
Abstract
Keywords
Introduction
In recent years, the use of rigid bronchoscopy to establish an operative channel and the combination of flexible and rigid bronchoscopy for intracavitary procedures have become increasingly common. Airway management during bronchoscopy procedures presents a significant challenge for anesthesiologists. 1
Superimposed high-frequency jet ventilation (SHFJV) is a novel ventilation mode. It has been established that compared to traditional anesthesia machines and conventional jet ventilation, SHFJV can integrate the techniques of large tidal volume-controlled ventilation and high-frequency jet ventilation, thereby effectively addressing the problem of insufficient effective ventilation caused by the gas leakage during the procedure, as well as the issue of CO2 elimination associated with conventional jet ventilation.2,3 The repeated jet stream at the stenosis site may produce shear and stress, and lead to tissue edema, making the stenosis worse. Although severe airway stenosis is not considered as an absolute contraindication for jet ventilation in adults, it does significantly increase the various risks during the surgery. Moreover, for individuals diagnosed with indications for intracavitary treatment but with underlying severe pulmonary and cardiovascular diseases, high-frequency ventilation is a relative or absolute contraindication.
Currently, there are no relevant clinical reports related to the safe use of SHFJV in rigid bronchoscopy procedures for the high-risk patient population. Therefore, this study aimed to retrospectively investigate the safety and efficacy of SHFJV in the context of rigid bronchoscopy procedures.
Subjects and Methods
Subjects
A total of 363 patients underwent rigid bronchoscopy in the Zhongda Hospital with Southeast University from March 2021 to June 2023 were included in this study. Among them, there were 176 cases of airway stenosis and 187 cases were without airway stenosis. The inclusion criteria used were as follows: (1) aged 18 and above; (2) required ventilation support during endobronchial treatment; (3) voluntarily participated in the study. The exclusion criteria were as follows: (1) hemodynamic instability; (2) patients suffering from malignant or life-threatening arrhythmias or recent acute myocardial infarction; (3) patients with cerebral infarction or intracerebral hemorrhage within the past month; (4) insertion failure of the rigid bronchoscopy due to various reasons.
This study was approved by Clinical Ethics Committee of the Zhongda Hospital with Southeast University (approval number: 2021ZDSYLL364-P01).
Methods
All patients were subjected to invasive blood pressure monitoring, electrocardiography, pulse oximetry, and intraoperative blood gas analysis after entering the operation theater. Anesthetic induction was performed with midazolam; propofol; sufentanil; and rocuronium bromide administered intravenously. Anesthesia was maintained with a continuous intravenous infusion of propofol (4-6 mg/kg/hour) and remifentanil (0.15-0.25 µg/kg/minute). After anesthetic induction, a rigid bronchoscope (Storz and Carl Reiner) was placed by an experienced interventional bronchoscopist. The device and its working interface are shown in Figure 1. The closeup manner of how the bronchoscope is connected is shown in Figure 2.
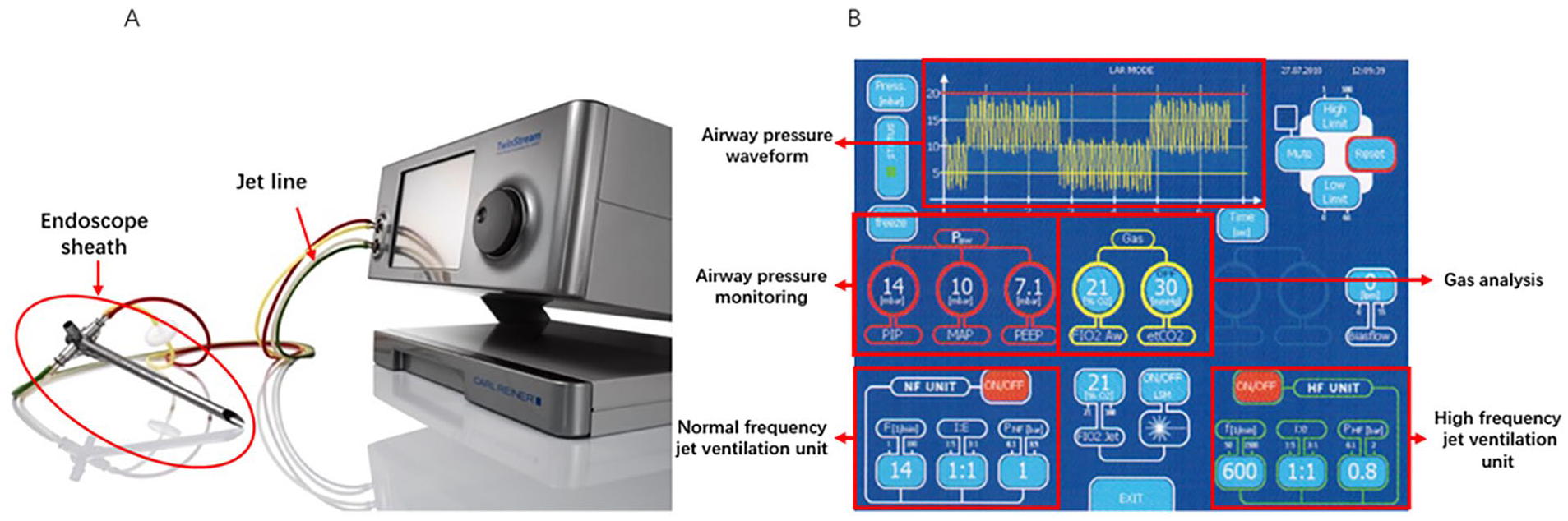
(A) The superimposed high-frequency jet ventilation device and (B) its working interface.

