
Abstract

Significance Statement
Hyalinizing clear cell carcinomas (HCCCs) are a rare neoplasm. The distinct morphological features of HCCCs, particularly its clear cell appearance, can lead to diagnostic challenges, often resulting in misidentification with other more aggressive salivary gland malignancies, such as epithelial-myoepithelial carcinoma, mucoepidermoid carcinoma, and myoepithelial carcinoma. Given the generally favorable prognosis associated with HCCCs, accurate and timely differential diagnosis from other malignant salivary gland tumors is crucial for appropriate patient management.
A 75-year-old male patient presented to the Ear, Nose, and Throat (ENT) clinic with pain and swelling in the left half of the maxilla. ENT examination revealed a solid mass lesion causing mucosal ulcers on the left half of the soft palate. The patient was then referred to the radiology clinic and a computed tomography (CT) scan was performed.
CT scan and magnetic resonance (MR) images showed a solid mass lesion in the left half of the soft palate, 4 cm × 4 cm × 3.5 cm in size, extending to and eroding the left maxillary sinus walls, causing medullary expansion of the bony structures in the left maxillary sinus walls, almost completely occluding the maxillary sinus ventilation, extending to and partially obliterating the level of the left frontoethmoidal recess, and not containing calcification (Figure 1). A biopsy was performed.
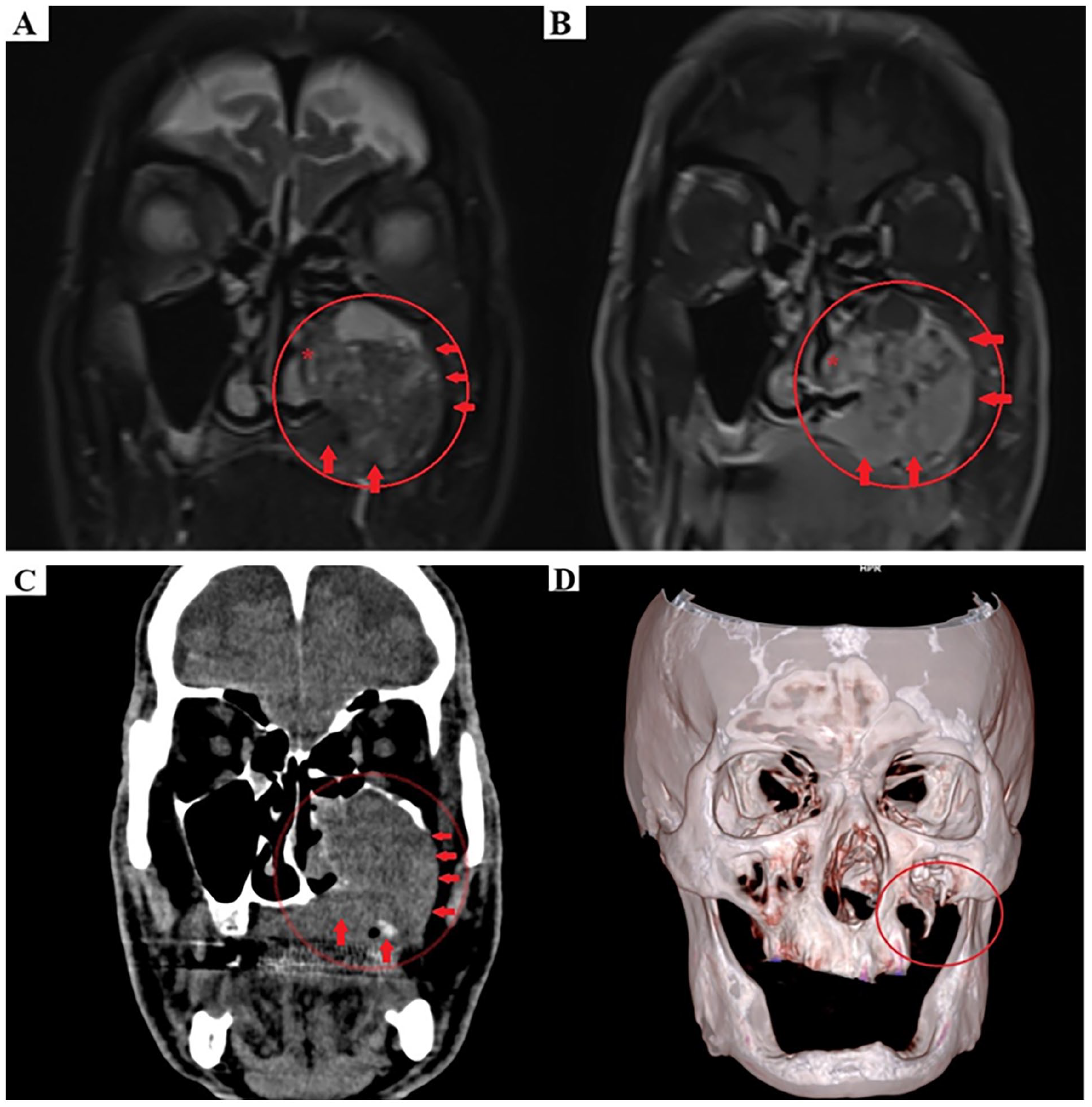
(A, B) Fat-suppressed T2-weighted sagittal MR (A) and contrast-enhanced fat-suppressed T1-weighted sagittal MR (B) images showed a solid mass lesion in the left half of the soft palate (circle), extending to and eroding the left maxillary sinus walls (arrow), extending to and partially obliterating the level of the left semilunar hiatus (star). (C) Noncontrast sagittal CT images show a solid mass lesion (circle) in the left half of the soft palate extending into the left maxillary sinus walls and eroding these structures (arrows). (D) Coronal CT 3D reconstruction images show that the inferior wall of the left maxillary sinus is eroded (circle). MR, magnetic resonance; CT, computed tomography.
