
Abstract
Objective:
The aim of this study is to describe the clinical characteristics and intraoperative findings and further evaluate the efficacy of endoscopic ossiculoplasty for the management of isolated congenital ossicular chain malformation.
Methods:
A retrospective study was performed on 16 ears (15 patients) with the isolated congenital ossicular chain malformation who underwent endoscopic ossiculoplasty in our department from May 2017 to January 2019. Endoscopic exploratory tympanotomy was conducted to check the ossicular chain; at the same time, endoscopic ossiculoplasty was performed depending on intraoperative findings. Air-conduction thresholds, bone-conduction thresholds, and air-bone gaps (ABGs) were measured before and after surgery, and the hearing outcome was assessed at 6 months postoperatively.
Results:
The most common malformations of ossicular chain were the missing of the incus long process and stapes suprastructure. A serial assessment of the hearing status was conducted before and 6 months after surgery. It showed the mean postoperative pure-tone average (PTA) was significantly reduced, and the mean postoperative ABG was obviously closed, respectively (P < .001). The mean PTA gain was 36.3 ± 8.6 dB, and the ABG closure was 35.1 ± 8.3 dB; ABG closure to 20 dB or less and ABG closure to 10 dB or less were achieved in 14 cases (87.5%) and 5 cases (31.3%), respectively. No differences were observed in postoperative hearing outcome between type Ⅲ cases and type Ⅳ cases; however, cases with partial ossicular replacement prosthesis implantation showed a larger hearing gain (P = .049) and a higher proportion of postoperative ABG less than 10 dB (P = .021). No facial palsy and significant sensorineural hearing loss occurred; all patients completed the surgery without the need of canalplasty, and the chorda tympani nerve was preserved in all patients.
Conclusions:
This research showed endoscopic surgery was effective in the diagnosis and management of isolated congenital ossicular chain malformation; the endoscopic ossiculoplasty provides an alternative method to manage congenital ossicular chain malformation, with comfortable hearing outcome and the advantage of excellent vision and less invasion.
Introduction
The isolated congenital ossicular chain malformation (ICOCM) accounts for a small part of middle ear malformation cases and is usually characterized by deformities of ossicular chain without malformation of the external ear or other organs. 1 -3 However, as the tympanic membrane and external canal often appears normal, the ICOCM is prone to be misdiagnosed in clinical practice. 4 The ICOCM often shows severe conductive hearing loss since childhood; with the development of modern imaging technology, more and more ICOCM cases were diagnosed before surgery. However, many minor malformation cases were still missed before surgery. 5 Therefore, exploratory tympanotomy was the main approach for the diagnosis of ICOCM, and ossiculoplasty could be performed at the same time according to the intraoperative findings.
In order to facilitate surgical approach selection to reconstruct the ossicular chain, some researchers proposed some classification systems for congenital ossicular chain malformation. 1,2,4,6 The widely accepted classification system was proposed by Teusnissen and Cremers in 1993, which classified ossicular chain malformation into 4 types. 1 In the past decades, microscopic ossiculoplasty had achieved satisfactory hearing improvement; however, endoscopic tympanoplasty has increased annually in recent years, showing some obvious advantages compared with microscopic tympanoplasty. 7,8 In our own experiences of endoscopic tympanoplasty, these advantages seem to be especially obvious in minimal invasive middle ear surgery. However, up to date, only few studies with very limited cases reported endoscopic ossiculoplasty in ICOCM. 9,10 Herein, we report a series cases of ICOCM from China, to evaluate the surgical results of endoscopic ossiculoplasty.
Materials and Methods
Clinical Data
A retrospective analysis was performed on patients who visited our hospital and underwent ear surgeries due to hearing loss between May 2017 and January 2019. A total of 632 patients were performed tympanomastoid surgeries, and the cases met the following criteria were included in this study. Inclusion criteria were as follows: (1) a typical history of conductive hearing loss since early childhood and no history of hearing loss caused by otitis media or trauma, (2) a normal external acoustic meatus and an intact tympanic membrane and no other congenital diseases or abnormal tissue structure, and (3) the case was confirmed as ICOSM and excluded other diseases that induced congenital hearing loss, such as otosclerosis, congenital cholesteatoma, and so on. Exclusion criteria were as follows: (1) ICOSM combined with otitis media, (2) severe malformation of ossicular or facial never, a postauricular incision was adopted, or the ossiculoplasty was aborted, and (3) the case lost to follow-up and postoperative hearing outcome was not obtained. This study was approved by the institutional ethics review board of our institution, and informed consent was obtained for our study from all participating patients.