(A, B) The closeup manner of how the bronchoscope is connected.
The ventilation parameters were set as follows: frequency 600 per minute, inspiratory:expiratory (I:E) ratio 1:1 to 1:2, driving pressure 0.5 bar; conventional frequency jet ventilation with a frequency of 12 to 20 per minute, I:E ratio 1:1 to 1:2, and the driving pressure 0.7 bar. Intraoperatively, routine monitoring of the bispectral index was routinely performed to control anesthesia depth between 40 and 60. When the procedure was completed, the rigid bronchoscope was withdrawn, and an endotracheal tube or laryngeal mask was inserted and then connected to an anesthesia machine. The patients were sent to the recovery room for resuscitation after operation. When the patient recovered spontaneous breathing, the endotracheal tube/laryngeal mask was withdrawn. Patients with the Steward score above 6 points were sent back to the general ward, whereas those with the unforeseen complications or those who could not be extubated were admitted in intensive care unit (ICU).
Observation indicators
Mean arterial pressure (MAP), heart rate (HR), and pulse oxygen saturation (SPO2) were recorded at different time points as indicated: before induction of anesthesia (T1), after anesthesia induction (T2), 15 minutes after SHFJV ventilation (T3), and at the end of surgery (T4). Arterial blood gases was recorded at T1, T4, and 2 days after operation. We properly documented the duration of the surgery, time of endotracheal tube/laryngeal removal, length of stay in postanesthesia care unit (PACU), length of the postoperative hospitalization, incidence of various intraoperative and postoperative complications (including hypoxia, CO2 retention, bronchospasm, laryngeal edema, pneumothorax, postoperative respiratory distress, acute lung injury, etc), as well as the 30 day postoperative mortality rate.
Statistical analysis
SPSS version26.0 (SPSS Inc) was used for the statistical analysis and measurement data have been expressed as mean ± standard deviation (X ± SD), and whereas as the counting data have been expressed by frequency (n) or rate (%). Chi-square test was used for the count data, t test for the measurement data, paired t test for the paired groups measurement date, One-way analysis of variance (ANOVA) was used for comparison between the 2 groups. Statistical significance was set at P < .05
Results
Clinical Characteristics of Enrolled Patients
The baseline clinical characteristics of included patients have been shown in Table 1. There were no significant differences observed in age, gender, body mass index between the 2 groups (Table 1).
Basic Information of Patients Included in the 2 Different Groups.
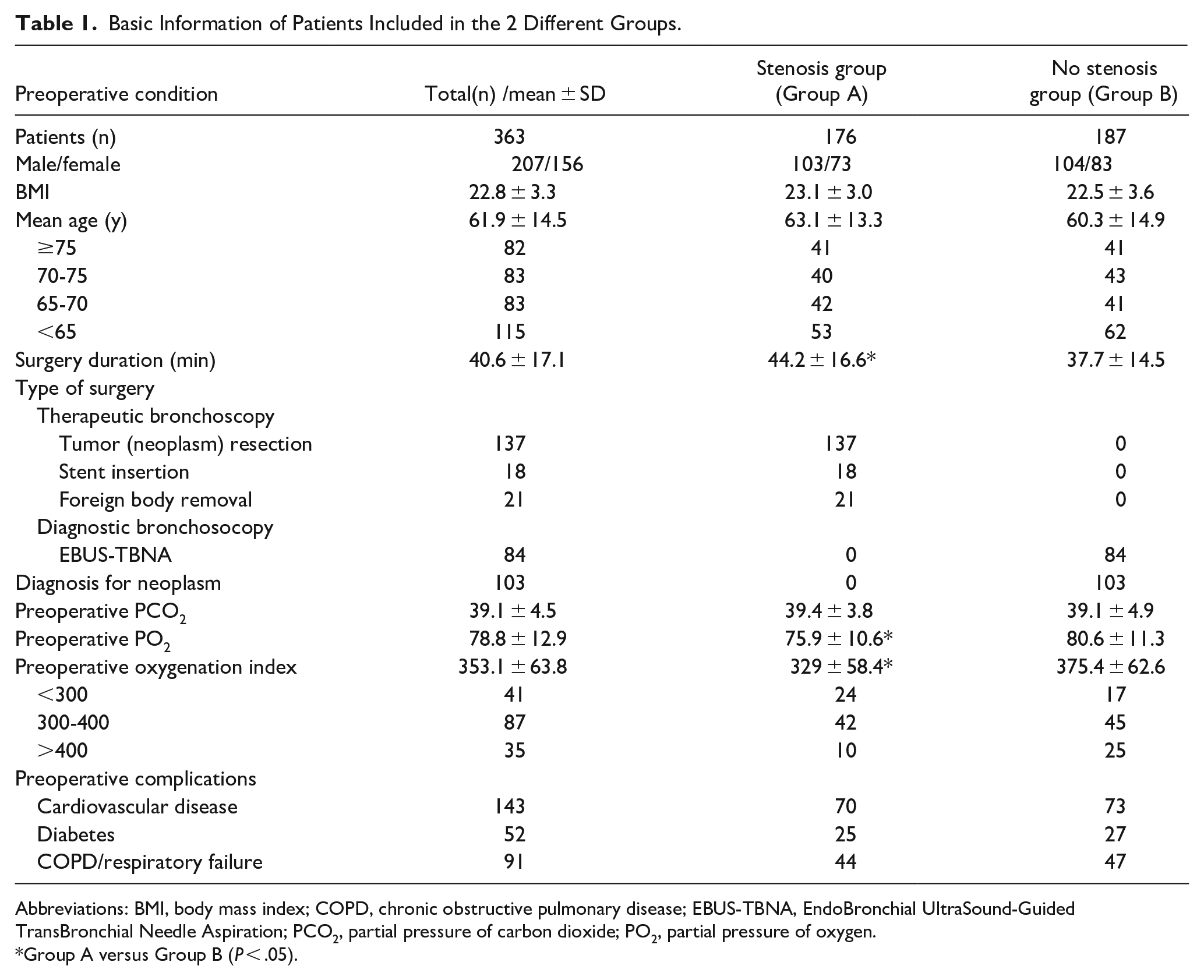
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; EBUS-TBNA, EndoBronchial UltraSound-Guided TransBronchial Needle Aspiration; PCO2, partial pressure of carbon dioxide; PO2, partial pressure of oxygen.