In the pathological assessment of biopsy specimens; microscopic examination revealed small, rounded cells with clear cytoplasm and oval nuclei, which occasionally formed nests and intertwined cords in the subepithelial area of the oral mucosa. The stroma in the tumor-adjacent region exhibited a hyalinized appearance. Pleomorphism, atypical mitoses, or necrosis were not observed. Histochemical analysis did not detect the accumulation of mucin with either mucicarmine staining. While the cells exhibited positive staining with Periodic Acid-Schiff (PAS), the staining faded in Periodic Acid-Schiff Staining with Diastase (D-PAS) analysis (Figure 2).
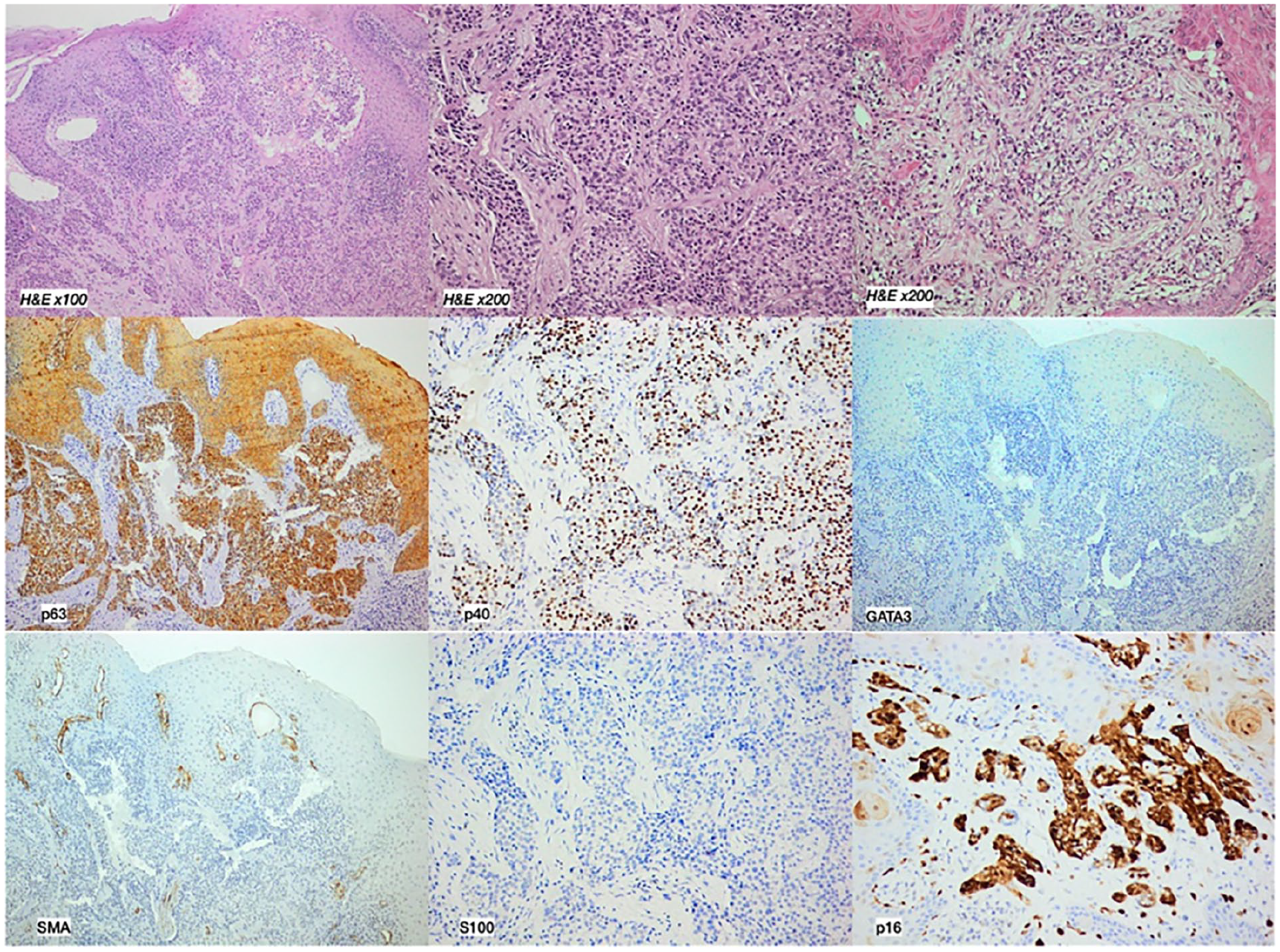
The carcinoma consists of cells with clear to eosinophilic cytoplasm, organized in elongated cords, interconnected trabeculae, and nests. The nuclei are positioned centrally and exhibit inconspicuous nucleoli. Immunohistochemical staining was conducted, yielding the following outcomes: positive expression of p63, p40 p16, while S100, SMA, and GATA3 was negative. SMA, smooth muscle actin.
Immunohistochemical examination revealed the expression of p63 and p40 in tumor cells, while no expression of SMA, calponin, CD10, RCC, GATA3, or S100 was observed. Diffuse strong staining was noted in p16 examination. The Ki-67 proliferation index was 1%.
The findings were interpreted as clear cell carcinoma (CCC) of the hyalinized type.
The tumor was then excised by ENT, final pathological examination confirmed the initial diagnosis based on biopsy. The patient then came for annual MR imaging follow-up. MR examination 1 year after the operation was normal. However, 2 years after the operation, a newly formed, round-shaped, contrast-enhancing solid recurrent lesion was observed in the operation area, obliterating the left ethmoidal cells (Figure 3).
