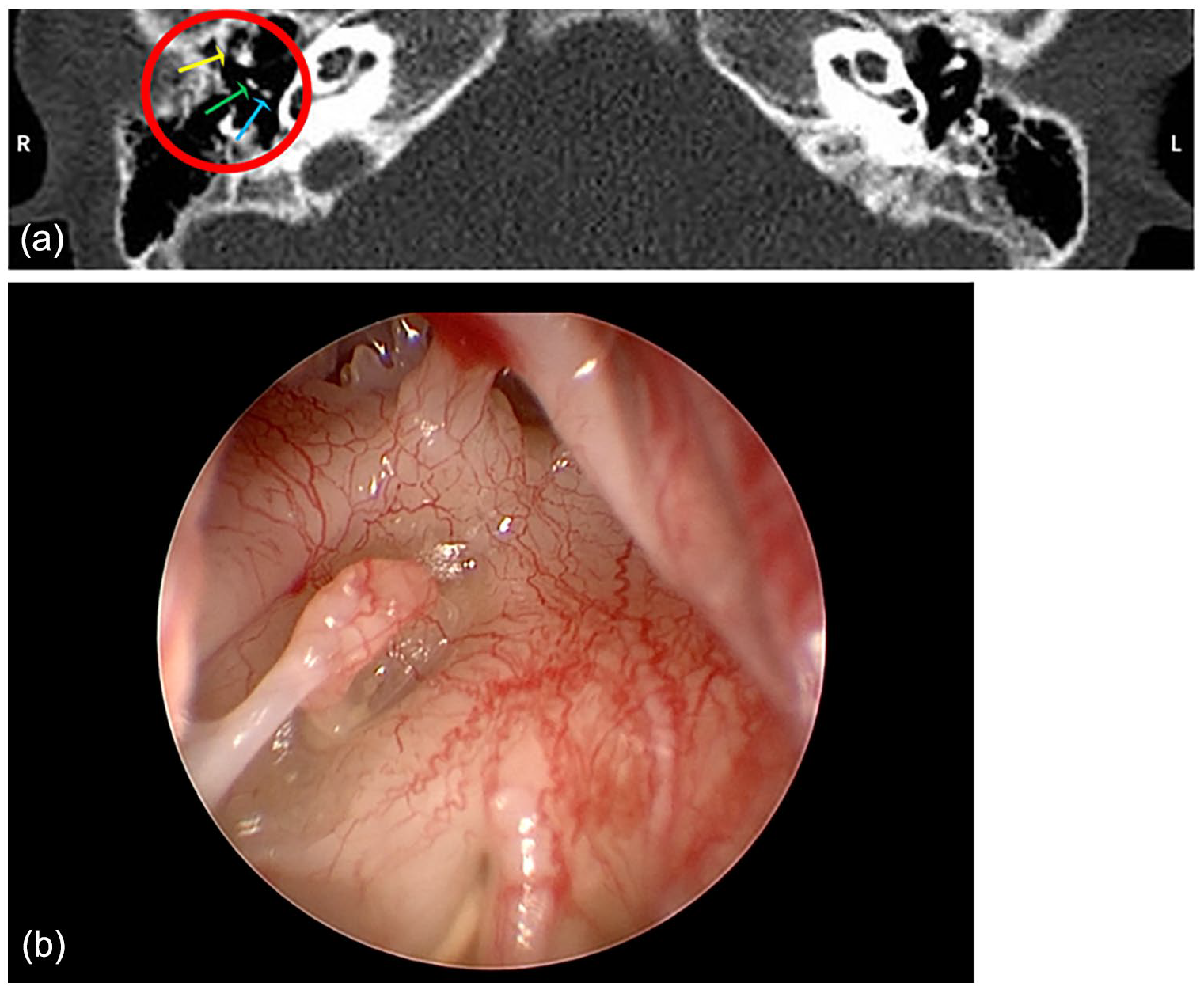
(a) Three ossicles (yellow arrow pointing to malleus, green arrow pointing to incus, blue arrow pointing to stapes) were shown on the horizontal position of the high-resolution computed tomography image before the operation; it was confirmed during the operation that the shape of the long process of the incus was poor. (b) Intraoperative exploration of the incus of the right ear.
