
Abstract
Keywords
Introduction
Conductive hearing loss (CHL) results from abnormal sound transmission in the external, middle, and inner ears, 1 with various factors contributing to its occurrence, including genetic abnormalities, embryonic developmental issues, inflammation, trauma, and tumors.1,2 Among these, inflammation stands out as the most commonly identified cause.1-4 While most CHL patients can be diagnosed through comprehensive medical history and examination, instances of noninflammatory, nontraumatic CHL, with intact and normal tympanic membrane, present a diagnostic challenge. These cases lack significant abnormal signs, explicit audiological or imaging assessments results, and a history of otitis media or trauma, making it difficult to establish a clear diagnosis.2,5,6 This particular condition is referred to as unexplained conductive hearing loss (UCHL), and exploratory tympanotomy is the primary method employed for its diagnosis and treatment.2-8
UCHL arises from abnormalities in the middle ear’s sound transmission structure, manifesting primarily as CHL. Additional symptoms may include tinnitus, ear fullness, dizziness, and ear pain, and so on.3-10 Congenital UCHL often manifests since childhood or is incidentally discovered, while acquired UCHL, such as otosclerosis (OTS), develops gradually over time.8,11 Identifying the etiology of UCHL preoperatively proves challenging based solely on clinical manifestations, radiographic, and audiological examinations. Numerous previous articles have reported cases of preoperative diagnostic errors or difficulties. The objective of this article is to review and summarize the clinical characteristics of various types of UCHL reported in the literature, analyze factors affecting diagnosis, and evaluate the benefits of surgical treatment along with potential complications. This information aims to enhance the management and treatment of such diseases in clinical practice.
Materials and Methods
A comprehensive literature search was conducted across multiple databases, including PubMed, Embase, Web of Science, and Cochrane, focusing on the theme of “conductive hearing loss with an intact tympanic membrane.” The search terms utilized were “conductive hearing loss” and “intact tympanic membrane.” Two researchers carried out the literature review independently, culminating in a final search on September 30, 2023. Adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 642 articles were identified; after eliminating duplicates, 458 articles remained. A detailed flowchart of the study process can be found in Figure 1.
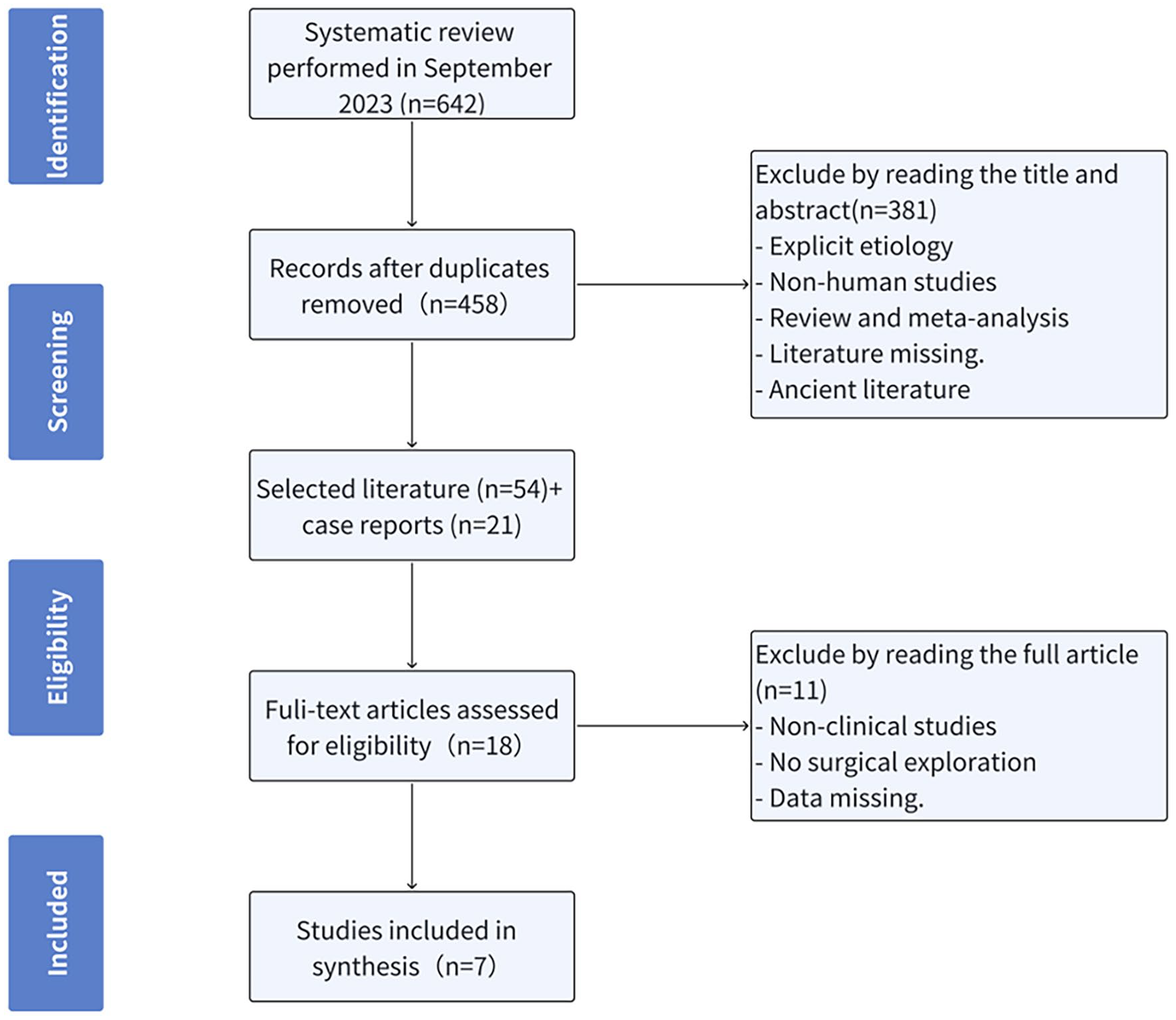
Project flow chart. Literature evaluation and selection, according to PRISMA criteria (http://www.prisma-statement.org/). PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Exclusion criteria were: (1) various lesions or deformities of the external auditory canal; (2) tympanic membrane perforation; (3) inflammatory middle ear diseases such as secretory otitis media, suppurative otitis media, and so on; (4) sensorineural hearing loss; (5) congenital external ear malformation or genetic syndromes associated with hearing loss; (6) traumatic hearing loss; (7) jugular vein tumors; (8) animal experiments, cadaver studies; (9) conference abstracts, reviews, and meta-analyses; (10) missing references or articles published before 2003. In cases where the title and abstract did not clearly fit into any of the aforementioned criteria, the full text of the research report was reviewed to assess its relevance to this study. A total of 54 research articles were obtained, along with 21 case reports.