Group A versus Group B (P < .05).
The average duration of the surgery was higher in Group A than in Group B (44.2 ± 16.6 minutes vs 37.7 ± 14.5 minutes, P = .006; Table 1). The preoperative arterial partial pressure of oxygen (PO2) and the preoperative oxygenation index was significantly lower in Group A than in Group B (75.9 ± 10.6 mmHg vs 80.6 ± 11.3 mmHg, P = .003; Table 1). Due to varying degrees of airway obstruction, some patients in Group A experienced chest tightness, shortness of breath, and varying degrees of difficulty breathing before surgery, resulting in lower preoperative oxygenation compared to Group B. In addition, in terms of the treatment approaches, most patients in Group A were subjected to intracavitary treatments, but those in Group B predominantly received diagnostic bronchoscopy (Table 1).
Intraoperative Monitoring Indicators
During the surgical procedure, both groups of the patients maintained stable vital signs. It was noted that compared to T1, the MAP at time points T2, T3, and T4 showed a significant decrease (P = .001; Figures 3 and 4). Differences in MAP at different time points are considered to be caused by narcotic drugs. Although there were fluctuations in HR and SPO2 (Figures 3 and 4), they more or less remained within the normal range as well as MAP.
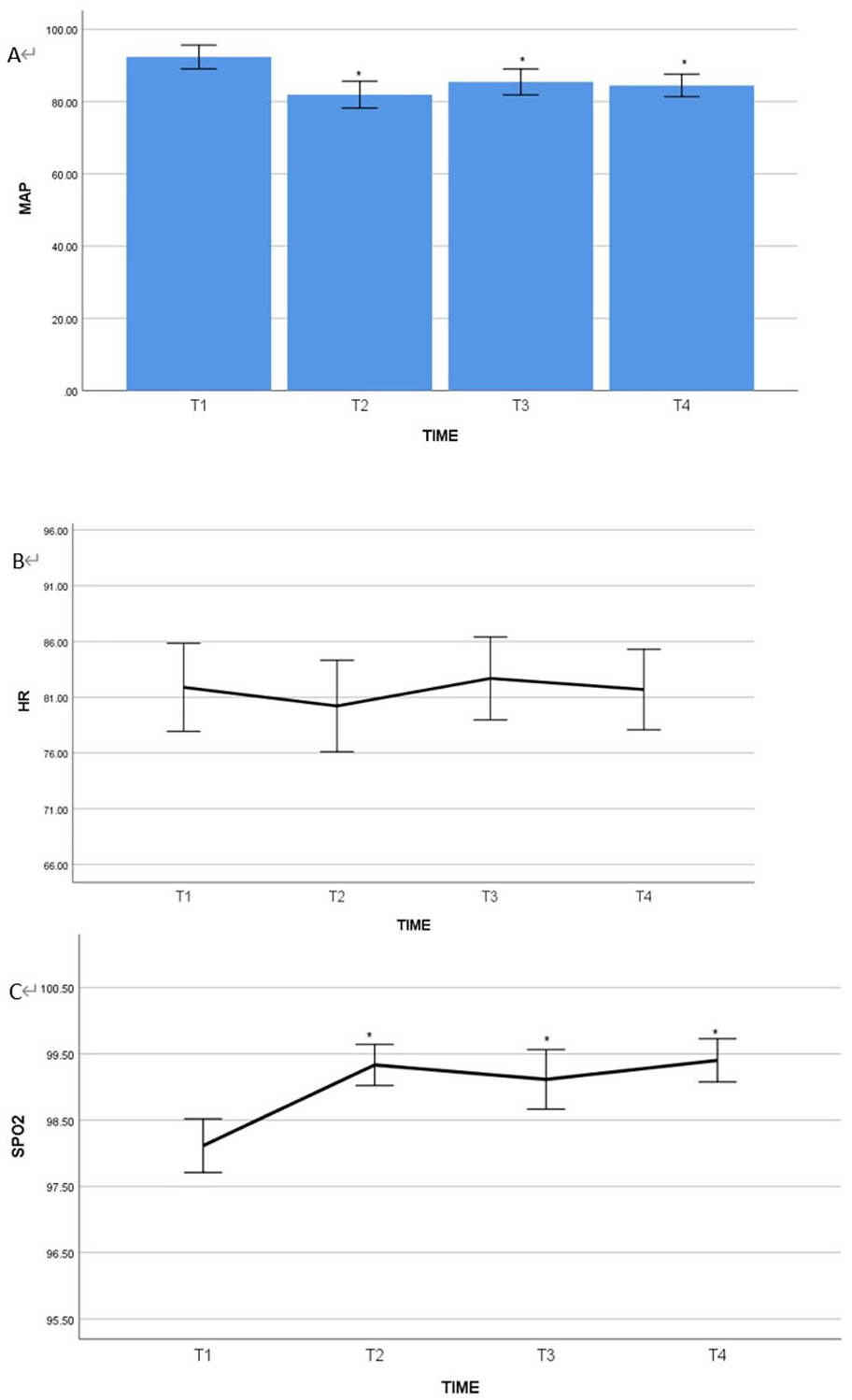
Comparison of MAP, HR, and SPO2 at different time points in the nonstenosis group (Group B) patients. It was found that in Group B, the MAP at T2 (after anesthesia induction), T3 (15 minutes of SFHJV ventilation), and T4 (end of surgery) were significantly lower than the MAP at T1 (on admission) (P < .05, panel A). There was no statistically significant difference in HR among the 4 time points (P > .05, panel B). The SPO2 at T2, T3, and T4 were significantly higher in comparison to SPO2 at T1 (P < .05, panel C).
