
Abstract
The primary nasopharyngeal papillary adenocarcinoma (NPPA) is extremely rare which accounts for less than 0.48% of all malignant neoplasms in the nasopharynx. The clinical features, diagnosis, and treatment of NPPA have not been well described. We present 2 patients with NPPA that were treated with total endoscopic resection and radiotherapy at Vietnam National Cancer Hospital. Through these cases and reviewing of the literature, we provide deeper understanding of NPPA to highlight clinical pathological characteristics and the optimal treatment strategy for patients with pathologically confirmed NPPA. Our 2 cases were successfully treated and remained disease-free 4 years after treatment. The NPPA was usually an indolent tumor with polypoid appearance and slow growth rate and has a good prognosis. Surgical excision, including endonasal endoscopic excision with or without adjuvant radiotherapy, was most effective with a localized and operable tumor.
Introduction
According to the fourth edition of World Health Organization (WHO) in 2017, nasopharyngeal carcinoma was classified into the following subtypes: nonkeratinizing squamous cell carcinoma, keratinizing squamous cell carcinoma, basaloid squamous cell carcinoma, and nasopharyngeal papillary adenocarcinoma. 1 The primary nasopharyngeal papillary adenocarcinoma (NPPA) is extremely rare and accounts for less than 0.48% of all malignant neoplasms in the nasopharynx. 2 NPPA was an indolent tumor with polypoid appearance and slow growth rate. 3 Unlike conventional nasopharyngeal carcinoma, excellent prognosis and rare recurrence were observed in NPPA with appropriate surgical treatment, including transnasal endoscopic surgery. 4 To date, few cases have been reported in the literature. The clinical features, diagnosis, and treatment of NPPA have not been well described. We herein report 2 cases of women with primary NPPA, followed by a brief discussion on this rare disease.
Case Report
Case 1
A 48-year-old female patient with no specific medical history was referred to our hospital for a routine health checkup. Nasal endoscopy incidentally discovered a tumor in the roof of nasopharynx of approximately 10 mm in size (Figure 1). Nasopharyngeal tumor biopsy was performed and a pathology report was low-grade NPPA. Immunohistochemically, the tumor cell expresses EMA, CK7, TTF1 but not CK5/6, thyroglobulin, and Epstein-Barr virus (EBV), which support the diagnosis. Magnetic resonance imaging (MRI) showed moderate enhancement tumor located in the roof of the nasopharynx with size of 10 mm and absence of neck nodal metastasis (Figure 2). The chest and abdominal computed tomography (CT) scan and whole body scan showed no evidence of metastasis. The final diagnosis was primary papillary adenocarcinoma of nasopharynx, low grade, cT1N0M0, stage I. The patient underwent the total excision via nasal endoscopy, 4 in which the tumor on the nasopharynx roof was completely resected with surgical margin of approximately 1 cm. The postoperative pathology was consistent with the pretreatment one with negative margin. The patient then received postoperative radiotherapy (PORT) in 30 fractions with a total of 60 Gy for 6 weeks. She was discharged in July 2019. The patient is currently being followed up with no evidence of recurrence or distant metastasis or any posttreatment complications after 4 years.