A total of 17 ears (16 patients) were included; however, 1 case was aborted for ossiculoplasty as the oval window was covered by a malformed facial nerve (Supplemental Figure). Therefore, this research analyzed the 16 ears (15 patients) which had undergone endoscopic ossiculoplasty. According to the Teunissen and Cremers classification system, 13 ears were type Ⅲ and 3 ears were type Ⅳ. 1 Fifteen patients showed unilateral ear anomalies, and 1 patient showed bilateral ear anomalies. The patients included 10 males (11 ears) and 5 females (5 ears), with an age range of 9 to 48 years and an average age of 26.2 ± 13.3 years. All patients had hearing loss since childhood without progressive aggravation.
High-resolution computed tomography (CT) scans and 3-D reconstruction of ossicular chain were performed before surgery. Preoperative CT scans confirmed ossicular chain malformation in 13 ears and misdiagnosed for the other 3 ears, whose intraoperative findings showed tissue connection between the stapes head and the terminal of the partial missing incus long process (P1, P4, P11). The pure-tone threshold audiometry was routinely conducted, the pure-tone average (PTA) of 4-frequency (0.5, 1.0, 2.0, and 4.0 kHz) ranged from 46 to 73 dB, the bone conduction (BC) threshold of all affected ears range from 5 to 35 dB, and the air-bone gap (ABG) was obtained from AC-PTA and BC-PTA. Tympanogram has already been classified as type A in 11 ears, type Ad in 3 ears, and type As in 2 ears. The Gelle’s test was negative in 14 ears and suspected positive in 2 ears.
Surgical Methods
Endoscopic exploratory tympanotomy was performed under general anesthesia by the same senior surgeon (C.Z.). A tympanomeatal flap incision was made with a transcanal approach to expose the tympanic cavity. The smaller amount scutum was removed using a curette in 6 ears (37.5%) for exposing the ossicular chain and oval and round window. The ossicular morphology, connection, and mobility were explored using 0° and 30° endoscopes (Karl Storz). Various ossicular reconstruction strategies were applied depending on the type of malformation as follows: (1) a piston prosthesis (Spiggle-Theis) was used in the case of stapes ankylosis or aplasia of oval window, (2) a partial ossicular replacement prosthesis (PORP; Spiggle-Theis) was used in the case of normal stapes suprastructure with mobile footplate, and (3) a total ossicular replacement prosthesis (TORP; Spiggle-Theis) was used in the case of abnormal stapes suprastructure with mobile footplates or oval window dysplasia. A small piece of tragal cartilage was harvested and placed between the PORP/TORP prosthesis and the tympanic membrane. Finally, the external auditory canal was packed with gelatin sponge particles. At the end of the operation, the amount of bleeding was recorded. Two weeks later, the packing materials were cleaned and the tympanic membrane was examined with ear endoscopy in the outpatient department. Six months after the surgery, hearing status was assessed by pure-tone audiometry. All patients were followed up at least 1 year.
Statistical Methods
A SPSS 17.0 statistical software (SPSS, Inc) was used for data analyses. A 1-sample Kolmogorov-Smirnov test was used to analyze the normality of the data distribution. A paired-samples t test or Wilcoxon signed rank test were used for comparisons before and after surgery. A P value <.05 was considered statistically significant.
Results
Intraoperative Findings
Endoscopic exploratory tympanotomy revealed that ossicular chain malformation usually involved the incus and stapes suprastructure. Most cases showed a normal malleus, except for 3 ears (18.8%) showed the fixation of incudomalleolar joint. The malformation of incus was observed in 14 ears (87.5%), the most common malformation was the various degree missing of the long process. Stapes malformation was observed in 10 ears (62.5%), which often involved the stapes suprastructure with a mobile footplate (7 in 10 ears). Oval window aplasia or dysplasia which was classified as type Ⅳ was observed in 3 ears (P13, P14, P15): 1 ear (P13) showed the dysplasia of oval window and missing of stapes, as well as facial nerve anomaly, and 2 ears (P14, P15) showed aplasia of oval window and stapes malformation (Table 1, Figures 1 and 2).