From the initial pool of 54 research articles, a refined selection process was undertaken to specifically extract literature related to UCHL. Full-text articles assessed for eligibility: (1) observational studies and experimental studies; (2) focus on CHL without deliberate exclusion or inclusion of specific major diseases; (3) confirmation of diagnosis through exploratory tympanotomy, with detailed reporting of general patient information, surgical procedures, and follow-up details. Seven retrospective studies met these criteria, and the extracted information included author details, publication year, sample size, general patient information, examinations, treatment measures, and outcomes.
On a thorough examination of the full texts, researchers observed that among the excluded inflammatory and traumatic cases, reported subtypes of CHL included congenital ossicular anomalies (COA), OTS, congenital middle ear cholesteatoma (CMEC), among others. The study then proceeded to succinctly summarize the primary diagnostic and therapeutic characteristics associated with each identified subtype.
Results
Characteristics of Various UCHL Diseases
In our systematic literature review, we purposefully excluded factors like inflammation and trauma, which are known to contribute to CHL. Our findings revealed that UCHL encompasses a spectrum of conditions, including (COA, OTS, CMEC, oval window atresia (OWA), superior semiregular-canal bony dehiscence, congenital stapedial footplate fixation (CSFF), middle ear osteoma, middle ear adenoma, congenital ossification of stapedial tendon (COST), among others.
Among these conditions, COA, OTS, and CMEC emerged as the most prevalent types, as supported by references.2,4,5,8,9,12-15 Conceptual maps illustrating various UCHL diseases are presented in Figure 2. The subsequent section provides a concise summary of the key characteristics associated with each disease type.
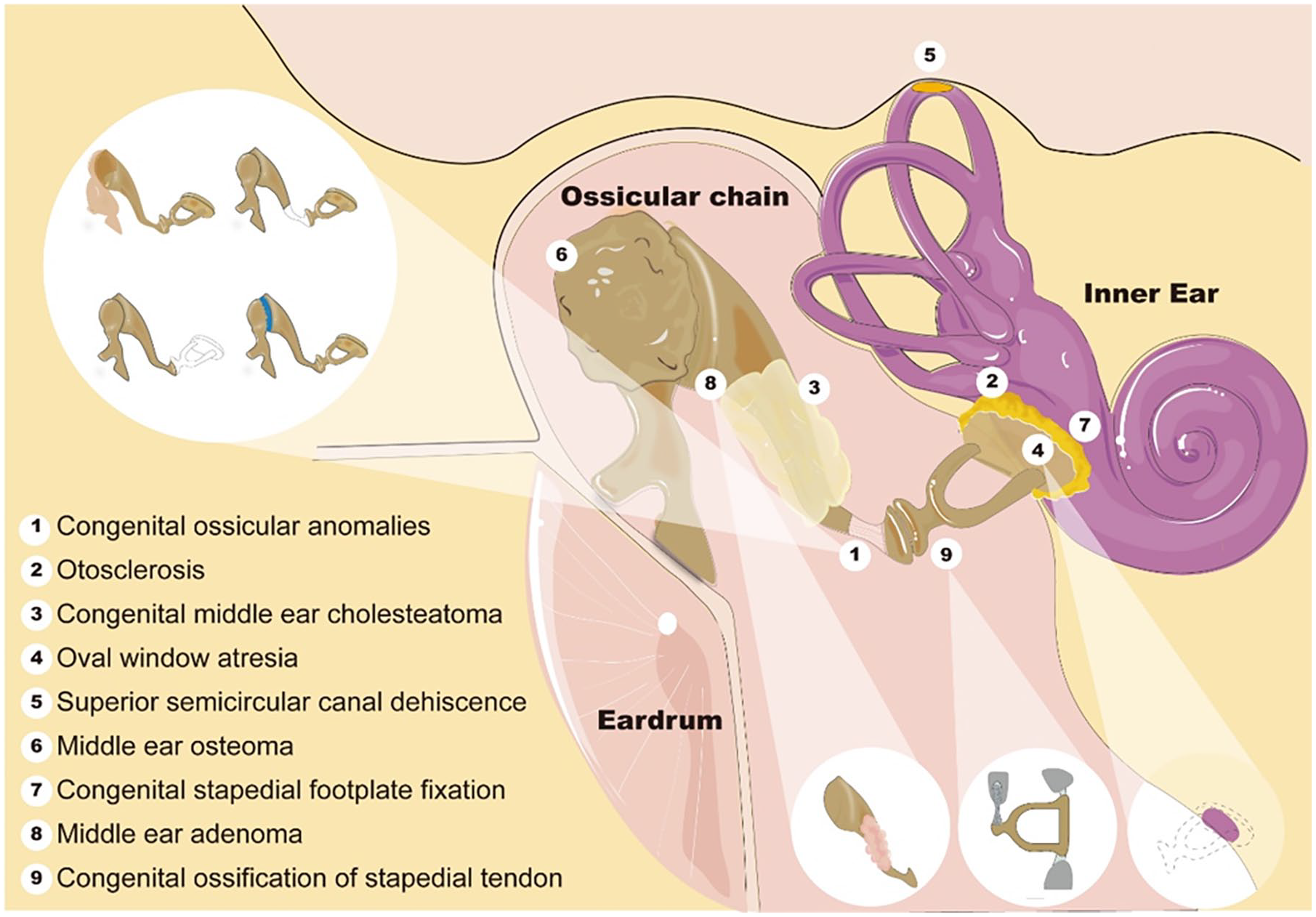
The conceptual maps of various UCHL diseases. UCHL, unexplained conductive hearing loss.