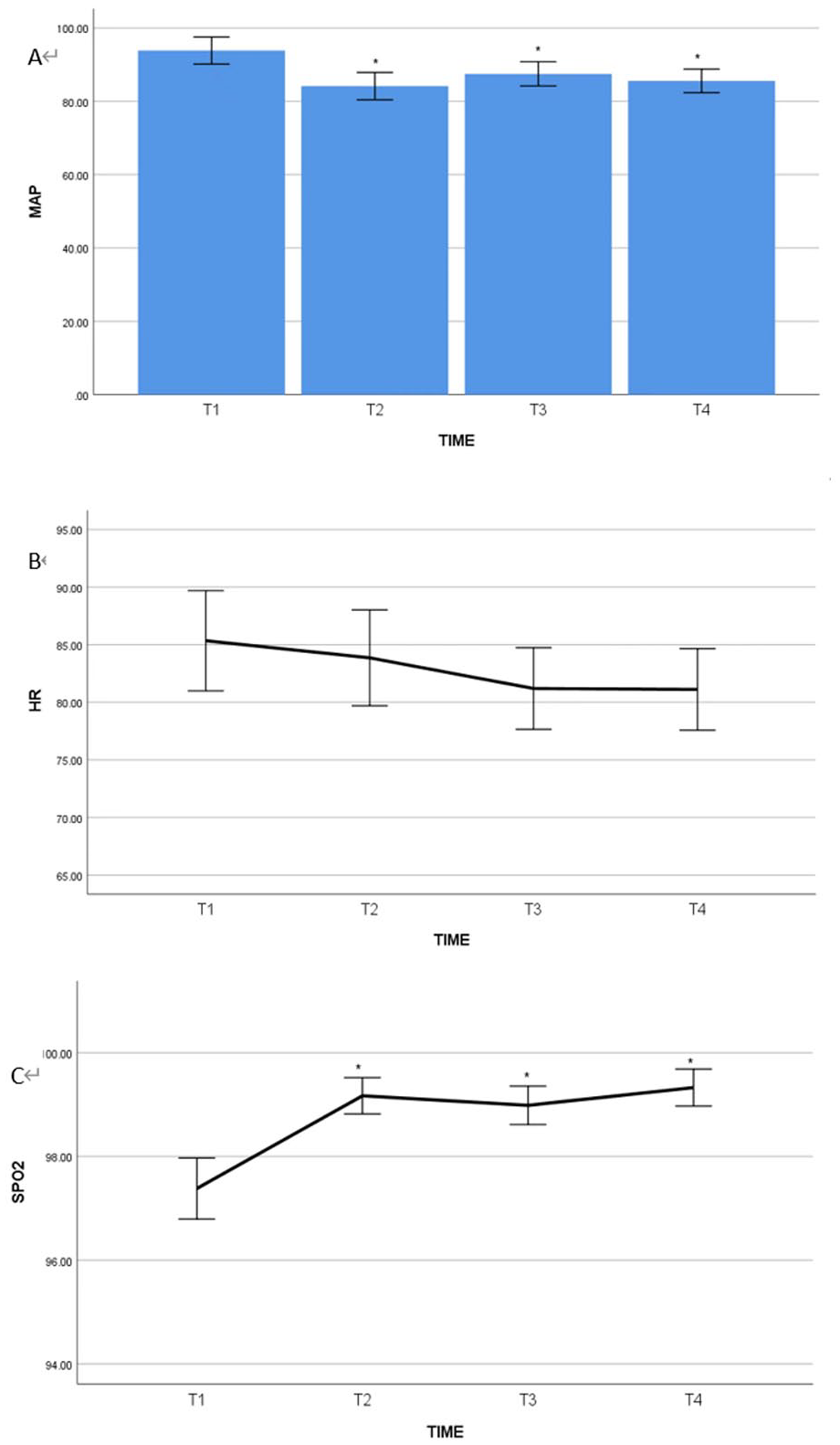
Comparison of MAP, HR, and SPO2 at different time points in the stenosis group (Group A) patients. It was noted that in Group A, MAP at T2 (after anesthesia induction), T3 (15 minutes after SFHJV ventilation), and T4 (at the end of surgery) were significantly lower than MAP at T1 (on admission) (P < .05, panel A). There were no statistically significant differences found in HR among the 4 time points (P > .05, panel B). SPO2 at T2, T3, and T4 showed significant improvement to T1 (on admission) (P < .05, panel C).