Audiological examination
All children were tested for pure tone audiometry (PTA) and acoustic immittance audiometry. PTA was conducted using an Interacoustics®AD229b instrument. We measured air and bone conduction thresholds at 0.5, 1, 2, and 4 kHz. The ABG was recorded. Hearing loss was defined as follows: 26 to 40 dB, mild hearing loss; 41 to 55 dB, moderate hearing loss; 56 to 70 dB, moderate to severe hearing loss. 2 Acoustic immittance audiometry was evaluated using the MAICO®MI44 instrument. Curves A, As, C, and B were divided according to the tympanogram curve and recorded.
Treatment Methods
Middle ear exploration was conducted under microscope or endoscope. We explored the middle ear and performed type II or type III tympanoplasty according to the intraoperative condition. Deformities and implants in the auditory ossicles were recorded during surgery. Partial ossicular prosthesis (PORP) (Figure 3a), total ossicular prosthesis (TORP) (Figure 3b), PISTON stapes prosthesis (Figure 3c), bone bridge implantation (Figure 3d), and autologous ossicular repair (ossicular release) were selected as surgical intervention schemes. Ossicular prosthesis (PORP, TORP, PISTON) are selected from KURZ (Germany). Bone bridge implantations are selected from Med-EI (Austria).
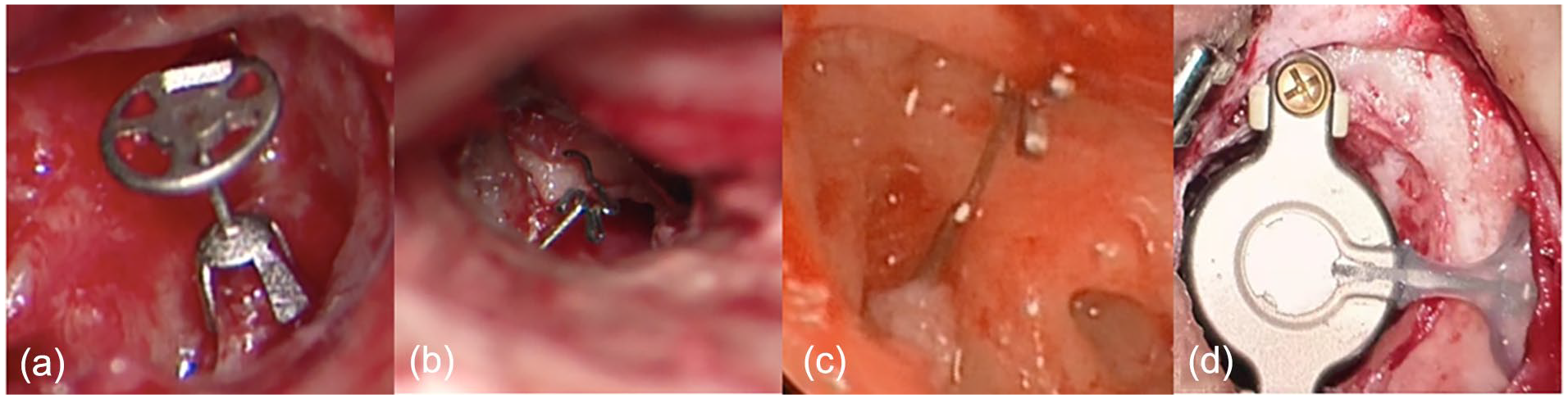
(a) Intraoperative implantation of a partial ossicular prosthesis. (b) Intraoperative implantation of a total ossicular prosthesis. (c) Intraoperative implantation of a PISTON. (d) Bone bridge implantation.
Postoperative Follow-Up Observation Index
Patients were followed up at 3, 6, 12, 18, and 24 months after surgery. Follow-ups included audiological examinations, otoscopy, and tympanometry. Postoperative bone conduction, air conduction, PTA, ABG, and binaural acoustic immittance curves were recorded.
Statistical Processing
SPSS 26.0 software was used for statistical analysis, and all data were tested for normality and homogeneity of variance. Descriptive data are expressed as mean or mean ± standard deviation, and a paired t-test was used to compare the hearing effect before and after the operation. One-way analysis of variance was used for patients with uniform effective rate variance, and the rank-sum test was used for those with uneven variance. Statistical significance was defined at P < .05.
Results
Age of Surgical Intervention
Surgical intervention was performed in 8 children ranging from 5 years 9 months to 12 years 8 months, with a median age of 8.5 years. Postoperative follow-up was conducted for 6 months to 2 years.