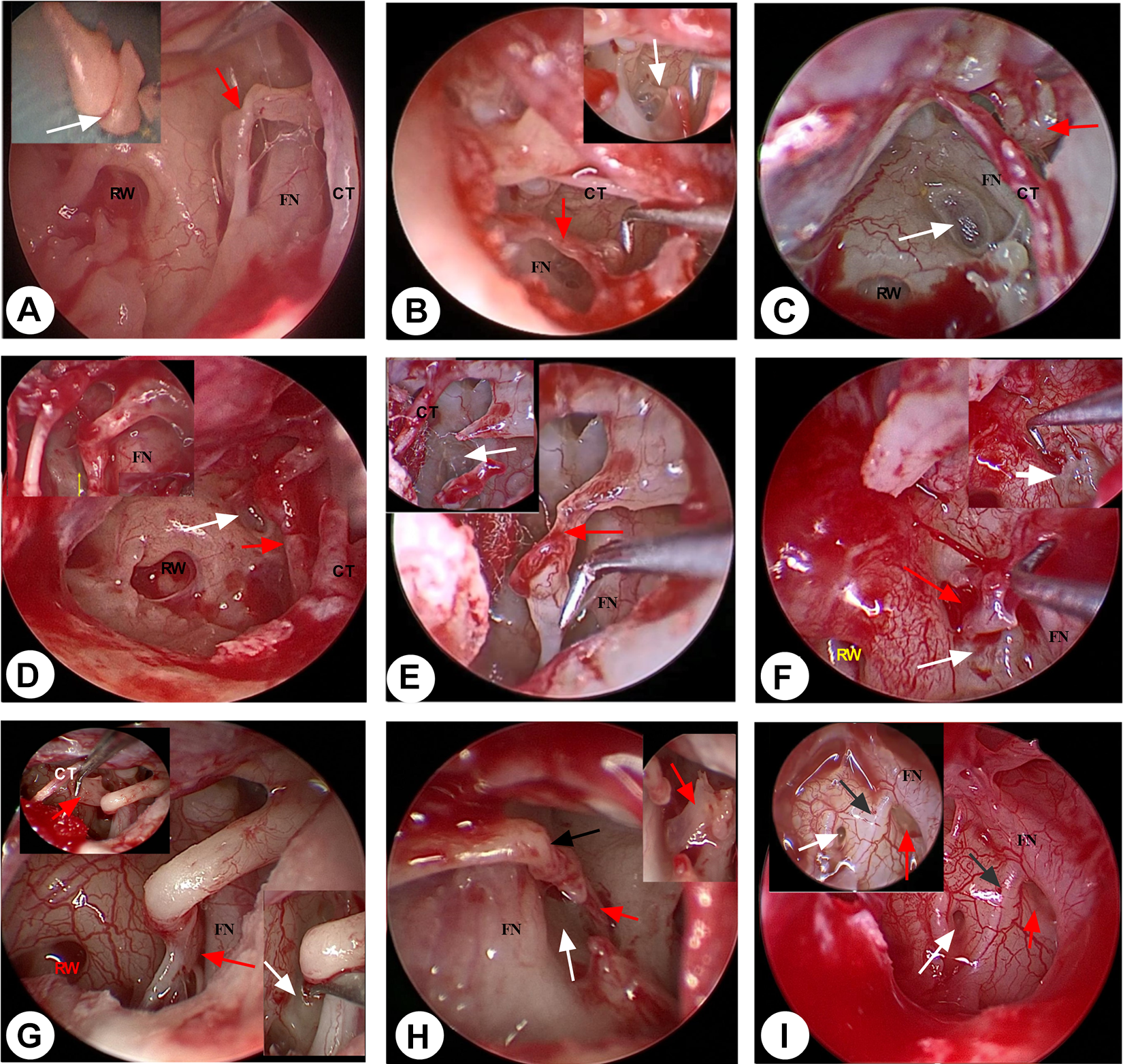
Various ossicular malformation types under endoscopic view. CT indicates chorda tympani never; RW, round window; FN, facial nerve. A, White arrow showed incudomalleolar joint fusion; red arrow showed a mild degree missing of the incus long process, which was instead by a soft tissue connection between the long process residual and the normal stapes. B, Red arrow showed a moderate degree missing of the incus long process, which was instead by a soft tissue connection between the long process residual and the normal stapes; white arrow showed a normal stapes. C, Red arrow showed a severe degree missing of incus long process; white arrow showed absence of stapes suprastructure with a mobile footplate. D, Red arrow showed a tissue connection between the long process and stapes tendon; white arrow showed absence of stapes suprastructure with a mobile footplate. E, Red arrow showed a moderate degree missing of the incus long process, which was instead by a soft tissue connection between the long process residual and the stapes tendon; white arrow showed absence of stapes suprastructure with a mobile footplate. F, Red arrow showed a stapes anomaly with a complete missing of incus; white arrow showed the aplasia of oval window closed by bony plate. G, Red arrow showed a stapes anomaly with a normal incus; white arrow showed the aplasia of oval window closed by bony plate. H, Red arrow showed a stapes anomaly; white arrow showed the aplasia of oval window closed by bony plate; black arrow showed a shorter long process and a longer lenticular process of incus. I, Red arrow showed dysplasia of oval window under 0° and 30° endoscopic view; white arrow showed dysplasia of round window under 0° and 30° endoscopic view; black arrow showed a facial nerve malformation.