Congenital ossicular anomalies
COA represent the most prevalent form of UCHL, 3 stemming from abnormal development in the first or second pharyngeal arches during embryonic stages.16,17 In a study by Yang and Liu, 18 it was observed that 50.9%, 48.0%, and 18.3% of patients exhibited deformities in the stapes superstructure, incus, and malleus bones, respectively. In addition, anomalies such as CSFF, OWA, and facial nerve abnormalities may coexist. The typical manifestation of COA includes moderate to moderate-severe unilateral hearing loss, often accompanied by symptoms like tinnitus and ear fullness.5,16 Temporal bone s (HRCT) is a crucial diagnostic tool, although its success rate is deemed unsatisfactory. Nevertheless, sensitivity can be enhanced through post-processing imaging techniques.19-21 Zhang et al 22 highlighted that the long crus deformity of the incus, stapes superstructure deformity, and OWA are readily identified in preoperative HRCT, while ossicular fixation is prone to being overlooked. The primary method for treating COA is endoscopic ossicular reconstruction.3,16,23
Otosclerosis
OTS is characterized by spongy degeneration in the bony labyrinth of unknown cause. 24 Potential contributing factors include genetics, environmental influences, viral infections, and autoimmune factors. 25 This condition predominantly affects middle-aged individuals, particularly women, 5 presenting as bilateral progressive moderate to moderate-severe CHL.5,24,26 In cases where the cochlea is involved, mixed deafness may ensue, 22 often accompanied by symptoms such as tinnitus and ear fullness.5,24 Typical findings on HRCT include abnormal low-density areas around the vestibular window and cochlea.12,24 However, there exists considerable variability in sensitivity, 20 possibly attributable to differences in disease severity and equipment. 24 Studies indicate higher radiological sensitivity during the active phase of OTS (76.3%) compared to the inactive phase (61.9%). 26 Diagnosis primarily relies on typical symptoms and examinations, with confirmation requiring intraoperative evaluation of the mobility of the stapes footplate. The treatment involves implanting a piston following the fenestration of the stapes footplate,5,27 leading to a significant improvement for approximately 90% of patients.11,24,25,28,29
Congenital middle ear cholesteatoma
CMEC manifests as an invasive lesion, likely originating from residual ectodermal squamous epithelium.17,20,30,31 This condition is clinically rare, primarily observed in children, 5 accounting for roughly 2% to 5% of all middle ear cholesteatoma cases.30,32 Initial symptoms tend to be mild, 33 typically manifesting as unilateral CHL in childhood. As the condition progresses, patients may experience sensations of ear fullness, otorrhea, dizziness, and even facial paralysis.5,17,31 Endoscopic examinations often reveal pearly-white mass-like structures on the inner surface of the eardrum,30,32 while HRCT displays intratympanic quasi-circular soft tissue density shadows. 20 Zhao et al 17 suggests a comprehensive preoperative radiographic assessment and surgical exploration for any soft tissue density shadows within the tympanic cavity of UCHL patients to rule out the presence of minute cholesteatoma. Early suspected cases should undergo surgical intervention primarily focused on complete cholesteatoma removal rather than hearing improvement.6,31,32 The typical surgical approach involves endoscopic endoaural incision, occasionally supplemented by microscopic mastoid incision when required, followed by long-term follow-up care. 31
Oval and round window atresia
Oval and round window atresia (ORWA) is a congenital malformation within the labyrinthine wall, with OWA being the more prevalent subtype.34,35 It may coincide with other external and middle ear deformities. 36 The key symptom involves moderate to severe CHL since childhood. HRCT often reveals irregularities or absence of the oval or round window, frequently accompanied by additional middle ear malformations. 35 Su et al 35 reported that 69.1% of ORWA patients lacked a long crus of the incus, 61.9% lacked the stapes, 45.1% had stapes superstructure deformities, and 69.1% exhibited facial nerve abnormalities. The primary treatment approach involves vestibule fenestration, although its efficacy remains suboptimal.34-36 Henkemans et al 36 reported long-term success rates ranging from 12.5% to 75%, alongside several postoperative complications.
Superior semicircular canal dehiscence
Superior semicircular canal dehiscence (SSCD) is a condition resulting from a bony wall defect in the superior semicircular canal.12,37 This condition is also referred to as the “third window lesion” and may be associated with genetic, infectious, or traumatic factors. 12 Typical patients, predominantly middle-aged and elderly individuals, manifest vestibular-cochlear symptoms indicative of SSCD syndrome, including episodic vertigo, CHL, and tinnitus.12,15 Although HRCT is instrumental in identifying defects in the superior semicircular canal, such abnormalities can occasionally go unnoticed. 37 For mild SSCD symptoms, conservative treatment may be sufficient, but severe cases often necessitate surgical interventions like superior semicircular canal plugging and reinforcement.12,37
Middle ear osteoma