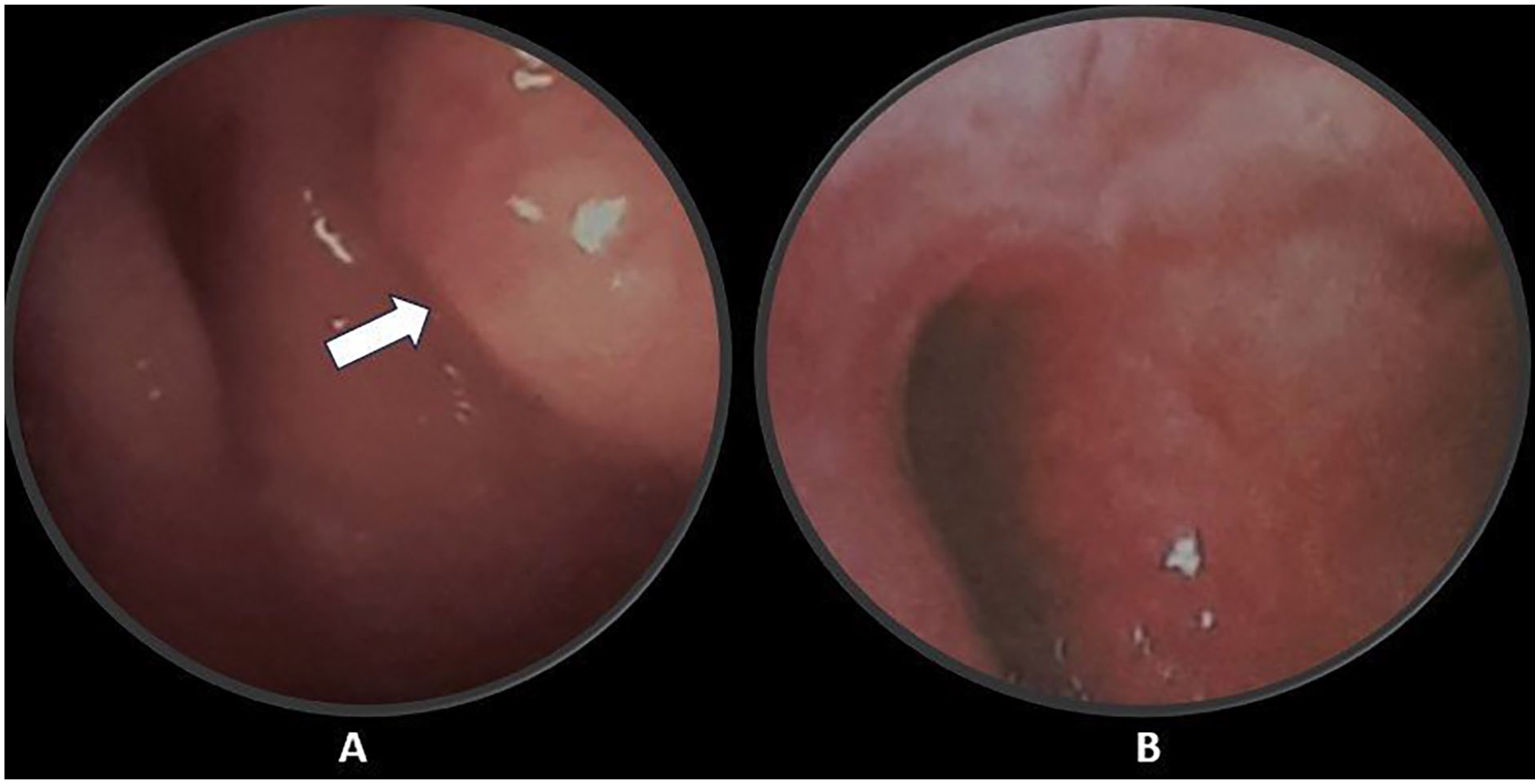
Nasopharyngoscopy (A) at the time of diagnosis, the nasopharyngeal tumor (arrow), and (B) no lesion was seen after 4 years.