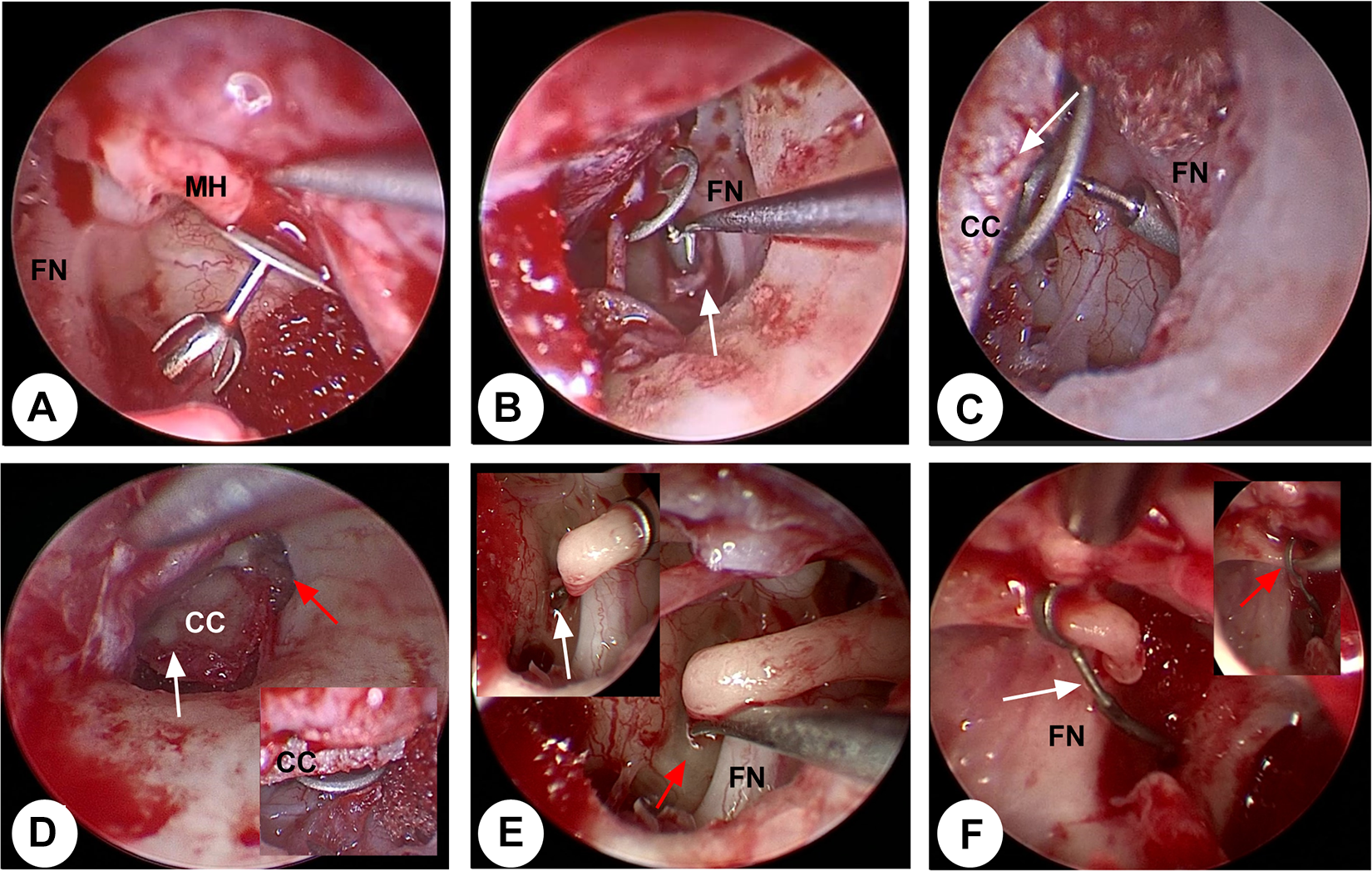
Various endoscopic ossiculoplasty strategies and skills. FN indicates facial never; C, cartilage and perichondrium complex; MH, malleus handle. A, It showed a malleus handle-partial ossicular replacement prosthesis (PORP)-stapes ossiculoplasty. B, It showed a malleus handle-total ossicular replacement prosthesis (TORP)-footplate ossiculoplasty strategy, with a small piece of fascia underlaid TORP for fixation. C, It showed a malleus handle-TORP-footplate ossiculoplasty strategy, with a small piece of cartilage covered upon TORP for fixation. D, White arrow showed a small piece of cartilage and perichondrium complex was placed between the malleus handle and TORP/PORP for more close connection; red arrow showed no scutum bony removal and canaloplasty was necessary. E, Red arrow showed aplasia of oval window closed by bony plate; white arrow showed small fenestra stapedotomy, and piston implantation was performed. F, Red arrow showed a straight piston was failed to clipped to the shorter long process; white arrow showed the piston was slightly curved and then could closely fixed onto the long process.