Middle ear osteoma represents a rare, slow-growing osseous tumor that originates within the tympanum.38-40 While its exact etiology remains unclear, the most frequent location of origin is the tympanic promontory (39.5%), 38 often observed in younger individuals. A hallmark presentation includes unilateral CHL, accompanied by tinnitus and sensations of ear tightness. However, smaller osteomas can remain asymptomatic.38-41 Otoscopy might disclose a creamy-white mass situated on the inner surface of the eardrum. 38 Concurrently, HRCT imaging can indicate a localized, high-density bony lesion within the tympanum, potentially showing fusion with the ossicular chain or the tympanic wall. 39 During exploratory tympanotomy, one may encounter a bone-like neoplasm that has integrated with the adjacent bone tissue. Such lesions can be challenging to fully excise, often necessitating the use of a bone drill. 38 Fortunately, with ossicular reconstruction, hearing improvement is achievable in the majority of cases.39-41
Congenital stapedial footplate fixation
CSFF is a nonprogressive CHL that manifests from childhood and is linked to the abnormal development of the annular ligament of the oval window in the embryo, potentially accompanied by other ossicular anomalies.42-44 It is important to differentiate CSFF from juvenile otosclerosis (JO), a progressive condition that may have a familial history.42,45 CSFF is characterized by poor hearing, often with an air-bone gap (ABG) exceeding 30 dB.42,46 Some studies suggest that in HRCT, attention should be given to abnormalities in the dimensions of the pyramidal eminence and the aperture of the stapedial tendon, which may be more significant than stapes footplate fixation.44,46 Surgical intervention for CSFF is similar to that for OTS, but the treatment outcomes are notably less favorable.42,45
Neuroendocrine adenomas of the middle ear
Neuroendocrine adenomas of the middle ear (NAME) are rare, benign, and slow-growing primary tumors of the middle ear with an extremely low incidence.47,48 The exact etiology of NAME is unclear, 49 but it may originate from neural crest stem cells. 48 Clinical manifestations include CHL, possibly accompanied by sensations of ear fullness, tinnitus, and ear pain. Otoscopic examination may reveal a nonpulsatile white or pink mass on the inside of the eardrum. HRCT and magnetic resonance imaging typically show a nonvascular lesion enveloping the ossicles without causing bone destruction, and it may potentially invade the posterior tympanum and the pharyngotympanic tube. 50 NAME exhibits invasive characteristics.47,50 The treatment principle for NAME involves complete tumor resection, followed by pathological and immunohistochemical evaluation to assess the nature of the tumor. 49 Adjuvant radiation or chemotherapy may be considered in certain cases, and long-term monitoring is essential to detect recurrence, progression, or metastasis.47,48
Salivary gland choristoma in the middle ear
Salivary gland choristoma in the middle ear is an infrequent congenital tumor. 51 It is posited to arise from the abnormal development of the second branchial arch in the early embryo, leading to the heterotopic location of salivary gland tissue in the tympanum. This condition may potentially be accompanied by other malformations within the middle ear.52,53 Clinical manifestations typically include unilateral CHL, possibly accompanied by symptoms such as tinnitus, ear fullness, and facial paralysis. 51 HRCT unveils a well-defined soft tissue mass surrounding the ossicles in the middle ear without any evidence of bone destruction. 53 The recommended course of treatment involves the complete excision of the tumor and subsequent reconstruction of the ossicular chain. Pathological examination plays a crucial role in confirming the salivary gland origin of the mass, 51 and the overall prognosis for patients is generally favorable. 53
Congenital ossification of stapedial tendon
COST is a rare hereditary middle ear disease.54,55 This condition presents as unilateral or bilateral CHL,54,56 posing a diagnostic challenge as it is difficult to differentiate from OTS and CSFF in the preoperative phase. 55 HRCT imaging may reveal linear, bony density shadows extending from the pyramidal eminence to the stapes superstructure. 55 A definitive diagnosis requires exploratory tympanotomy, during which intraoperative observation reveals ossification of the stapedial tendon along with poor mobility of the stapes. The restoration of stapes mobility can be achieved by releasing the stapedial tendon, leading to a favorable auditory prognosis.55,56
Analysis of Articles About UCHL
Following careful screening by 2 researchers, we analyzed data from 7 articles to comprehensively examine symptoms, diagnosis, and treatment of UCHL.3-5,7-10 The cohort comprised 522 patients, including 151 cases of COA, 93 cases of OTS, 205 cases of CMEC, 5 cases of COA and CMEC, and 9 cases of COWA. In addition, 59 cases were linked to traumatic or inflammatory factors. COA, OTS, and CMEC emerged as the primary contributors to CHL with intact tympanic membranes. Detailed information is meticulously documented in Tables 1 to 3. Consistent with prior literature, COA and OTS were identified as prevalent causes of UCHL across pediatric and adult populations. It is worth noting that the study by Xu et al 5 significantly influenced the CMEC cases, potentially leading to an overestimation of the proportion of CMEC in our study.
Number of Ears and Types of Diseases Reported in the Literature.
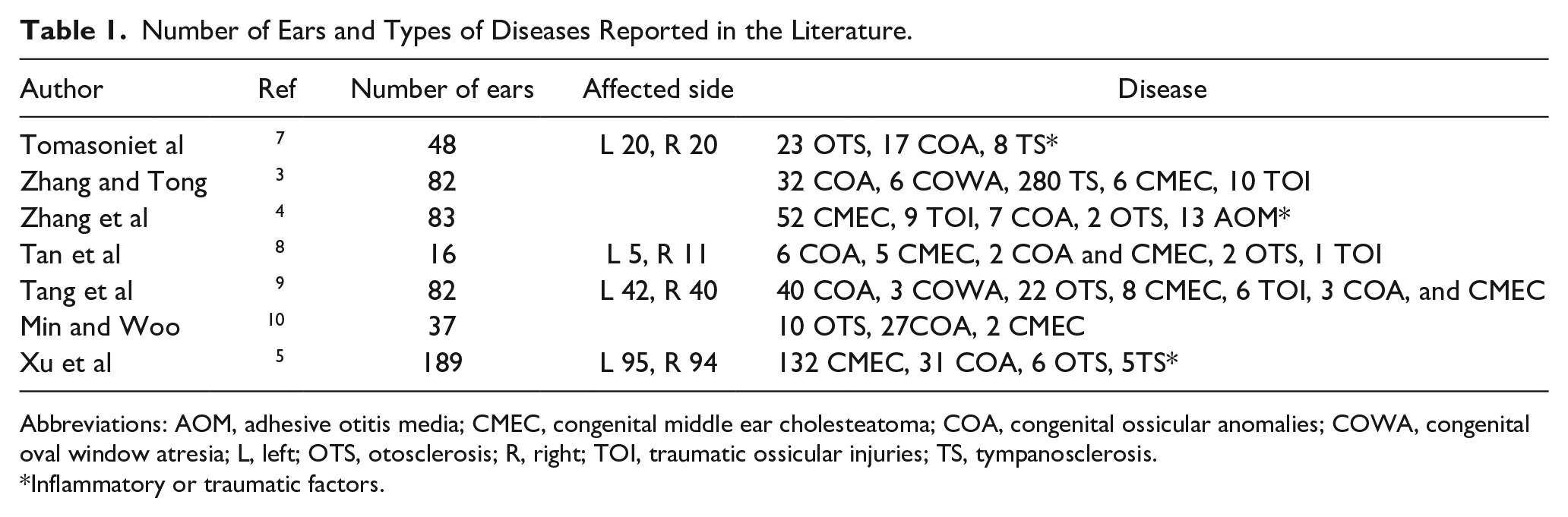
Abbreviations: AOM, adhesive otitis media; CMEC, congenital middle ear cholesteatoma; COA, congenital ossicular anomalies; COWA, congenital oval window atresia; L, left; OTS, otosclerosis; R, right; TOI, traumatic ossicular injuries; TS, tympanosclerosis.
Inflammatory or traumatic factors.
Demographic Information.
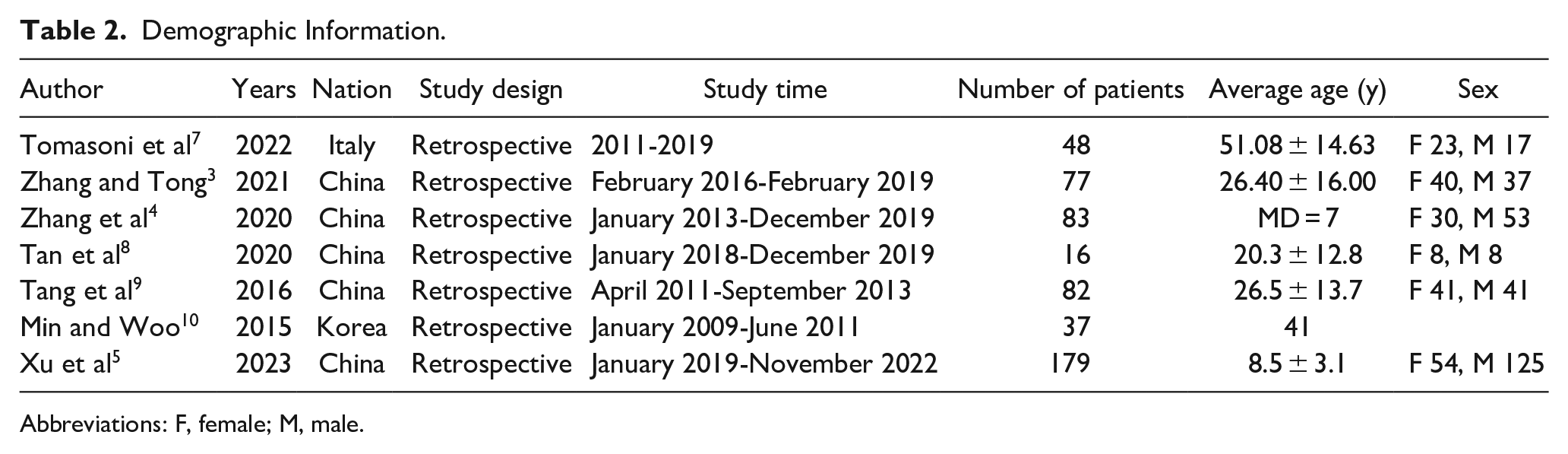
Abbreviations: F, female; M, male.