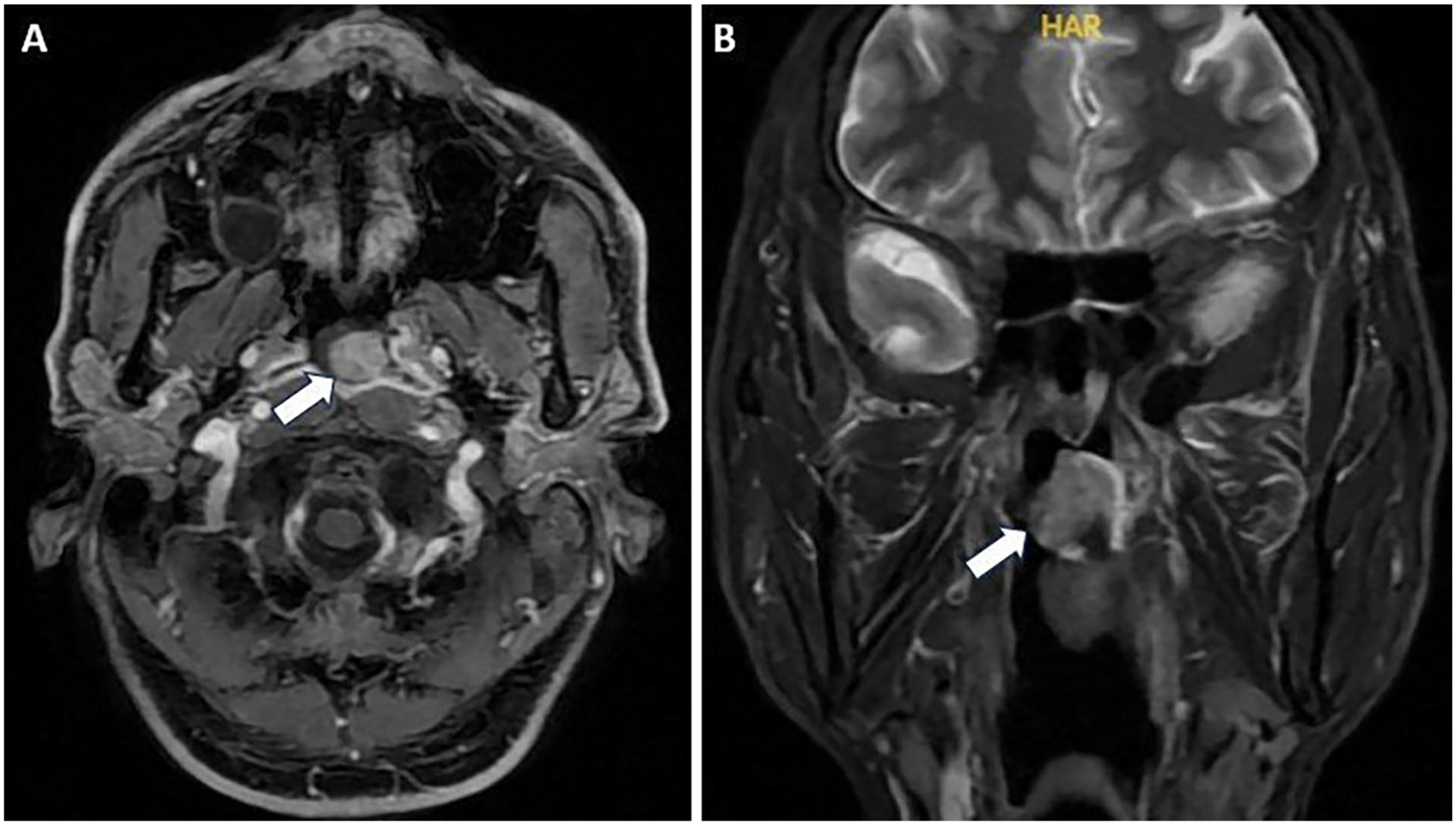
Magnetic resonance images showed the tumor located on the roof of the nasopharynx on the axial images (A, arrow) and the coronal images (B, arrow).
Case 2
A 50-year-old woman was admitted to our hospital with intermittent headaches and tinnitus in the right ear for 2 months. Nasopharyngoscopy assessment showed submucosal lesions on the roof of the nasopharynx (Figure 3). A biopsy was performed and diagnosed as NPPA. The MRI showed a tumor located on the roof of the nasopharynx with a size of 28 mm invading the parapharyngeal space (Figure 3). The patient was diagnosed with primary papillary adenocarcinoma of nasopharynx, T2N0M0. We performed a wide excision with nasal endoscopic assistance. In this operation, the tumor of 2 cm in size was completely excised with a surgical margin of 5 mm. Postoperative histology revealed a papillary adenocarcinoma with the margin of microscopic residual tumor (R1). She then received adjuvant radiotherapy in 30 fractions with a total of 66 Gy over 6 weeks and was discharged in November 2019. There was no evidence of recurrence or metastasis after 4 years of follow-up.