Patients Characteristics, Intraoperative Findings, and Endoscopic Ossiculoplasty Effects.
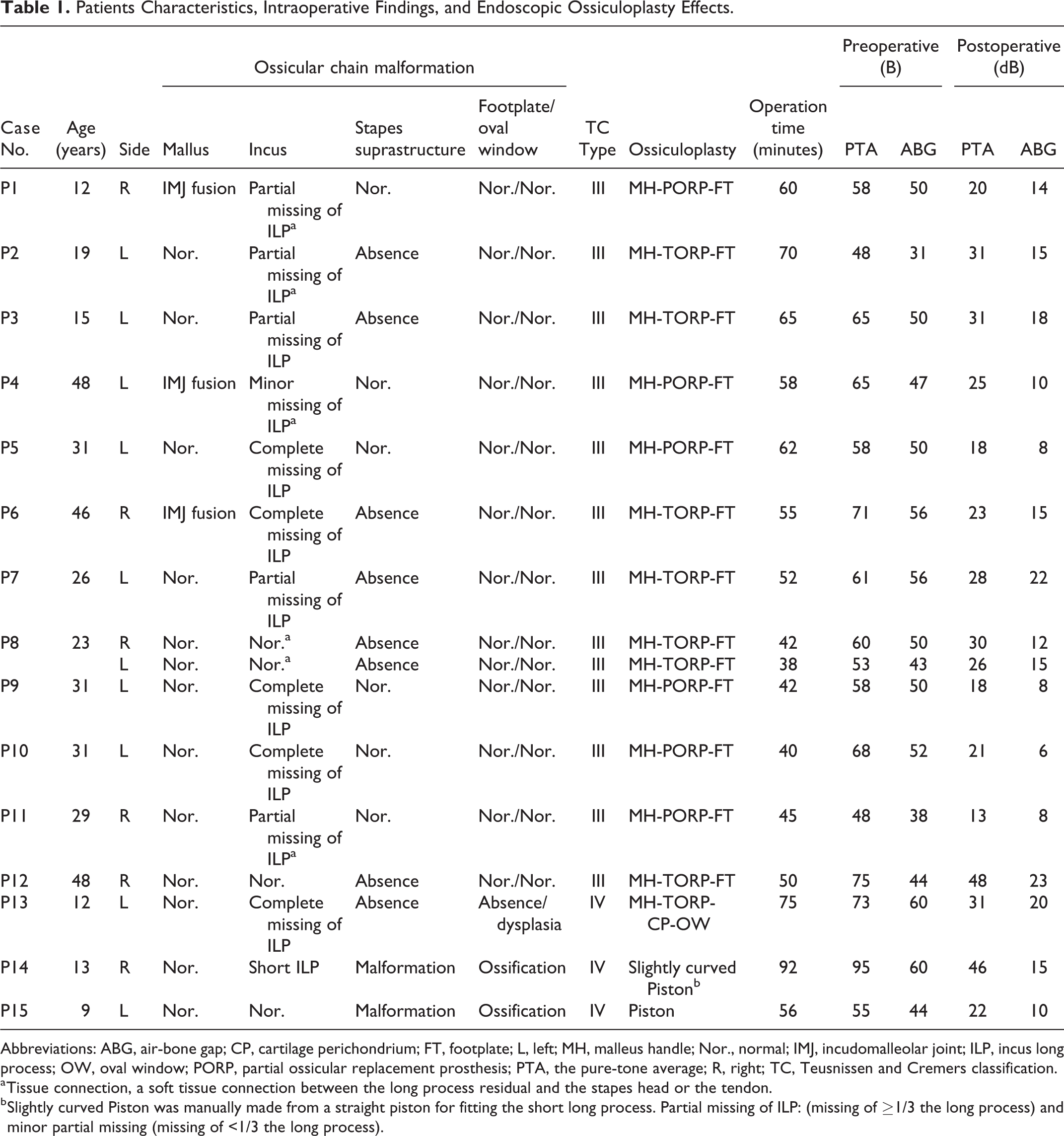
Abbreviations: ABG, air-bone gap; CP, cartilage perichondrium; FT, footplate; L, left; MH, malleus handle; Nor., normal; IMJ, incudomalleolar joint; ILP, incus long process; OW, oval window; PORP, partial ossicular replacement prosthesis; PTA, the pure-tone average; R, right; TC, Teusnissen and Cremers classification.
a Tissue connection, a soft tissue connection between the long process residual and the stapes head or the tendon.
b Slightly curved Piston was manually made from a straight piston for fitting the short long process. Partial missing of ILP: (missing of ≥1/3 the long process) and minor partial missing (missing of <1/3 the long process).