Number of Ears for Different Diseases Reported in Each Article.
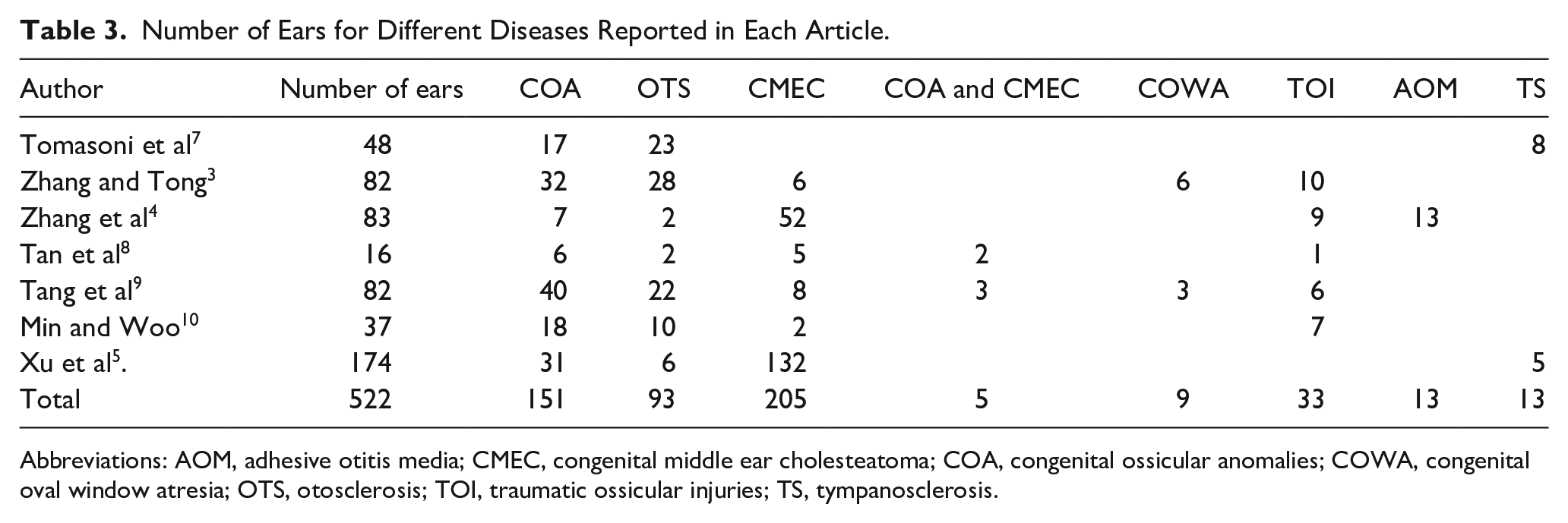
Abbreviations: AOM, adhesive otitis media; CMEC, congenital middle ear cholesteatoma; COA, congenital ossicular anomalies; COWA, congenital oval window atresia; OTS, otosclerosis; TOI, traumatic ossicular injuries; TS, tympanosclerosis.
Of the 7 articles, 5 are from China and 2 are from South Korea and Italy, respectively. The publication dates extend from 2015 to 2023, encompassing retrospective studies, as comprehensively summarized in Table 2. On closer examination, 2 articles specifically reported pediatric cases,4,5 with the youngest patient recorded at 2 years old. Furthermore, a solitary article exclusively focused on adult patients over 18 years old. 7 The average age of patients in the remaining literature ranged from 20 to 41 years old.3,8-10 Notably, excluding factors such as inflammation and trauma, the incidence of OTS in the 2 articles pertaining to pediatric patients was markedly lower than that reported in other literature. Moreover, there is a discernible trend of increasing incidence with the average age of patients (P = .009, Figure 3).
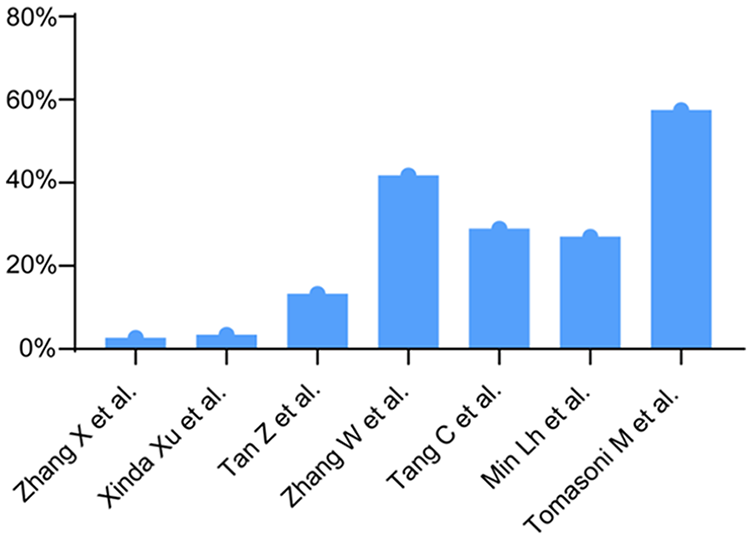
Proportion of OTS patients with average age. OTS, otosclerosis.