Complications and Postoperative Situations
We found that Group A showed a significantly higher increase in the rate of PCO2 at the end of the surgery in comparison to Group B (30.9% ± 15.8% vs 17.23% ± 10.4%, P = .002; Table 2). However, there were no significant differences observed between the 2 groups in terms of extubation time, PACU stay time, and postoperative hospitalization days. The oxygenation index improved substantially in both the groups on the second day after the surgery (Table 2). Although there was a significant improvement in oxygenation after surgery, it was still lower in group A than that in Group B (332.8 ± 121.9 vs 405.3 ± 129.9, P = .04; Table 2). It is considered to be related to the patient’s basic lung function status. During the operation, 1 patient in each group experienced bronchospasm (Table 2), which was relieved following administration of methylprednisolone. These 2 patients only exhibited a slight decrease in SPO2, with the lowest value being 89% to 91%. After the spasm was relieved, SPO2 recovered to 100%. In addition, 7 patients in Group A and 4 patients in Group B developed laryngeal edema (Table 2), which was relieved after the administration of methylprednisolone. There was no significant decrease in SPO2 noted in these 11 patients. Three patients were transferred to the ICU after the surgery (Table 2). One patient had multiple preoperative complications and a more severe condition, whereas the other 2 patients had slight bleeding during the operation, thus requiring delayed extubation. All the 3 patients were transferred to general wards on the second day after surgery. However, no deaths occurred in either group during the 30 day follow-up period (Table 2).
Postoperative Complications and Anesthesia Recovery in the 2 Different Groups.
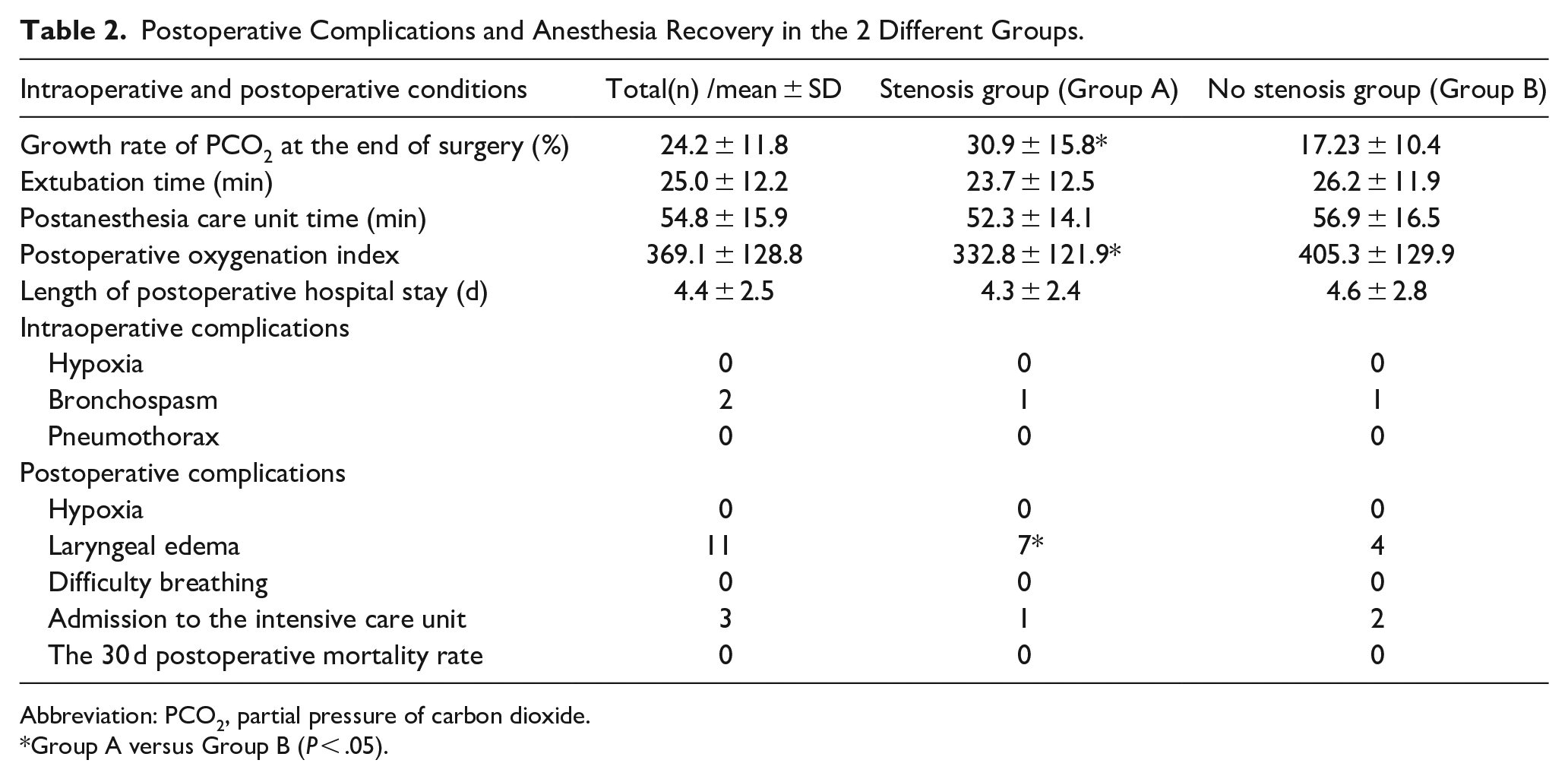
Abbreviation: PCO2, partial pressure of carbon dioxide.
Group A versus Group B (P < .05).