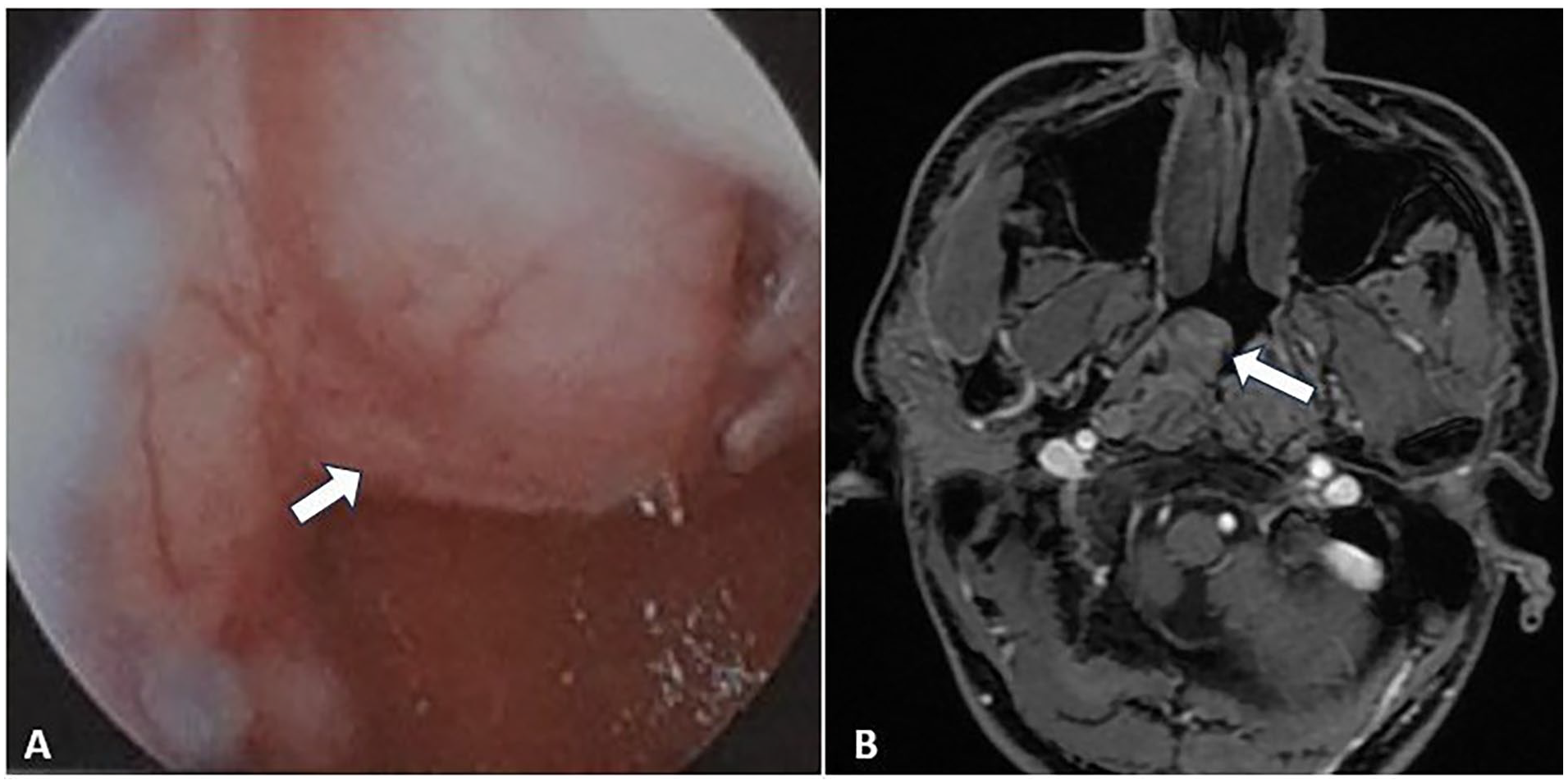
Nasopharyngeal tumor on nasopharyngoscopy (A) and magnetic resonance imaging (B).