The predominant symptoms observed in patients with UCHL encompass hearing impairment, tinnitus, along with sensations of dizziness, ear stuffiness, ear pain, and facial paralysis.3,5,8-10 Among patients diagnosed with COA, 87.5% to 93.0% exhibit CHL that manifests from childhood, with an associated tinnitus incidence of 15.6% to 30.2%.3,5,9 In contrast, OTS patients, ranging from 86.4% to 96.4%, present with progressive CHL, and a tinnitus incidence ranging between 60.1% and 90.9%.3,5,9 TOI results in immediate hearing loss, accompanied by tinnitus in 50.0% to 80.0% of cases.3,9 The duration of the disease was reported in 5 articles,4,5,7-9 spanning from 7 days to 50 years. In addition, 3 articles delved into the positive rate of temporal bone CT in preoperative diagnoses of noninflammatory CHL with an intact tympanic membrane, with rates ranging from 33.8% to 87.1%.4,5,8 Specifically, COA demonstrated rates of 28.6% to 64%, while CMEC exhibited rates of 83.3% to 100%. The observed differences were significant, potentially attributable to the superior capability of temporal bone CT in identifying abnormal low-density shadows within the tympanic cavity.
All studies employed exploratory tympanotomy to confirm the etiology of CHL. Among them, 2 articles explicitly detailed the use of an endoscope for surgical procedures,3,8 1 utilized a microscope, 9 and another employed both. 10 Comprehensive final diagnostic results from all studies are consolidated in Table 3.
Each article conducted preoperative and postoperative assessments of average hearing thresholds (Pure-tone averag, PTA) and ABG at frequencies of 0.5, 1, 2, and 3/4 kHz. The collective PTA and ABG values from 7 articles are summarized in Table 4. The studies universally analyzed hearing outcomes by comparing preoperative and postoperative PTA and/or ABG. Specifically, 4 articles reported the primary hearing indicators (PTA and/or ABG) before and after surgery for each disease,3,5,7,9 and detailed information is presented in Table 5. The follow-up duration in all cases exceeded 3 months. Overall, most patients achieved good hearing recovery goals.
Postoperative Hearing Improvement and Complications.
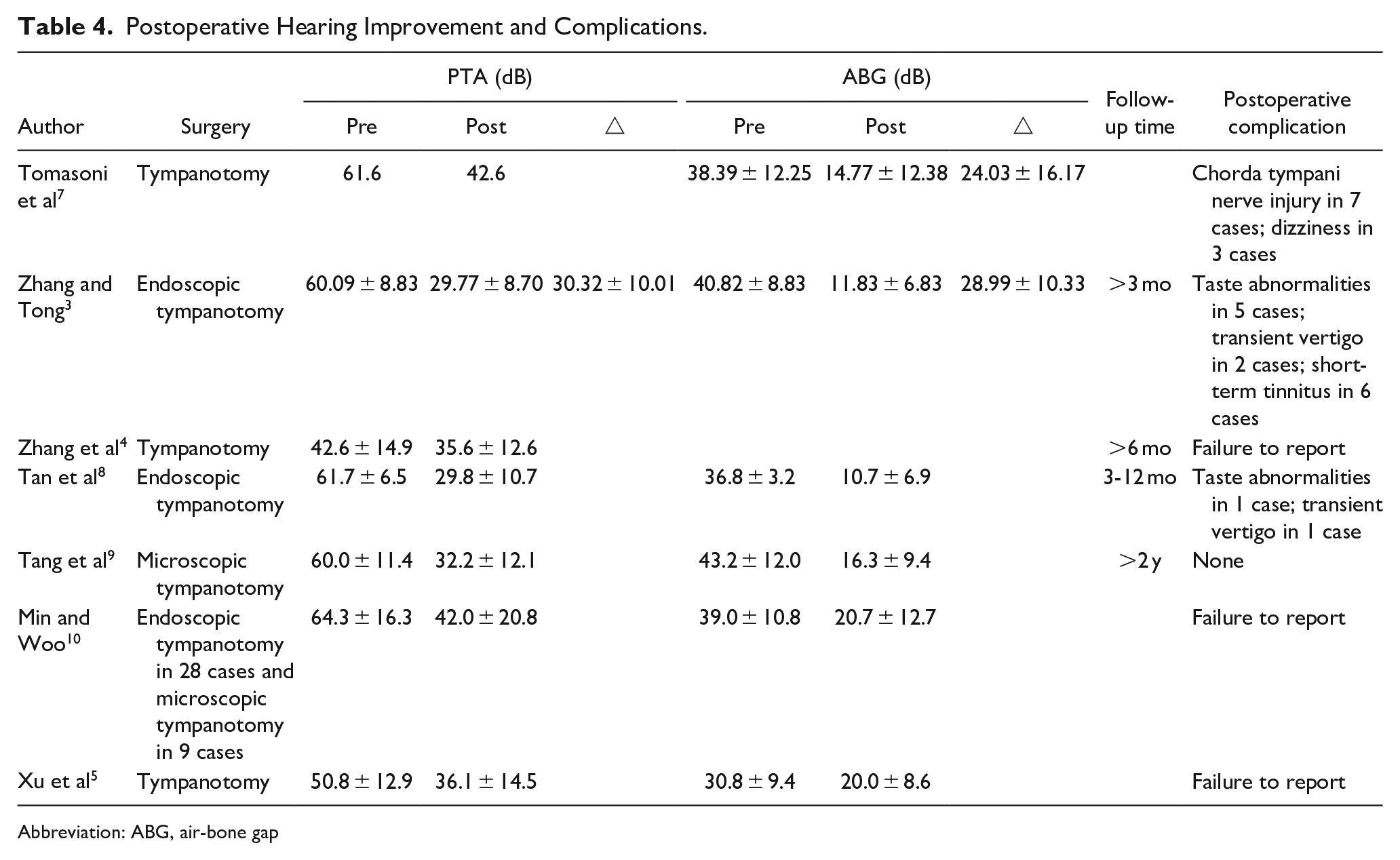
Abbreviation: ABG, air-bone gap
Preoperative and Postoperative Audiological Data of Different Diseases (Excluding Traumatic Inflammation).