Surgical Results of Endoscopic Ossiculoplasty
The operation time ranged from 38 to 92 minutes, and the average of operation time was 56.4 ± 14.5 minutes. A serial assessment of the hearing status was conducted before and 6 months after surgery. The mean postoperative PTA was significantly reduced, and the mean postoperative ABG was obviously closed than those of the preoperative (P < .001). The mean PTA gain was 36.3 ± 8.6 dB, and the ABG closure was 35.1 ± 8.3 dB. The average BC was not changed significantly (P = .241). The ABG closure to 20 dB or less and ABG closure to 10 dB or less were achieved in 14 cases (87.5%) and 5 cases (31.3%), respectively (Table 2).
Hearing Comparison Between Before and After Surgery.
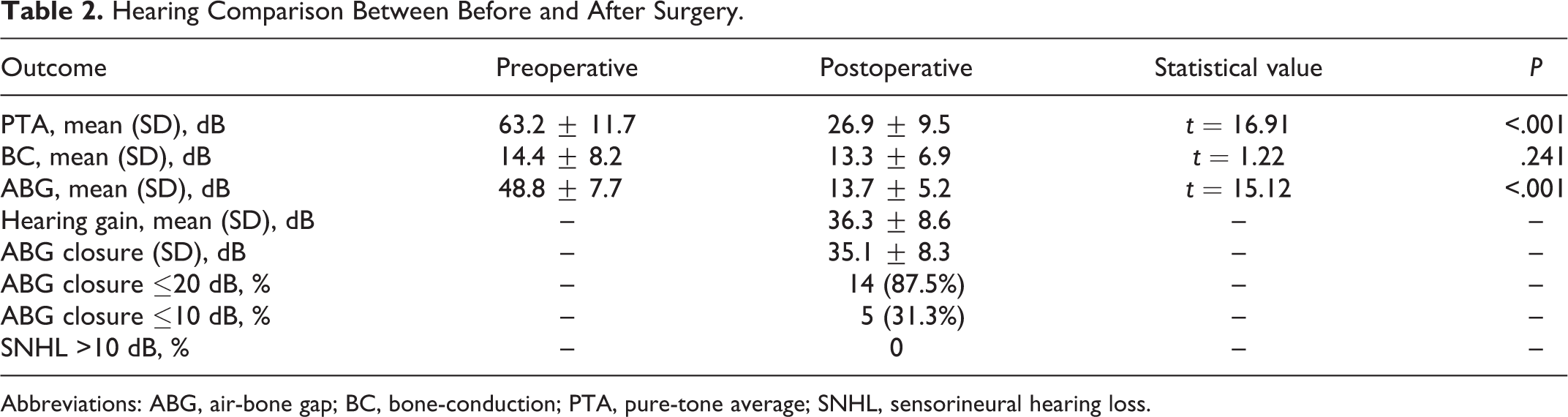
Abbreviations: ABG, air-bone gap; BC, bone-conduction; PTA, pure-tone average; SNHL, sensorineural hearing loss.
We also analyzed the postoperative hearing outcome between type Ⅲ cases and type Ⅳ cases; no statistical differences were found in PTA gain and ABG closure, respectively (P = .269 and .310). Moreover, we compared the hearing status between PORP implantation and TORP implantation; no difference of PTA and ABG were found before surgery. However, cases with PORP implantation showed a significant larger PTA gain (P = .049) and a statistical higher proportion of postoperative ABG less than 10 dB (P = .021; Table 3).
Hearing Comparison Between PORP and TORP Implantation for Type III Cases.