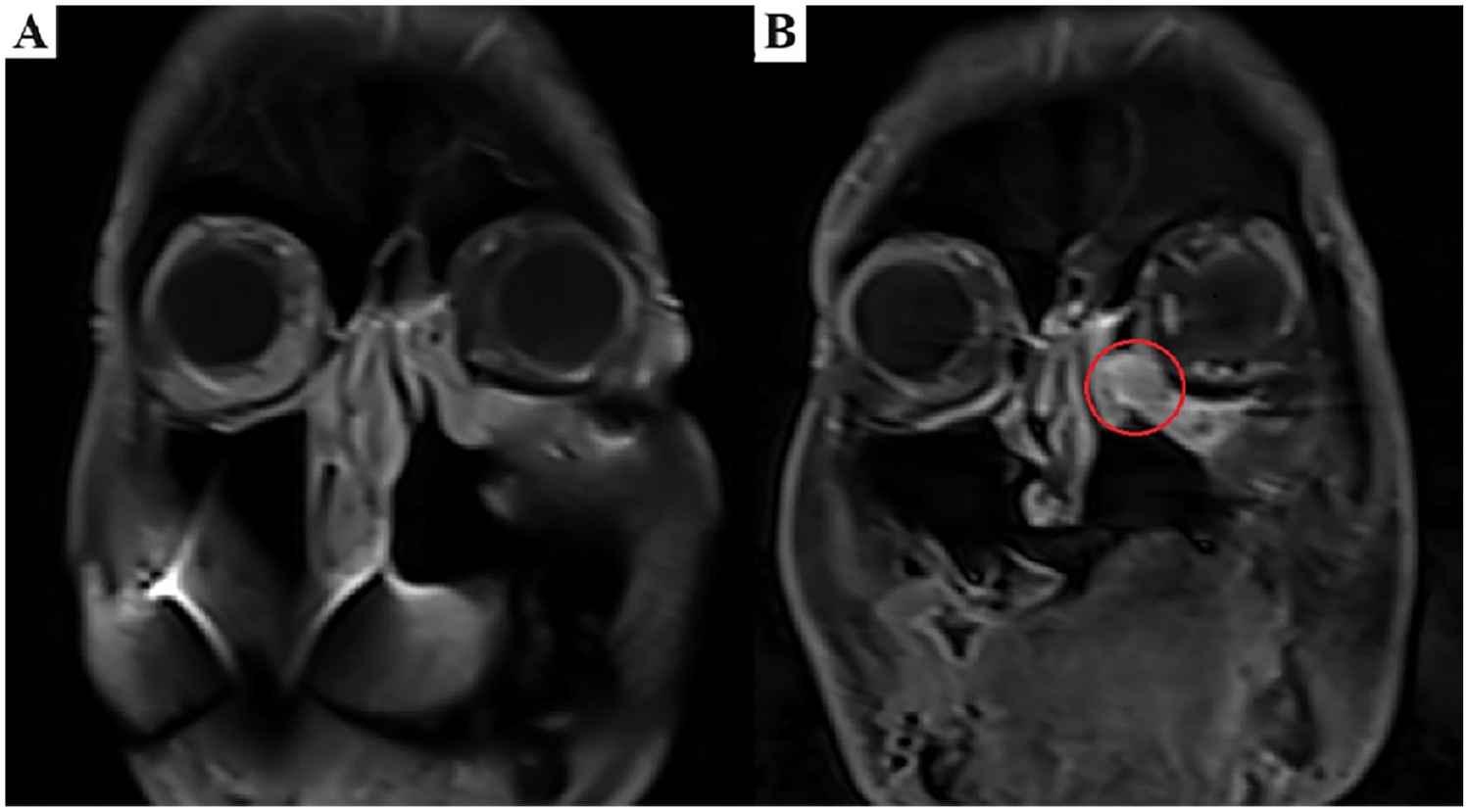
(A) Contrast-enhanced fat-suppressed T1-weighted sagittal MR images performed 1 year postoperatively, there is no lesion adjacent to the maxillary sinus wall. (B) Contrast-enhanced fat-suppressed T1-weighted sagittal MR images performed 2 years postoperatively, revealed a newly developed contrast-enhancing round-shaped soft tissue lesion (circle) adjacent to the left maxillary sinus wall, obliterating the left ethmoidal cells. MR, magnetic resonance.
CCC is a low-grade tumor formed of malignant cells with clear cytoplasm that accounts for fewer than 1% of all salivary gland malignant tumors and has a good prognosis. It generally appears in the fifth or sixth decade of life and affects women more than men.1-4
This neoplasm primarily localizes in the palate and the base of the tongue, with patients presenting either as asymptomatic or with diffuse ulcerated mucosal lesions accompanied by pain and swelling.3,4 As seen in our case, there is a 12% to 17% tendency for HCCC to reappear at the same site, and there have been several instances where the cancer has spread to nearby lymph nodes or distant parts of the body.5-7
Clear cells are PAS-positive, diastase-sensitive, and mucicarmine-negative because they contain glycogen. CCC also responds to low and high molecular weight keratin, anti-epithelial membrane antigen, and, in certain circumstances, carcinoembryonic antigen. In CCC, S-100 protein, muscle-specific actin, smooth muscle actin (SMA), myosin, and calponin all stain negatively, suggesting a lack of myoepithelial differentiation. 8