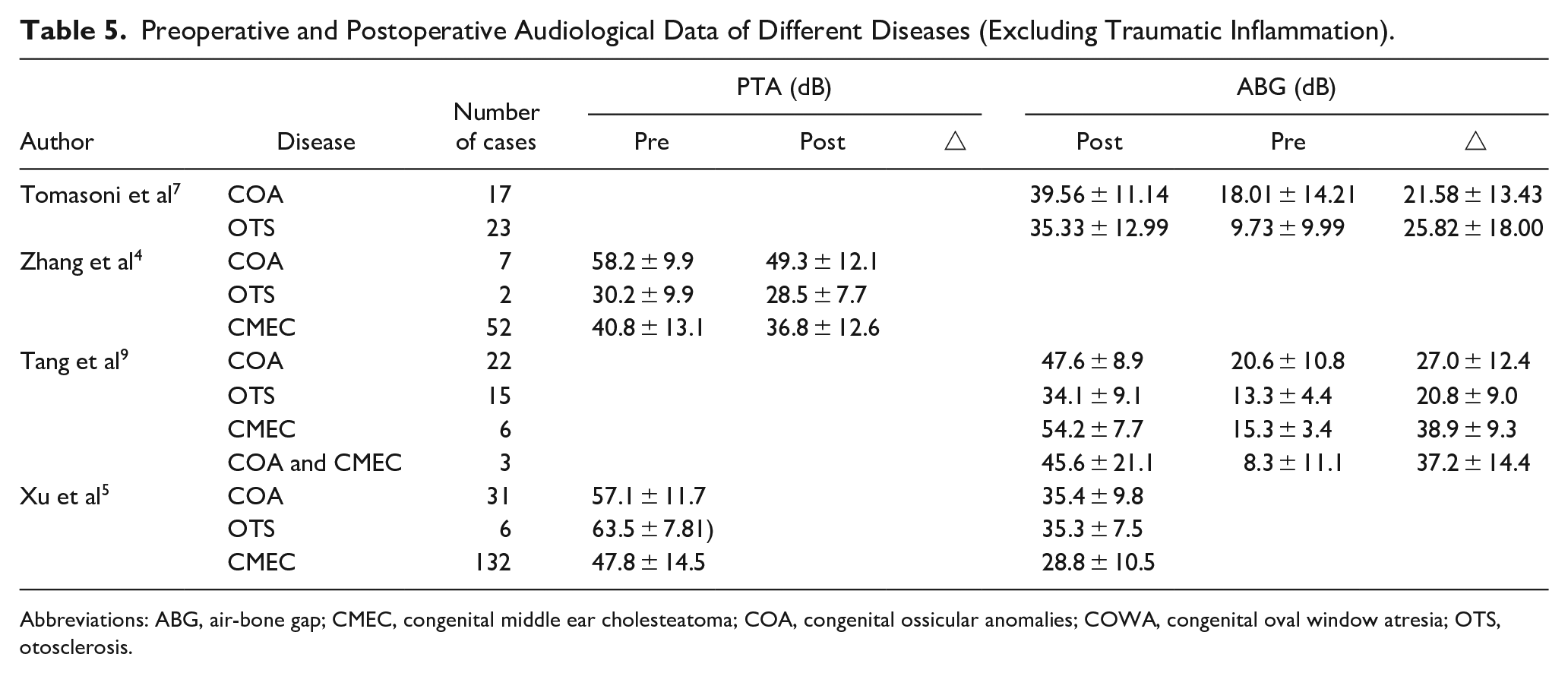
Abbreviations: ABG, air-bone gap; CMEC, congenital middle ear cholesteatoma; COA, congenital ossicular anomalies; COWA, congenital oval window atresia; OTS, otosclerosis.
Four articles have documented postoperative complications.3,7-9 The detailed information is presented in Table 4. Common postoperative complications include taste disorders, tinnitus, and dizziness. Taste disorders are primarily attributed to damage to the chorda tympani nerve during surgery, with the potential for gradual recovery over time if the chorda tympani nerve is not completely severed. Tinnitus and dizziness are predominantly short-term or transient postoperative complications with a favorable prognosis. None of the reviewed articles reported severe complications such as sensorineural hearing loss, facial paralysis, or intracranial infection.
Discussion
UCHL encompasses a spectrum of diseases characterized by common clinical presentations, specifically CHL with an intact tympanic membrane and the absence of inflammation or trauma history. Diagnosis solely based on preoperative examination poses challenges. Consequently, exploratory tympanotomy becomes imperative for a meticulous inspection of the middle ear’s structure, aiming to eliminate middle ear pathology and enhance hearing.3,5,7,21,22,27,57 Common UCHL diseases include COA, OTS, CMEC, OWA, SSCD, CSFF, middle ear osteoma, middle ear adenoma, COST, and so on.2-9,12,15,35,38,41,42,47,51,55
UCHL can significantly affect patients’ quality of life, especially children in crucial speech development stages. The literature suggests that children affected by CHL might delay seeking medical attention due to limited cognitive ability, a lack of medical awareness, and a tendency to adapt or endure symptoms. 18 In a study conducted by Xu et al, 5 involving 179 children with noninflammatory CHL, the average time from parents recognizing symptoms to a confirmed diagnosis was 2.2 ± 2.9 years. The shortest diagnostic duration was observed in cases of CMEC (average 1.3 years), while cases related to ossicle defects or OTS took approximately 5 years. This discrepancy might be attributed to CMEC exhibiting more invasive symptoms, whereas the latter 2 primarily cause hearing loss with a singular symptom. Shin et al 58 suggests that delaying the identification of cholesteatoma in children could lead to more extensive erosion, poorer hearing outcomes, and an increased risk of recurrence. Hence, it is crucial to pay close attention to any abnormal speech or behavioral signs in children, and suspected UCHL cases should be promptly referred to a hospital. In addition, regular hearing screenings for school-age children prove to be an effective method to detect concealed instances of UCHL.
Given the potential risks associated with hearing loss in children, it is recommended to consider an approach involving exploratory tympanotomy at an opportune time. 59 Subsequent decisions regarding artificial ossicular reconstruction or artificial auditory implants should be informed by the findings of the exploratory procedure, representing an optimal approach to diagnose and treat children with UCHL, particularly in cases involving cholesteatoma. Some perspectives suggest that suspected cases of COA and OTS should initially incorporate hearing aids to improve auditory function. 60 For bilateral cases, surgery may be considered at 5 to 6 years old, while unilateral cases might be deferred until 10 years old or later. However, an opposing viewpoint argues for early intervention in unilateral hearing loss, emphasizing that the temporal bone completes ossification around age 6, allowing for middle ear surgery. 61 Debates arise regarding inner ear window procedures in children, with some proposing waiting until the age of 15 to prevent window closure over time. 62 Nevertheless, Tolisano et al 63 asserts that children can safely undergo stapes surgery, noting a notably higher success rate in children compared to adults due to the shorter duration and less severe pathological changes in the footplate. Ching et al 64 indicates that children with CMEC undergoing surgery after the age of 3 do not exhibit a worse prognosis. For those under 1 year of age with no significant intratympanic growth, surgery can be delayed until 1 to 2 years of age. However, suspicion of CMEC in those over 3 years old should prompt early surgical intervention to minimize further damage to the middle ear caused by cholesteatoma. 30 Jenks et al 65 found that children in Potsic stage III were significantly older than those in stage I to II. Given that Potsic stage is a major risk factor for cholesteatoma recurrence and hearing loss, the early identification and intervention in children with CMEC are considered advantageous. Therefore, early diagnosis and intervention play a pivotal role in the management of UCHL in children. Our clinical experience suggests that surgical interventions in UCHL children aged 3 to 6 years do not result in significantly worse outcomes or increased complications.