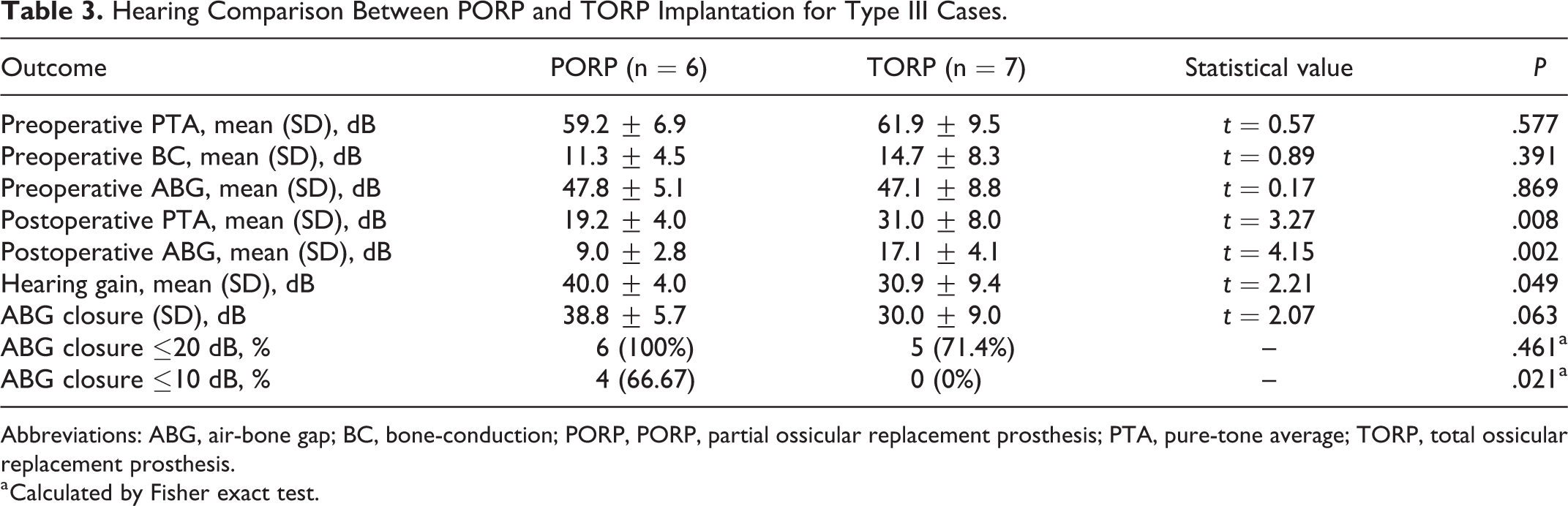
Abbreviations: ABG, air-bone gap; BC, bone-conduction; PORP, PORP, partial ossicular replacement prosthesis; PTA, pure-tone average; TORP, total ossicular replacement prosthesis.
a Calculated by Fisher exact test.
Complications
All patients completed the surgery without the need of canalplasty; the chorda tympani nerve was preserved in all patients. Moreover, the amount of bleeding was less than 5 mL. No major complications, such as facial palsy and significant sensorineural hearing loss, occurred.
Discussion
In this research, a series of ICOCM cases from China were retrospectively analyzed; although a few previous studies had reported surgical management of ICOCM, the number of cases is generally small. 1 -4,6,11 -16 Endoscopic ear surgery has rapidly developed in recent decade 7,8,17 ; however, so far, only few studies reported endoscopic ossiculoplasty for ossicular chain malformation. Wu et al 9 retrospectively analyzed endoscopic surgery for 12 patients with congenital ossicular chain anomalies and showed showed endoscopic surgery is suitable for the management of various types of congenital ossicular chain anomalies. Zhu et al 10 reported 8 pediatric congenital ossicular fixation treated by endoscopic ossiculoplasty and showed endoscopic approach was effective in improving hearing and was an alternative method for the management of congenital ossicular pathology. In this research, our results showed endoscopic transcanal approach was effective in the management of not only malformation involving any of the 3 ossicles but also aplasia or dysplasia of oval window. Moreover, compared with microscopic tympanoplasty, endoscopic surgery showed obvious advantages of a wide-angle and magnified view and minimal invasiveness 7,8 ; no related complications occurred in this research; however, some complications were reported in the literatures of microscope ossiculoplasty, such as sensorineural hearing loss, 13 -15 the transection of chorda tympani nerve, 9 and luxation of footplate. 15
The main goal of ossiculoplasty is to improve hearing; in the past decades, traditional microscopic surgery for congenital ossicular anomalies had achieved comfortable hearing outcomes. 1 -4,6,11 -16 Recently, Iannella et al 18 reported different material and methods for endoscopic ossiculoplasty, which showed a satisfied clinical–audiological outcome. In order to answer whether endoscopic ossiculoplasty could obtain a comparable hearing for ossicular chain malformation, we conducted a rapid systematic literature search for studies published in the past 2 decades, in which the hearing outcomes of microscopic ossiculoplasty were reported. Finally, a total of 10 articles with essential data were analyzed. However, only in the study of Wu et al, 9 a comparison between endoscopic and microscopic ossiculoplasty was performed, and it showed endoscopic ossiculoplasty achieved comparable postoperative hearing outcomes with less invasiveness and a shorter operation time. Therefore, we compared our cases with the cases of the literatures (Table 4). Our research showed a more favored hearing outcome; the hearing gain and ABG closure were both better than those in the literatures, and the proportion of ABG closure to 20 dB or less was 85.5% (14 ears) in this study, which was higher than most studies, but inferior to the study of Hashimoto et al. 6 However, in the study of Hashimoto et al, the proportion of reconstruction with piston prosthesis was obvious higher than this study (34.6% vs 12.5%), as many studies reported, 19,20 and the piston prosthesis usually obtains a better result. Moreover, though only half of these studies had stated the incision approach, 10,11,13,15, 16 as the view characteristic of microscope, an endaural or postauricular incision as well as additional scutum removal or canalplasty were frequently required for the visualization of the entire ossicular, 7,14 which could increase the risk of chorda tympani injury and possible ossicular trauma and sensorineural hearing loss induced by drill noise. 21,22 However, in this research, a more limited removal of the scutum was performed only in cases with oval windows and stapes pathology for adequate exposure, and no canaloplasty was needed.