Histologic characteristics, on the other hand, are not pathognomonic for HCCC. Mucoepidermoid carcinomas, epithelial-myoepithelial carcinomas, clear cell odontogenic carcinomas, and metastatic lesions are among the HCCC differential diagnoses.9,10
Since mucin is found in the cytoplasm of clear cells in mucoepidermoid carcinoma, positive staining with mucicarmine may aid in the differential diagnosis. 2 In epithelial/myoepithelial carcinoma and malignant myoepithelioma, but not in HCCC, neoplastic cells stain positively with S-100 protein and SMA. 9
The contribution of particular stains to the distinguishing of CCC and odontogenic tumors is minimal; nonetheless, odontogenic tumors can be separated from CCC by a biphasic development pattern and positive staining for cytokeratin and S-100 protein. 11
In the differential diagnosis of hyalinizing CCC, metastatic malignancies such as renal cell carcinoma should also be examined. These individuals, however, frequently have a history of renal mass. These cancers stain positively with cytokeratin and vimentin in the presence of metastasis, whereas HCCC stain negatively with vimentin.
To conclude, a hyalinizing CCC is an uncommon minor salivary gland malignancy. It is sometimes mistaken with other aggressive salivary gland cancers with clear cells, such as epithelial-myoepithelial carcinoma, mucoepidermoid carcinoma, and myoepithelial carcinoma. The prognosis for hyalinizing CCCs is favorable. Therefore, it is critical to evaluate the patient clinicopathologically, obtain an accurate diagnosis, and follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.