The use of temporal bone HRCT is essential for the preoperative diagnosis of UCHL. 1 However, routine HRCT encounters challenges in accurately depicting the intricate structures of the middle ear, potentially leading to misdiagnosis and overlooking cases.4,6,17,22,24,26 Studies have highlighted variations in the effectiveness of HRCT in detecting middle ear diseases. Tang et al 9 reported an accuracy of only 40.0% in identifying congenital middle ear malformation (CMEM). Similarly, Zhang et al 22 found that only 62.1% of CMEM cases could be detected via HRCT, while Zhao et al 17 reported abnormal findings in the auditory bones in 9 out of 10 UCHL cases, including 5 cases with localized cholesteatoma. However, intraoperatively, all 10 patients were diagnosed with COA and CMEC, emphasizing that HRCT alone cannot conclusively determine the etiology of UCHL.
Various advanced imaging technologies, such as multislice computed tomography, cone beam computed tomography (CBCT), Multiplanar reconstruction (MPR), and Volume Rendering (VR), have been shown to enhance scanning precision and improve the quality of ossicular chain reconstruction, thereby increasing the success rate of preoperative diagnoses.19-21 Liu et al 19 demonstrated that MPR and Computed tomography volume rendering (CTVR) effectively display the ossicular chain, particularly excelling in showcasing the stapes superstructure and incus deformity. Li et al 20 proposed that HRCT post-processing techniques, such as MPR and CTVR, have the potential to reveal early, hidden minute cholesteatoma. Debeaupte et al 21 found that CBCT offers advantages over multidetector computed tomography with lower radiation exposure and higher resolution, significantly aiding in OTS diagnosis and staging. Therefore, the continued development of more refined scanning techniques and higher-quality imaging methods holds the potential to further enhance the success rates of preoperative diagnosis for UCHL.
Most congenital UCHL cases stem from genetic and embryonic developmental abnormalities. 30 Developmental impediments in the first or second branchial arch of the ectoderm may result in multiple coexisting pathologies.15,30 Furthermore, due to the nonspecific symptoms of UCHL, manifestations of one disease may mask another—a scenario not uncommon in clinical practice.5,6,12,37 For instance, CMEC could originate from residual epithelium associated with auditory bone development, potentially co-occurring with COA.6,17,32 Zhao et al 17 recommended a thorough examination for any soft tissue density shadows found in the tympanic cavity via HRCT to rule out minute cholesteatomas. In cases of stapes footplate fixation, SSCD may coexist and mask its symptoms. SSCD may also be present and mask its symptoms. Neglecting SSCD while addressing SFF alone can lead to poor postoperative hearing recovery. 12 Hence, for UCHL patients, thorough preoperative imaging examinations to identify more suspicious lesions and comprehensive intraoperative exploration of the middle ear structure are essential approaches to elucidate the etiology and enhance surgical benefits.8,20,24,31,32,46
To advance the diagnosis and treatment of patients with UCHL, otologists should prioritize several key aspects. First, it is imperative to expand the overall understanding of UCHL. This involves not only mastering common diseases such as COA, OST, and CMEC but also delving into rare diseases. Attention to detail during medical history collection, preoperative examinations, and surgical exploration is crucial.4,15,37,41,42,44,46,47,51,55 Second, there is a necessity to improve the ability to interpret imaging studies with precision. Thoroughly examining various parts, including the middle ear cavity, ossicular chain, stapes footplate, oval and round windows, and semicircular canals, is essential. Checking for the integrity of middle ear structures, the presence of abnormal tissue shadows, and density differences in structures like the stapes footplate, promontory, and semicircular canals is crucial.6,20,21,24,44,46,55 This aids in the preoperative identification of potential causes, facilitates surgery preparation, and improves communication with patients. In addition, it supports the study of surgical plans in advance and enables thorough exploration and reconstruction during surgery. Third, meticulous intraoperative exploration of the middle ear is vital, involving the complete removal of any abnormal lesions within the middle ear. For eligible cases, artificial ossicular implantation should be performed based on the type of lesion.3,10,16,23,45,47,56 For those not suitable for artificial ossicular implantation, the consideration of delayed implantation of bone conduction hearing aids is recommended to enhance the patient’s hearing level. 57 Fourth, post-surgery, a tissue pathology examination of suspicious neoplasms obtained should be conducted. Different postoperative intervention and recovery plans should be developed for different patients.31,48,51,53 Finally, there is a pressing need to bolster patient follow-up procedures by implementing regular reviews and closely monitoring tumor residue and recurrence. Especially for tumors with recurrent tendencies such as cholesteatoma and adenoma, the follow-up time should not be less than 5 years.31,47-49,51
The inherent limitations in this study are readily apparent. First, the heterogeneity of the research and the insufficient sample size impede a more comprehensive analysis of differences among various components and hinder the formulation of definitive conclusions. The diverse themes and methodologies employed in each study pose challenges in extracting and summarizing data. Consequently, the primary aim of our study is to further elucidate the definition of UCHL. We seek to engage in discussions with clinical professionals to refine diagnostic and treatment methods, ultimately enhancing the clinical benefits for patients. We assert that the etiology of UCHL is complex, and the existing preoperative examination methods are inadequate in definitively determining the patient’s condition. Exploratory tympanotomy surgery and comprehensive diagnosis remain central to the treatment paradigm.
Conclusions
In summary, UCHL represents a spectrum of diseases with analogous clinical manifestations. Preoperative diagnosis poses a formidable challenge, with exploratory tympanotomy emerging as the primary method for both diagnosis and treatment. Meticulous intraoperative exploration of middle ear tissues, lesion clearance, and ossicular chain reconstruction contribute significantly to favorable prognoses. Surgical intervention, even in children aged 3 to 6, is a viable option. Otologists should augment their overall comprehension of UCHL diseases, emphasizing the significance of preoperative imaging examinations and surgical exploration to optimize patient outcomes.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
Conceptualization, H.X.; software, Y.H. and H.S.; resources, H.X.; data extraction, Y.H. and X.Y.; data curation, Y.H., X.Y., Y.W., D.H., and S.Z.; writing—original draft preparation, Y.H., D.H., and X.Y.; writing—review and editing, Y.H., H.S., D.H., and S.Z.; project administration, H.X., X.Y., S.Z., and H.S. All authors have read and agreed to the published.
Data Availability Statement
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Natural Science Foundation of China (Grant numbers 82071057 and 82101229).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (approval number: UHCT21836; approval date: February 28, 2022).
Informed Consent Statement
Patient consent was waived because this study is a retrospective analysis of the treatment effects on patients and poses no foreseeable harm to them.