Intragroup Comparisons in Group A
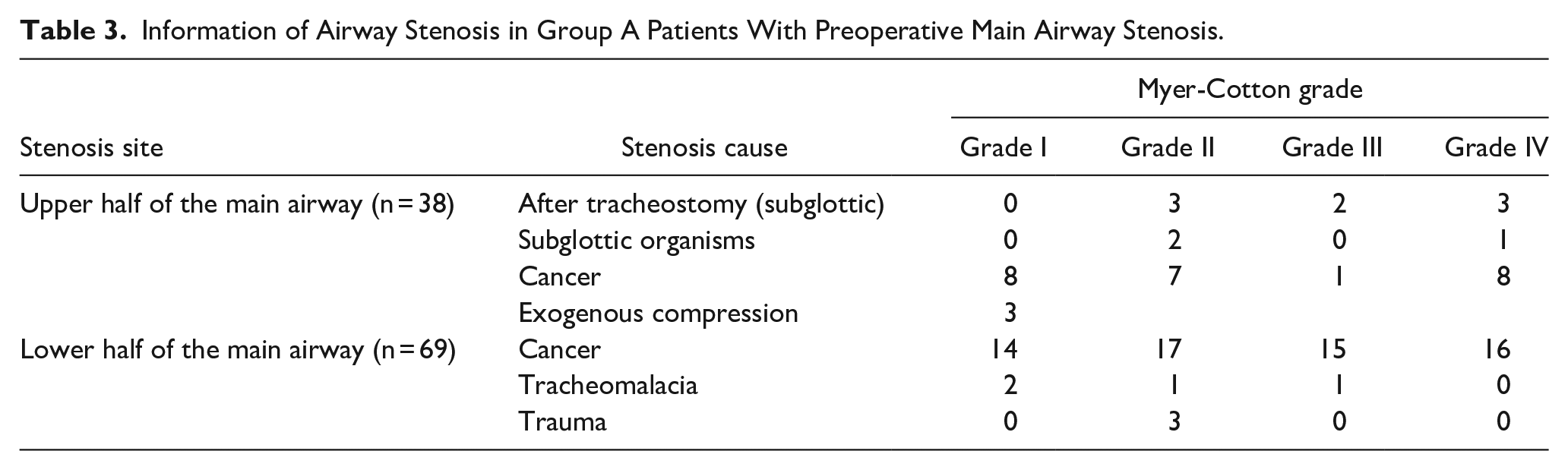
We also found that in Group A, there were 38 cases of narrowing located in the upper and middle parts of the main airway (11 of the patients had stenosis after tracheostomy, with the stenosis located below the glottis; Table 3), 69 cases in the middle and lower parts of the main airway, and 69 cases of left/right main bronchial stenosis. 107 patients with main airway stenosis were mostly caused by malignant tumors, accounting for 80% of the causes. In addition, there were also causes such as posttraumatic stenosis, granulation hyperplasia after tracheotomy, tracheomalacia, and exogenous compression (Table 3). According to the Myer-Cotton grading system, the degree of airway stenosis is divided into I to IV levels (Table 3). Thus, based on the severity of preoperative airway narrowing, the 107 patients with preoperative main airway stenosis were divided into 2 distinct groups: mild to moderate narrowing (Cotton I-II, tracheal stenosis <70%, n = 60) and severe narrowing (Cotton I-II, tracheal stenosis >70%, n = 47). The results indicated that patients with severe narrowing exhibited a longer operation time compared to patients with mild to moderate narrowing (47.8 ± 14.3 minutes vs 40.3 ± 15.2 minutes, P = .003; Table 4). However, there were no significant differences observed between the 2 groups in terms of extubation time (24.1 ± 10.5 minutes vs 25.6 ± 11.6 minutes, P = .23), length of PACU stay (32.7 ± 17.2 minutes vs 33.9 ± 18 minutes, P = .168), and the rate of CO2 increase (32.7% ± 17.2% vs 33.9% ± 18%, P = .339; Table 4). Although patients with severe narrowing had a longer length of postoperative hospitalization (Table 4), both the groups of patients displayed a good prognosis with no serious complications. In the mild to moderate narrowing group, 1 case experienced bronchospasm, which improved significantly after intravenous administration of methylprednisolone. In addition, 2 cases in this group developed laryngeal edema after the surgery (Table 4), but they were relieved after the treatment and there were no other severe complications such as respiratory distress or re-intubation noted in this group.
Information of Airway Stenosis in Group A Patients With Preoperative Main Airway Stenosis.
Comparison of Patients With Mild-to-Moderate and Severe Stenosis in Group A.