Malformation of the Auditory Ossicular Chain
Auditory bone deformities during surgery were as follows: Group 1 (incudostapedial joint deformity group), 6 ears (60%); Group 2 (simple incus deformity group), 2 ears (20%); and Group 3 (simple malleus deformity group), 2 ears (20%). Group A included 4 ears (40%), including 2 ears involving more than 2 auditory ossicles, accounting for 50% of the group; Group B included 6 ears (60%).
During preoperative imaging examination of the temporal bone, HRCT revealed abnormal morphology and connection of the auditory bone (positive) in 7 ears (70%) and no obvious morphological abnormality (negative) in 3 ears (30%). The coincidence rate between the HRCT and intraoperative exploration was 70%. Among the negative ears, 1 ear showed partial loss of the incus long process with stapedial floor fixation, and 2 ears showed partial loss of the incus long process.
The imaging findings, middle ear exploration findings, PTA and ABG preop, PTA and ABG postop, and reconstruction method (Table 1).
Basic Patient Information.
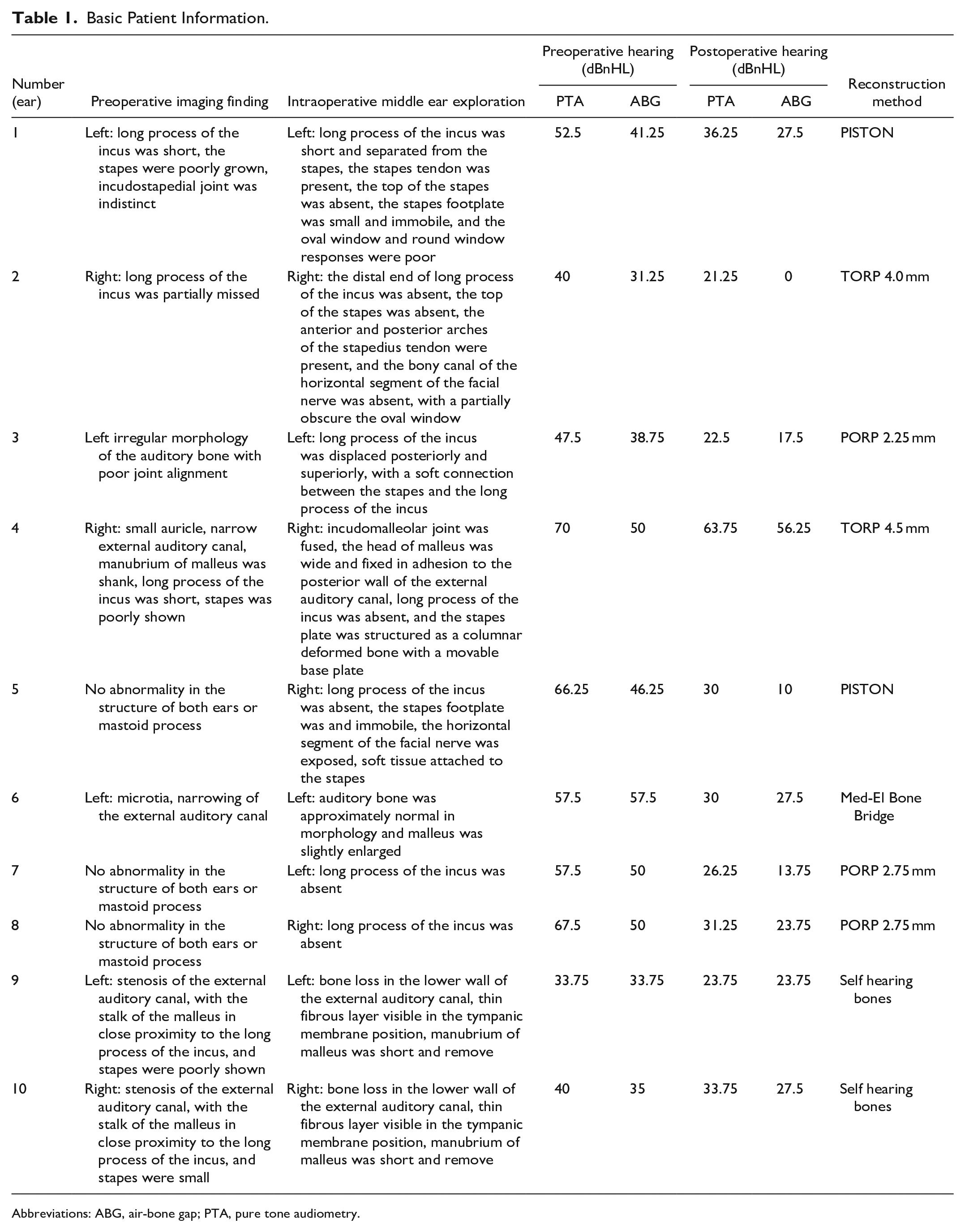
Abbreviations: ABG, air-bone gap; PTA, pure tone audiometry.