Classification and Hearing Outcome of Ossiculoplasty in the Literatures.

Abbreviations: CT, chorda tympani never; EA, endaural incision; EO, endoscopic ossiculoplasty; MO, microscopic ossiculoplasty; NA, not available; PA, postauricular incision; SHNL, sensorineural hearing loss; TC, transcanal incision.
a It showed cases of ossicular chain malformation with syndromes, 5 ears in the study of Albert, 12 ears in the study of Thomeer et al, and 6 ears in the study of Thomeer et al.
b Sensorineural hearing loss was defined as>15 dB loss of bone conduction after surgery.
c Only cases with complete data were analyzed, 16 out of 17 ears in Vincent (2015), and 47 out of 64 ears in Tang (2018); however, as the classification proportion in Tang (2018), only the data of 64 ears was available.
This study found ICOCM usually involved malformation of the incus and stapes suprastructure, which was classified as type III according to the Teusnissen and Cremers classification system; however, this classification failed to consider the different deformities in the stapes suprastructure, which should be treated by different construction strategies. In this study, 13 eras with mobile footplate were further classified according to the status of stapes suprastructure, the cases with normal stapes suprastructure was performed with ossiculoplasty using PORP, and the cases with abnormal stapes suprastructure was performed with ossiculoplasty using TORP. It showed that ossiculoplasty using PORP achieved a more satisfactory hearing outcome. Therefore, in order to guide surgical treatment approaches, some researches proposed new classification criteria, which were mainly based on the incus–stapes complex or stapes suprastructure. 2,4,6 But most researches had a limited case, and a further multiple-center research with larger cases was needed in future. Moreover, the malformation with normal stapes suprastructure was usually involved the incus long process, and we classified 3 subtypes of long process anomalies according to the degree of missing (shown in Table 1 and Figure 1); to the best of our knowledge, this is the first study to describe different types of long process malformation which may help the selection of a more accurate ossiculoplasty strategy.
Conclusion
This research showed endoscopic surgery was effective in the diagnosis and management of ICOCM, and the endoscopic ossiculoplasty provides an alternative method to manage congenital ossicular chain malformation, with comfortable hearing outcome and the advantage of excellent vision and less invasion. Endoscopic ossiculoplasty can provide an alternative method for the management of ICOCM.
Supplemental Material
Supplemental Material, Sup_Fig_1 - Endoscopic Ossiculoplasty for the Management of Isolated Congenital Ossicular Chain Malformation: Surgical Results in 16 Ears
Supplemental Material, Sup_Fig_1 for Endoscopic Ossiculoplasty for the Management of Isolated Congenital Ossicular Chain Malformation: Surgical Results in 16 Ears by Chunlin Zhang, Jiaoping Mi, Dan Long, Yuan Deng, Qiang Sun and Zhaohui Liu in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
C.Z. and Z.L. participated in the design of the study. D.L., Y.D., and H.C. performed the statistical analysis, drafted the manuscript, and C.Z. revised the manuscript. All the authors have approved the manuscript as submitted. C.Z. and J.M. performed the statistical analysis, drafted the manuscript, designed the study, and later revised the manuscript. Data are available upon request by contacting the corresponding author. All authors have agreed to publish this article. This study was approved by the Institutional Ethics Review Board of the Affiliated Hospital of Zunyi Medical University and informed consent was obtained for our study from all participating patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81760493) and the Fund from Education Department of Guizhou Province for Young Scientific and Technological Talents (QKH NO. 2017-201).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.