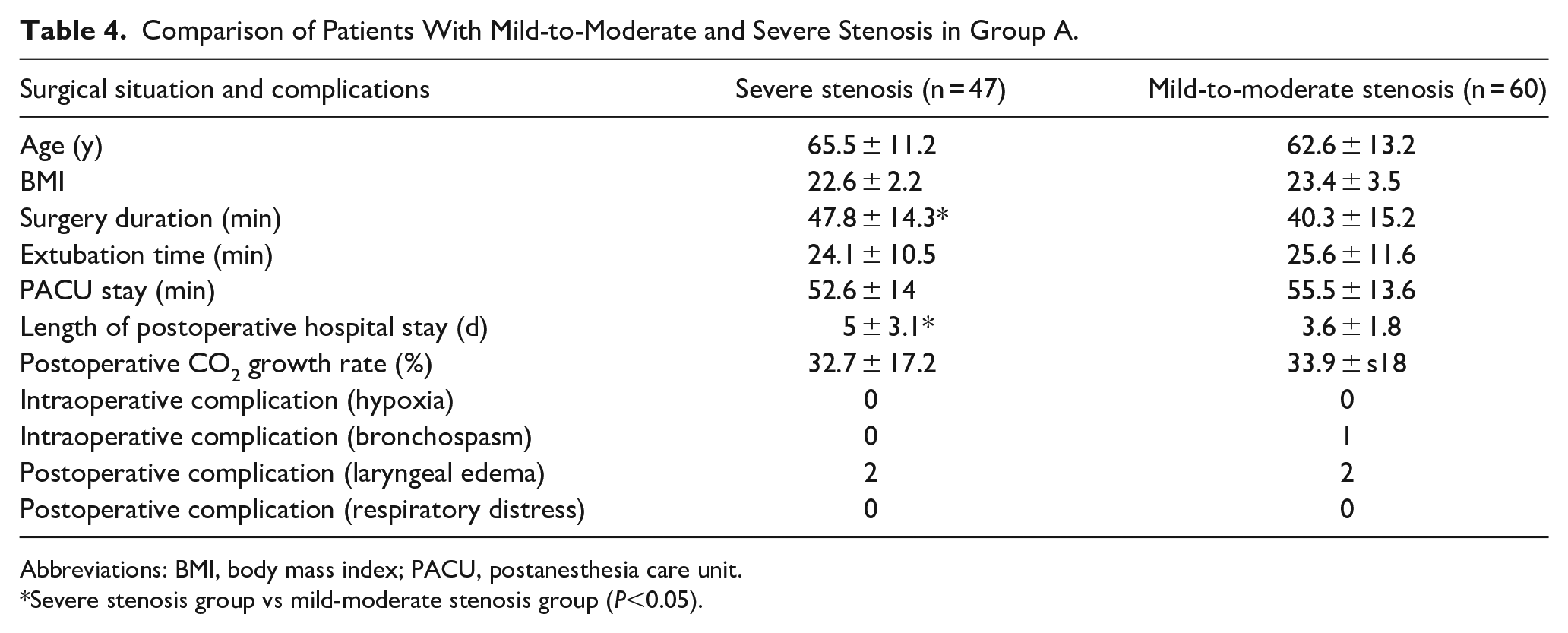
Abbreviations: BMI, body mass index; PACU, postanesthesia care unit.
Severe stenosis group vs mild-moderate stenosis group (P<0.05).
Discussion
In the past few years, the application of rigid bronchoscopy in intraluminal treatment has gained widespread acceptance and used commonly in clinical practice.4,5 Rigid bronchoscopy can display unique advantages in the management of airway diseases, including a large operating space, strong ability to maintain airway patency, effective handling of the massive hemoptysis within the airway, shorter procedure time, larger specimen acquisition, and easier placement and removal of various types of airway stents. It has been found to be useful particularly in those cases where the airway condition is poor and there is a risk of asphyxiation and respiratory distress.
In terms of ventilation management, during rigid bronchoscopy procedures, traditional ventilation modes often fail to provide safe and effective ventilation when the patient’s airway is completely open.
The SHFJV mode was first proposed by Aloy et al 6 in 1991. It was found that compared to high-frequency jet ventilation, it can effectively combine the function of conventional frequency ventilation while delivering high-pressure jet ventilation with tidal volumes of 1 to 3 ml/kg. This mode can utilize high-frequency jet ventilation to generate an expiratory pressure plateau in the lungs, thus creating a pulsatile positive end-expiratory pressure (PEEP) that can significantly benefit patient oxygenation. Frequency jet ventilation generates an inspiratory pressure plateau, which can facilitate rapid elimination of CO2 with larger tidal volumes. The combination of both these modes forms a pulsatile inspiratory pressure plateau as well as PEEP, which could be more effective in promoting CO2 elimination in comparison to high-frequency jet ventilation alone, and it can also effectively prevent atelectasis. 7 During the rigid bronchoscopy procedures, effective ventilation can be achieved by connecting the circuit to the side port of the bronchoscope, thereby resolving the contradiction between the rigid bronchoscopy treatment and airway management. As a novel ventilation technique, it was initially applied in adults and pediatric laryngeal surgery.8,9 In recent years, application range of this technique has been remarkably expanded and it has been widely used in several departments such as respiratory medicine, ICU, otolaryngology, as well as emergency medicine overseas.6,10
In this study, during the induction of anesthesia and the ventilation process, the blood pressure of patients showed a slight decrease (possibly related to the effects of narcotic drugs), but remained within the normal levels. Throughout the entire surgical procedure, blood pressure and cardiovascular function remained relatively stable without any significant fluctuations. Although there were some variations noted in the values of SPO2 at different time points, they were maintained at relatively higher levels. There were no instances noted where the operation had to be interrupted to improve patient oxygenation or due to the inability to maintain the optimal oxygen levels. In addition, various other indicators also remained within the normal physiological ranges. This can greatly enhance the convenience for the operators compared to the different conventional anesthesia machines and routine ventilation modes. In addition, the absence of manual control of ventilation and the technique of using high tidal volume ventilation with pure oxygen in the intraoperative period to improve patient oxygenation levels could significantly decrease the difficulty of airway management for the anesthesiologist.
A number of previous studies have indicated that SHFJV can be performed when the airway effectively loses its seal. It involves ventilation with smaller tidal volumes and higher ventilation rates, thus providing adequate ventilation while maintaining lower airway and intrathoracic pressures. This approach can minimize hemodynamic disturbances and help maintain cardiovascular stability. In addition, the incorporation of a conventional frequency ventilation mode in SHFJV can effectively prevent the accumulation of CO2. In the present study, the longest surgical duration was observed to be 70 minutes, and there were no instances of hypoxemia intraoperatively noted. Although postoperative PCO2 levels were slightly elevated compared to the preoperative levels, the overall patient prognosis was favorable, and no respiratory complications such as hypoxia, drowsiness, or respiratory distress observed. These findings suggest that optimal use of SHFJV in anesthesia management potentially ensure adequate oxygenation during surgery. Furthermore, all patients in this study maintained a safe circulatory level intraoperatively, and no other corresponding complications were observed during short-term and 30 day follow-up observations, which was consistent with the previous reports.11,12
Barotrauma is one of the major complications associated with high-frequency ventilation, as jet flow of high-frequency jet ventilation can cause the closure of small airways, thereby increasing pressure within the alveoli and distal trachea, thus raising the pressure within the airway. 13 However, SHFJV, by employing 2 different frequencies of jet streams simultaneously, can effectively reduce the occurrence of barotrauma. Although the exact airway pressures were not completely monitored in every patient enrolled in this study, no instances of barotrauma were observed in the short-term and 30 day postoperative follow-up, which was consistent with the previous research findings.14,15 These results demonstrated that SHFJV could be safely used for a broad range of clinical application. It has demonstrated promising prospects for patients affected with severe underlying lung diseases prone to barotrauma, such as chronic obstructive pulmonary disease (COPD), asthma, pulmonary fibrosis, and bullous lung disease.