Hearing Before and After the Operation
Of the 10 ears, 3 had mild hearing loss, 2 had moderate hearing loss, and 5 had moderate to severe hearing loss. All ears improved after surgical intervention (Table 2). All patients showed statistically significant differences in PTA and ABG improvement after surgical intervention.
Comparison of the Pure Tone Hearing Threshold and ABG Before and After the Operation (n = 10).

Abbreviations: ABG, air-bone gap; PTA, pure tone audiometry; SD, standard deviation.
P < .05 indicated a statistical difference.
Hearing before and after the operation in different auditory malformation groups
In the groups with different deformity sites: there was a statistically significant difference in the improvement of both postoperative PTA and ABG in Group 1, PTA in Group 2, and ABG in Group 3 (Table 3).
Comparison of the Pure Tone Hearing Threshold and ABG Difference Before and After the Operation in Different Auditory Malformation Groups.
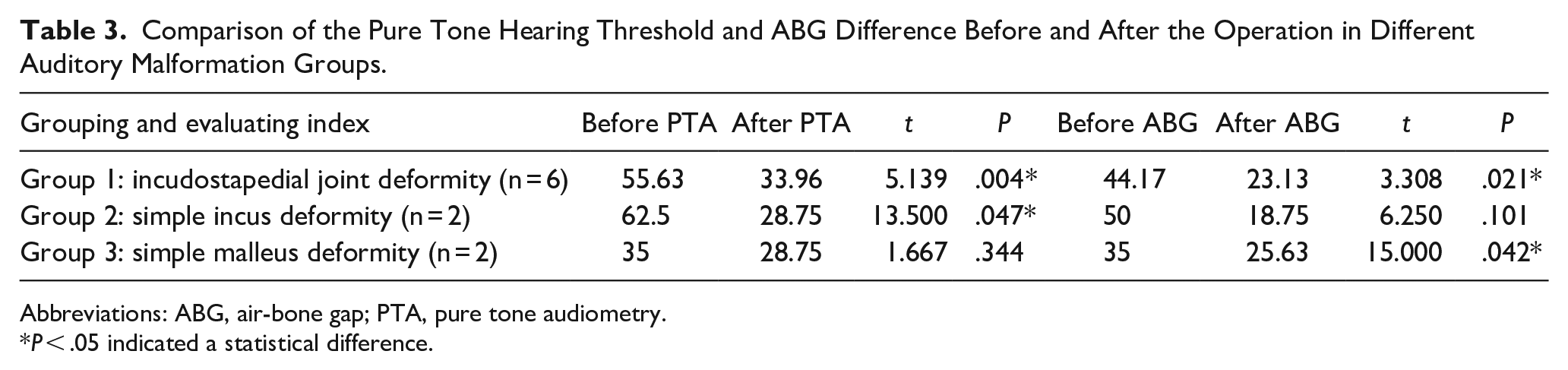
Abbreviations: ABG, air-bone gap; PTA, pure tone audiometry.
P < .05 indicated a statistical difference.
Hearing before and after the operation in Group 1
In the incudostapedial joint deformity, there was a statistically significant difference in the improvement of postoperative PTA in the group without stapes footplate fixation (Table 4).
Comparison of the Pure Tone Hearing Threshold and ABG Between Those With Incudostapedial Joint Deformity With or Without Stapes Plate Fixation Before and After the Operation.