Discussion
NPPA is rare with limited cases reported in the literature, first described in 1988 by Wenig et al. 5 Epidemiology, the largest previous study reported that patients range in age from 7 to 77 years with the median age of 41.5 years and the incident rate is higher in females with a female to male ratio of 1.5:1. 6 The other study showed that patients with NPPA were most commonly in their 30s, and there was no sex difference in its incidence. 7 However, a majority of nasopharyngeal cancers that originate from epithelium are closely related to the EBV infection. There is no evident base showing the association between nasopharyngeal papillary adenocarcinoma and the EBV. Furthermore, gene mutations such as KRAS, NRAS, BRAF, EGFR, and ALK have been reported as negative in some previous reports.1,8,9 Due to the scarcity of these neoplasms, further investigation is still needed to clarify the pathogenesis.
For clinical features, Table 1 shows the clinical characteristics of previously reported nasopharyngeal papillary adenocarcinoma. The tumors are commonly exophytic with a papillary, nodular or polypoid appearance. The main symptoms of TL-LGNPPA were nasal obstruction or nasal congestion, bleeding, and nasal or pharyngeal discomfort. 6 The tumors range from 0.3 to 4.0 cm and occur most frequently in the posterior or roof of the nasopharyngeal walls. 10 The tumors are commonly limited in the nasopharynx with good prognosis; in the study by Lai et al, 6 all patients were stage T1 with no nodal and distant metastasis; rarely in the case reported by Susilowati et al, 11 the tumors invaded the medial wall of the orbital cavity and bilateral node metastases. In our cases, demographic characteristics, including age, gender, tumor size, and location, match the previous reports.
Summary of Clinical Characteristics of Previously Reported Primary Nasopharyngeal Papillary Adenocarcinoma.
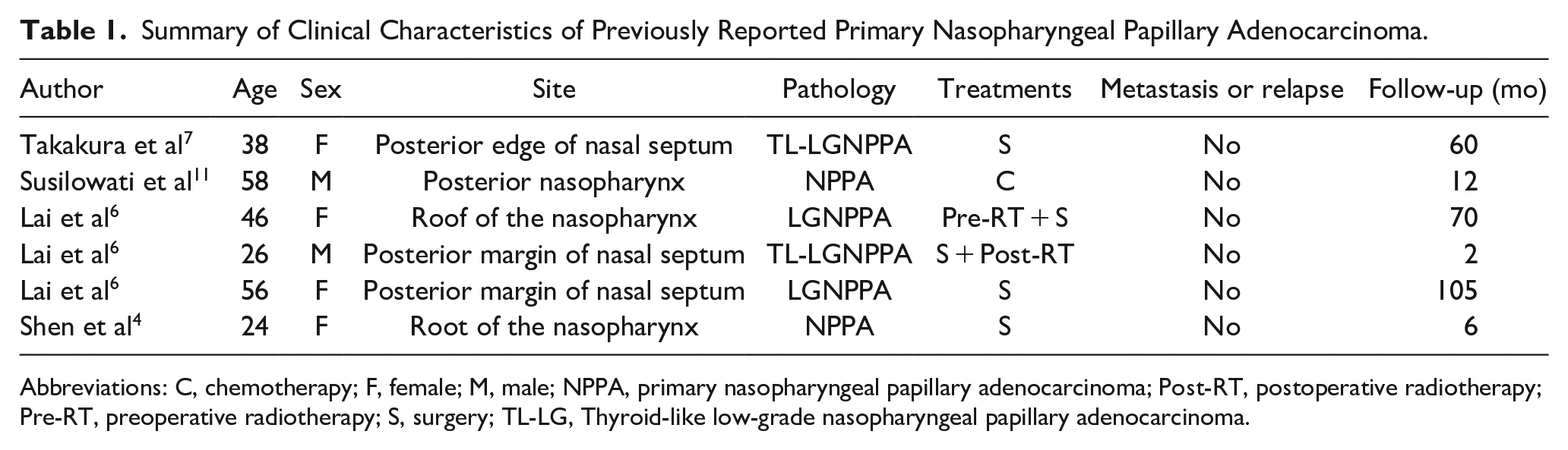
Abbreviations: C, chemotherapy; F, female; M, male; NPPA, primary nasopharyngeal papillary adenocarcinoma; Post-RT, postoperative radiotherapy; Pre-RT, preoperative radiotherapy; S, surgery; TL-LG, Thyroid-like low-grade nasopharyngeal papillary adenocarcinoma.