There is currently no consensus on the degree of airway stenosis for which SHFJV could be used. For example, some researchers believe that an increase of 10% in the degree of luminal narrowing can significantly increase the risk of ventilation failure by 23%. 3 However, other scholars have suggested that SHFJV is more suitable for patients suffering from moderate airway stenosis. 16 However, there are no specific reports describing the safety of SHFJV when applied to patients with severe main airway stenosis. In our study, we observed patients with severe airway stenosis and found no severe complications during the surgery or postoperatively. Although the postoperative hospital stay was slightly longer in the severe stenosis group in comparison to the mild-moderate group (Table 4), all patients exhibited a good prognosis and no deaths were recorded within 30 days of follow-up. This finding indicated that SHFJV can be safely used in patients affected with severe and extremely severe airway stenosis. However, due to the relatively small sample size of patients included this study, further investigations with well-designed studies are needed to explore the potential safety of its application.
Regarding application of SHFJV in patients with underlying cardiopulmonary diseases, there is currently some controversy and no clinical consensus. Some researchers believe that patients with pulmonary diseases (such as COPD, pulmonary nodules, etc) possess a higher risk of failure with SHFJV and are more likely to switch to endotracheal intubation ventilation. 17 However, some other scholars hold a different view, and have suggested that due to the minimal circulatory impact of SHFJV, it can be more suitable for use in patients with pulmonary or coronary artery diseases. 12 Among the 363 patients included in this study, 198 patients had a history of severe cardiopulmonary diseases such as hypertension, coronary heart disease, heart failure, and COPD. Some patients also had both lung and heart diseases (Table 1). This group displayed stable circulation during the surgery, with no severe complications observed intraoperatively or postoperatively. Among the 198 patients, 2 experienced bronchospasms, which was relieved after administration of the systemic steroids (methylprednisolone). These 2 patients showed only a slight decrease in SPO2, with the lowest value reaching 89% to 91%. After relieving the airway spasm, the SPO2 recovered to 100%. One patient in the group had preexisting heart failure, COPD, and type I respiratory failure. Although oxygenation was well maintained during the surgery, the patient was still transferred to the ICU for the continued observation and treatment, and thereafter was transferred to general ward on the second day after the surgery. The data from current study demonstrated that SHFJV has excellent safety in patients with underlying heart and lung diseases. This finding can greatly expand the application of rigid bronchoscopy treatment techniques to a wider range of patients with underlying heart and lung comorbidities.
SHFJV is considered safe and effective in clinical practice. Although this view is widely accepted, there is no research based on reliable data to prove its safety. This may be the main reason why this ventilation method, despite its safe and effective use in clinical practice for many years, is still less commonly used in hospitals around the world. However, previous studies have mostly focused on observing intraoperative oxygenation, carbon dioxide, and postoperative complications. While observing the safety of SHFJV in rigid bronchoscopic endoluminal treatment, this study focuses on whether SFHJV is equally safe for special populations with varying degrees of airway stenosis and severe cardiopulmonary disease before surgery, and provide some clinical data references for controversial issues in clinical practice.
There are a few limitations associated with this study as well. First, it is a single-center, retrospective study and the sample selection might introduce bias. The results need further validation through well-designed prospective, randomized, controlled studies in the future. Second, the sample size for observation was relatively small, especially for the patients with airway stenosis. There were a limited number of patients included with severe and extremely severe conditions, and further differentiation between the benign and malignant airway narrowing was not performed. Third, real-time monitoring of the various parameters such as CO2 concentration and airway pressure within the airway was not conducted. The study primarily focused on the measurement of the traditional clinical indicators of anesthesia management. It is hoped that the future studies will incorporate these aspects for further investigation and provide better clinical relevance.
Conclusions
In summary, the application of SHFJV in airway management during the rigid bronchoscopy can facilitate optimal patient oxygenation, reduce intraoperative CO2 accumulation, and offer favorable surgical conditions for the operator. It can also effectively maintain oxygenation during the procedure for the patients with severe and extremely severe main airway stenosis, thus ensuring the continuity of the operation. SHFJV exhibited minimal impact on the patient’s intraoperative circulatory level and thus can be safely used in elderly and high-risk patients with underlying cardiac and pulmonary diseases. It can thus serve as a suitable management method for rigid bronchoscopy treatment, with significant clinical value and promising prospects for further promotion.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
Literature search: Jing Li; data collection: Jing Li, Shixia Xu; study design: Ming Ding, Jing Li; analysis of data: Rongna Yang; manuscript preparation: Jing Li; review of manuscript: Ming Ding.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case was obtained from Clinical Ethics Committee of the Zhongda Hospital with Southeast University (approval number: 2021ZDSYLL364-P01).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Clinical Ethics Committee of the Zhongda Hospital with Southeast University (approval number: 2021ZDSYLL364-P01) approved protocols.