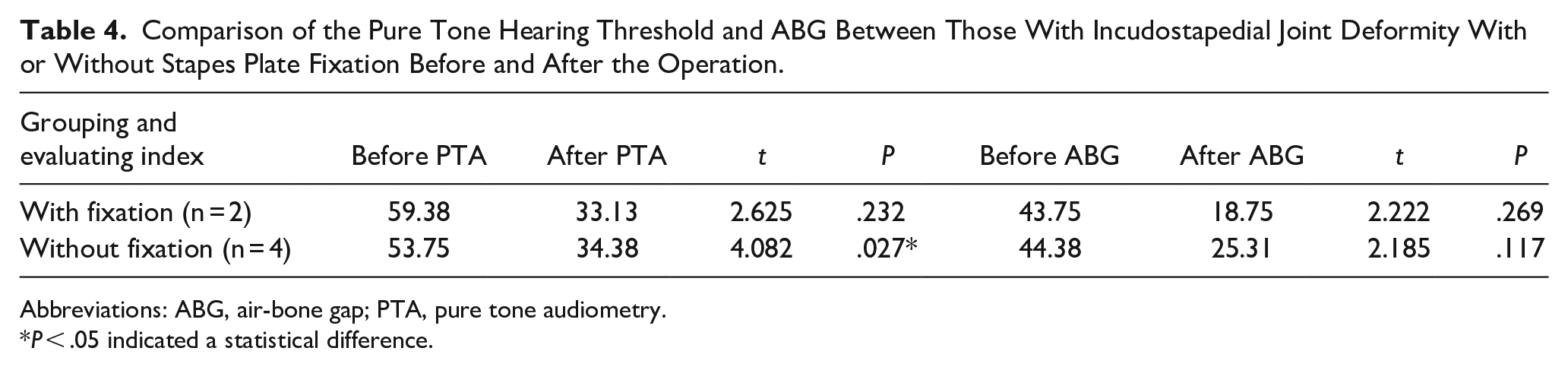
Abbreviations: ABG, air-bone gap; PTA, pure tone audiometry.
P < .05 indicated a statistical difference.
Preoperative and postoperative hearing with or without external ear deformities
There was a statistically significant difference in the improvement of postoperative ABG in the group without external ear malformation (Table 5).
Comparison of Pure Tone Hearing Threshold and ABG Before and After Operation With or Without External Ear Malformation.
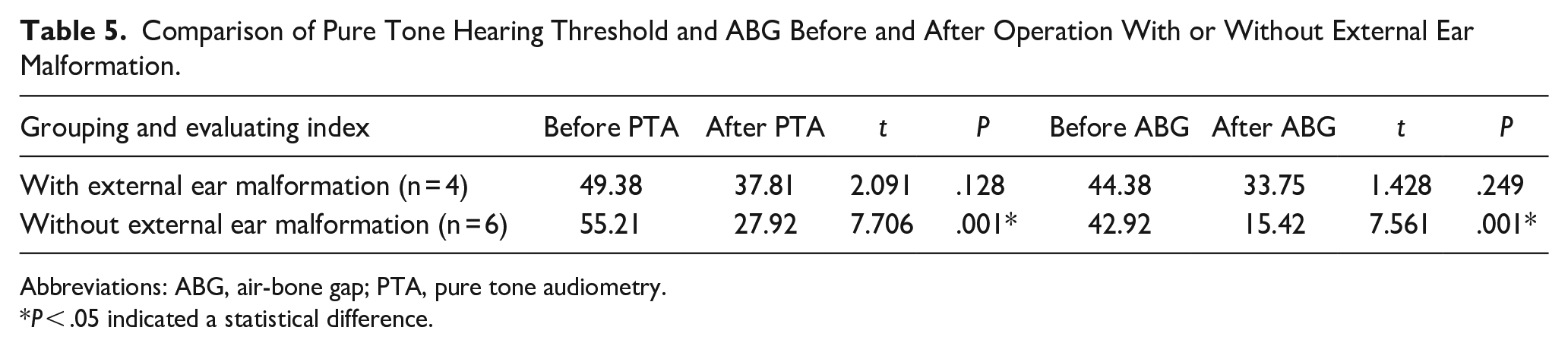
Abbreviations: ABG, air-bone gap; PTA, pure tone audiometry.
P < .05 indicated a statistical difference.
Comparison of postoperative effects of different implantation schemes
Comparing the different implantation protocols, there was a statistically significant difference in the improvement of postoperative PTA and ABG in the PORP group and ABG in the autologous auditory bone group, and no difference was found in the remaining groups (Table 6).