Histopathologically, low-grade NPPAs are characterized by papillary architecture with hyalinized fibrovascular cores and glands lined by cuboidal to columnar cells with a moderate amount of eosinophilic cytoplasm and round to oval nuclei with vesicular to clear chromatin which is similar to thyroid papillary adenocarcinoma. 7 Therefore immunohistochemistry (IHC) staining is critical to differentiate NPPA and metastatic thyroid papillary adenocarcinoma. 12 Thyroglobulin is usually detected in metastatic thyroid papillary adenocarcinoma, while NPPA is negative for thyroglobulin. Therefore, immunostaining of thyroglobulin is highly recommended to differentiate these 2 diseases. 7 Negativity for CK20, CD15, S-100, P40, P63, CK5/6, CDX-2, prostate-specific antigen and positivity for CK7, CK19, vimentin, and EMA on IHC can also support the diagnosis. 7
For the treatment, there was still no standard treatment for NPPA. Whether surgical treatment alone, solely radiotherapy or chemotherapy, or surgery combined with radiotherapy or chemotherapy remains controversial. According to the literature, unlike conventional nasopharyngeal carcinoma that was radiosensitive, radiotherapy or concurrent chemoradiotherapy was the first treatment for the local and advanced stage of tumor. NPPA is an indolent tumor with polypoid appearance and slow growth rate in which surgical excision, including endonasal endoscopic excision, was the most appropriate treatment for well-differentiated primary nasopharyngeal papillary. 4 A retrospective study by Liu et al 13 revealed that the overall survival in patients with T1 to T2 was significantly improved comparing combined surgical treatment group with the nonsurgical treatment group (radiotherapy; P = .041). Wenig et al 5 reported a case that failed with primary radiotherapy treatment and subsequently underwent surgical resection as salvage and had been free of disease over an 11 year period. The role of adjuvant radiotherapy after wide excision of early-stage NPPA is still unclear. The effectiveness of PORT has been emphasized in some reports. Lai et al 6 reported 2 cases without locoregional recurrence or distant metastasis after PORT. However, some authors revealed that the addition of PORT could not bring survival benefit, but increase toxicities for early-stage patients with clear margin and without adverse prognostic factors such as lymphovascular or perineural invasion. However, as the poorly differentiated or unresectable primary NPPA, it is highly radiosensitive and difficult to achieve the purpose of radical cure with surgery alone; definitive radiotherapy or chemoradiotherapy is considered as the primary treatment. Several reports revealed that photodynamic therapy (PDT) is a new treatment modality for head and neck cancers, with satisfactory treatment responses and minimal complications.14-16 In a study by Wang et al, 15 PDT combined with topical 5-aminolevulinic acid as an effective modality of postoperative adjuvant therapy was successfully used in the patient to eradicate residual disease with acceptable toxicities. The PDT could be promising for NPPA for its localization and low rate of nodal metastasis, but controversy exists due to the small sample size and limited number of studies. Both of our patients underwent surgery and adjuvant radiotherapy which currently show no signs of recurrent or metastasis.
Conclusions
Nasopharyngeal papillary adenocarcinoma is an extremely rare type with favorable prognosis. Surgical excision, including endonasal endoscopic excision with or without adjuvant radiotherapy, was most effective with localized and operable tumor. We report 2 cases of NPPA that were successfully treated with surgery and adjuvant radiotherapy.
Footnotes
Data Availability Statement
Original contributions presented in the study are included in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
Ethical approval is not required for this study in accordance with local guidelines. The authors declare that appropriate written informed consent was obtained from the patient for the publication of details of his medical cases and any accompanying images.