Comparison of Hearing Between Different Implant Groups Before and After the Operation.
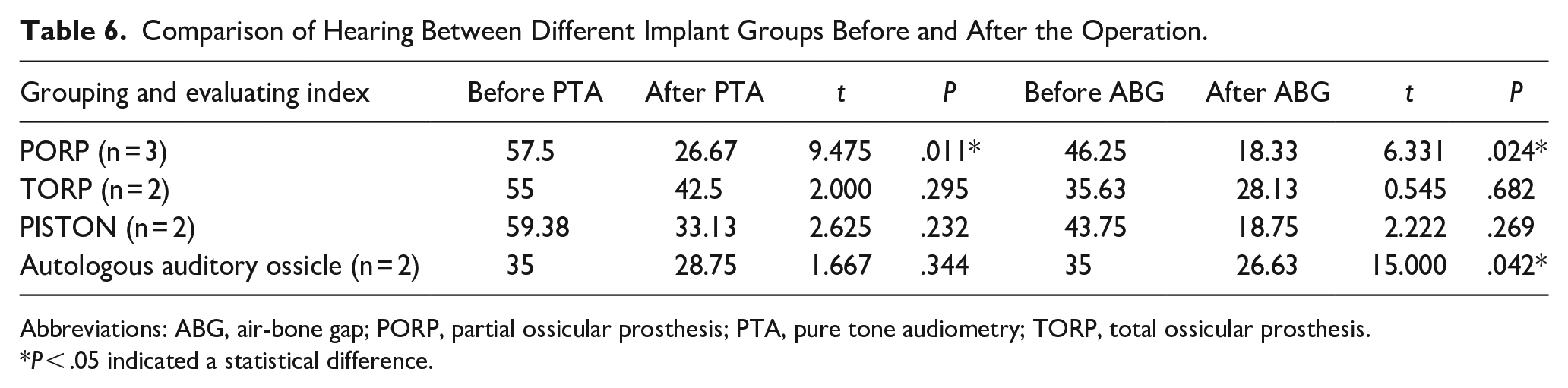
Abbreviations: ABG, air-bone gap; PORP, partial ossicular prosthesis; PTA, pure tone audiometry; TORP, total ossicular prosthesis.
P < .05 indicated a statistical difference.
Artificial Ossicular Implantation in the Same Auditory Malformation Group
Group 1: Incudostapedial joint deformity
In Group 1 (the anvil joint deformity group), due to the abnormal joint, the auditory threshold after implanted PORP decreased by 25 dB and the ABG decreased by 21.25 dB. The average hearing improvement was 12.5 dB and the ABG decreased by a mean of 12.5 dB after implantation of TORP. In the PISTON implanted group, the average hearing improvement was 26.25 dB and the ABG decreased by 25 dB. Moreover, the hearing threshold of the implanted bone bridge decreased by 27.5 dB and the ABG reduced by 30 dB.
Group 2: Simple Incus deformity
Two ears in Group 2 (the simple incus deformity group) were treated with PORP; the postoperative hearing improvement was more than 30 dB and the ABG decreased by approximately 30 dB.
Group 3: Simple Malleus deformity
In Group 3 (the simple malleus deformity group), 2 ears were treated with autologous auditory bone transplantation, and the decrease in the hearing threshold and ABG were both 10 dB.
Group with external ear malformations
Due to external ear malformations, middle ear lesions are often more severe in patients with external ear deformities, making them more likely to involve multiple auditory bones. After TORP implantation, the hearing threshold decreased by 6.25 dB and the ABG increased by 6.25 dB. Moreover, in patients with a bone bridge, the hearing threshold decreased by 27.5 dB and the ABG decreased by 30 dB. Lastly, in patients with autologous auditory ossicle implantation, the average hearing improvement was 10 dB and the ABG reduced by 10 dB.
Group without external ear malformations
In our clinic, hearing loss in those without external ear malformations is usually not as severe compared to those with external ear malformations; however, there can be deformities in any part, and there are different options for auditory bone implantation. The average hearing improvement after PORP implantation was 30.83 dB and the ABG decreased by a mean of 27.92 dB. After TORP implantation, the hearing improvement was 18.5 dB and the ABG decreased by 31.25 dB. After PISTON implantation the hearing improvement was 26.25 dB and the ABG decreased by 25 dB.
Discussion
Common Sites of Ossicular Chain Malformations in Children
The morphology of the auditory ossicles is related to embryonic development. After the fifth week of embryonic development, the first and second pharyngeal arches form the parenchyma around the tympanic primordium. The main cellular components are cranial neural crest cells, which contain Meckel’s and Reichert’s cartilage. The malleus and incus mainly develop from the Meckel’s cartilage, 3 and the stapes mainly develop from the Reichert cartilage. Due to different sources, any risk factors affecting the development of the pharyngeal arch can lead to malformation of the incus and stapes and an abnormal soft incudostapedial joint. This study suggests that malformations of the incudostapedial joints are the most common, and the localization of malformed ossicles should be combined with audiology and imaging examination. 4 Auditory bone deformities with external ear deformities are usually complex, and multiple auditory bones can be involved, even if they are not associated with external ear malformations. Multiple auditory ossicular deformities accounted for 60% of the cases in this study while multiple auditory malformations accounted for 50% of external ear malformations.
Relationship Between Preoperative Imaging Examination and Intraoperative Exploration Results of Ossicular Chain Malformation
In the past, before the development of advanced imaging examinations, malformations of the ossicular chain were primarily diagnosed based on audiologic assessments, 2 followed by confirmation through middle ear exploration.2,5,6 At present, HRCT of the temporal bone is the first choice of imaging examination for middle ear malformations. The minimum age for temporal bone CT examination is 2 years, which is advantageous for younger patients. 5
In this study, The coincidence rate between the imaging examination and intraoperative exploration part of the incus was missing and the stapes footplate was fixed; 2 ears in which the long process was 70%. Three negative ears were confirmed by surgical exploration: 1 ear in which the long process of the incus was absent; and none of the 3 ears with external ear deformities. HRCT has some limitations in the diagnosis of stapes footplate fixation without an external ear deformity and in the absence of the long process of the incus.
In the diagnosis of stapes footplate fixation without external ear deformity and loss of the long process of the incus, in addition to audiological examination, it is necessary to improve the accuracy of imaging examinations, such as 3-dimensional reconstruction. Surgical exploration is the gold standard for diagnosis. When clinicians encounter children with speech delay and conductive hearing loss, even if the imaging findings are not abnormal, surgical exploration should be considered to confirm the diagnosis.
Selection of Surgical Intervention for Ossicular Chain Malformation
The ossicular chain consists of 3 auditory ossicles: malleus, incus, and stapes. Unlike other bones, the auditory bone has no ability to regenerate; thus, any discontinuity of the ossicular chain can only be repaired by reconstructive surgery or ossiculoplasty.7,8 This study found that both PORP and PISTON can effectively improve postoperative hearing in children with incudostapedial joint deformity, but the effect of PISTON in decreasing the ABG is slightly worse. If there is stapes footplate fixation, the PISTON needs to be implanted after opening the oval window on the stapes footplate. It’s worth noting that in this case of bone bridge implantation, this intervention approach was chosen because the patient also had severe narrowing of the external auditory canal. The implantation had an ideal outcome; however, it incurred high costs and posed some postoperative aesthetic concerns. As a result, when a child is diagnosed with incudostapedial joint deformity, the condition of the external ear should also be considered in the selection of implantation options. If a patient has severe external ear malformation, then a bone bridge implantation or other bone conduction hearing aids [eg, Bone-anchored hearing aid, Sophono and bone-anchored hearing aids (BAHAs) attract] should be considered. Long-term BAHA wearing intervention is better than external otoplasty for long-term hearing improvement. 9 But traditional BAHAs are susceptible to complications, including skin infections. Conversely, Sophono and BAHA Attract devices do not present this issue. While the auditory efficacy of Sophono and BAHA Attract is comparable to that of conventional BAHAs, the skin’s dampening of high-frequency vibrations results in slightly reduced effectiveness of percutaneous bone conduction hearing aids in addressing high-frequency hearing loss, nonetheless, it continues to exhibit a consistent therapeutic efficacy. 10 If the parents do not want the child to have postoperative scars, the selection of artificial auditory ossicles is the best choice to improve hearing effectively, while PISTON implantation is the first choice for definite stapes footplate fixation. A new research suggests that Tympanosclerosis children may be better treated with alternative procedures such as malleovestibulopexy, TORP, or amplification instead of traditional stapes surgery. 11 For children with simple malleus deformities, the effect of the autologous auditory bone is limited; therefore, new implantation schemes must be considered. Bone bridge implantation can be considered if children with simple malleus deformities have external ear deformities. In children with simple incus malformations, the effect of PORP implantation is better and postoperative hearing is greatly improved. For ossicular chain malformations without external ear deformities, the effect of PORP and PISTON implantation is better; however, if children have a larger air-bone gap due to the absence of a stapes suprastructure or an immobile stapes footplate, TORP implantation can decrease the ABG to a great extent.
Effect of Surgical Intervention on Malformation of the Ossicular Chain
If we strongly suspect children to have ossicular chain malformations, whether they are accompanied by stenosis of the external ear or not, otologists should consider surgical treatment. The implantation of PORP and PISTON in children with ossicular chain malformations had a positive effect on reducing the postoperative hearing threshold and reducing the ABG. The preoperative hearing loss in patients with stapedial footplate fixation was slightly higher than that in patients without stapedial footplate fixation, and PISTON implantation achieved better results. The overall change in the hearing threshold in children with mobile stapes footplates was better than that in children with immobile stapes footplates. If, it is accompanied by a severe external ear malformation, bone bridge implantation is an ideal treatment option for improving postoperative hearing; however, many factors need to be considered. Bone bridges have been found to be more effective than BAHA in enhancing speech recognition; however, their implantation in the mastoid region of the middle ear poses potential risks, including implantation failure and challenges in patients with significant middle ear deformities. 12 The postoperative ABG in children with TORP implantation in the second ear in this study was larger than the preoperative ABG. This increase can be attributed to restenosis of the external auditory canal after hearing reconstruction. When assessing the prognosis of the intervention, it is important to consider that children with external ear malformations may require additional evaluation assessing sustained effects after external auditory canaloplasty to objectively assess the postoperative outcome. The intervention effect of autologous auditory ossicular repair or release in children with simple malleus deformity is limited. Accordingly, it is necessary to choose a better treatment protocol to improve postoperative hearing. The surgical effect in children with external ear malformations is generally worse than that in children without external ear malformations.
It’s important to acknowledge the limitations that exist in this study. Firstly, the sample size of the enrollment was small and the data analysis may be biased. Secondly, there was a single case of the intervention program that could not be analyzed. Lastly, for the type of deformity with low intervention effect, we didn’t provide a better intervention plan.
Conclusions
The most common malformation of the ossicular chain in children is the incudostapedial joint malformation. A certain rate of preoperative imaging examinations may yield negative results, necessitating the integration of auditory information to establish a definitive diagnosis. This is particularly critical in cases lacking the long foot of the incus or exhibiting stapes footplate fixation. Additional precise and comprehensive evaluation methods should be employed to ascertain the nature of the deformity. The effects of PISTON and PORP implantation in incudostapedial joint malformation are high, while bone bridge implantation can be considered in patients with severe external ear malformation. Autologous auditory bone repair can enhance hearing and reduce ABG, but its benefits are limited. Patients with simple incus malformations had better outcomes. There may be different intervention schemes for the same site of auditory ossicular malformation, and different intervention schemes should be based on an accurate assessment of the deformity. The effective range of stapes footplate activity can improve the prognosis. Future research could be directed toward more efficient surgical protocols and interventions for malformation of the ossicular chain in order to improve hearing as much as possible.
Footnotes
Acknowledgements
The authors gratefully acknowledge Prof. Jie Zhang for his guidance and quality control of this study, as well as the authors for their dedication to this study.
Author Contributions
All authors were involved in the conception. J.S.Z. wrote the first draft, which was reviewed and revised by J.Z. Conceptualization and method, J.Z.; formal analysis, W.L. and N.M.; clinical investigation, J.Z., W.L., N.M., and J.B.S.; resources, X.X.W. and S.L.L.; data curation, Y.X.L. and L.N.G. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Project of Education and Teaching Reform of Capital Medical University, No. 2022JYY268, Research Project of Education and Teaching Reform of Capital Medical University, No. 2022JYZ026 and Capital medical university research and cultivation fund grant number PYZ21141.
Ethical Approval
This study was approved by the Ethics Committee of Beijing Children’s Hospital. Ethics (Clinical Research) Review Number: [2023]-E-120-R.