
Abstract
Objective:
This study’s primary objective was to determine the predictive value and clinical significance of chest X-ray in diagnosing foreign body aspiration (FBA) in children. In addition, demographic, clinical, radiological, and bronchoscopic findings were evaluated.
Methods:
This retrospective study included 203 children (0-18 years of age) admitted to the hospital with suspected FBA during 2013 to 2023. Patients’ data were evaluated in terms of age, gender, symptoms, radiological findings, bronchoscopic findings, length of hospital stay, period of presence of foreign bodies (FBs), and post-procedural complications.
Results:
FBA was confirmed in 52.2% (n = 106) of the children, the majority (76.4%) of cases occurring in children aged 0 to 3 years. Symptoms most frequently reported presenting were cough (63.0%), wheezing (25.1%), vomiting (24.6%), choking (23.2%), fever (11.0%), stridor (9.4%), and cyanosis (6.4%). Chest radiographs revealed pathological findings in 62.1%, most commonly being prominent bronchovascular markings (50.4%), hyperinflation (15.2%), reduced transparency (15.2%), and visible radiopaque FBs (3.2%). Auscultation was abnormal in 65.0% of cases, with wheezing, diminished breath sounds, and crackles found most frequently. Although both auscultation and X-ray findings are independently associated with FB detection, auscultation demonstrates stronger predictive value. Bronchoscopy identified the right bronchial tree as the most frequent location of FBs (47.2%), with nuts being the item most commonly retrieved (51.9%).
Conclusions:
This study highlights the value of chest X-ray in combination with clinical signs. While auscultation alone is more predictive, using both improves diagnostic accuracy. A structured approach with clinical exam, imaging, and timely bronchoscopy is essential for optimal outcomes.
Keywords
Introduction
Foreign body aspiration (FBA) is a relatively common medical condition addressed in emergency care of children and can lead to severe complications or even sudden death. It most frequently occurs in children under 3 years of age, often during meals when the child is simultaneously playing, laughing, or crying. 1
Children in this developmental stage frequently explore their environment by placing objects into their mouths. The risk of aspiration increases when a child is simultaneously walking, running, talking, or laughing. Further predisposing children to aspiration events are the facts that their ability to chew and swallow is not yet fully developed, and their laryngeal elevation and glottic closure are still immature. 2
Commonly aspirated foreign bodies (FBs) include seeds, nuts, pieces of fruit or vegetables, and small plastic or metal toy components. 3 Clinical manifestations typically include coughing, wheezing, and respiratory distress, with severe cases presenting as acute choking. Some patients, however, may present with minimal or even no symptoms, and this can make diagnosis challenging.4,5
Prompt diagnosis is crucial, particularly in cases involving respiratory distress. The diagnostic approach includes a comprehensive physical examination with auscultation, together with an imaging method, such as a chest X-ray, which may reveal radiopaque FBs. In cases of radiolucent FBs, indirect findings such as unilateral hyperinflation (emphysema) or atelectasis may be observed. 1 A detailed clinical history from a witness is essential, especially when clinical symptoms are nonspecific. Bronchoscopy remains the gold standard for both definitive diagnosis and therapeutic removal of the FB. The primary aim of this study was to evaluate the importance and predictive value of chest X-ray in the differential diagnosis of FBA.
Materials and Methods
A retrospective study was conducted at the tertiary referral center. Included were pediatric patients ages 0 to 18 years who were admitted with suspected tracheobronchial FBA and underwent rigid or flexible bronchoscopy between January 2013 and December 2023. All patients received a standardized assessment, including detailed medical history, physical examination, chest radiography, and lung auscultation. Patients with incomplete medical records were excluded from the study. Data were extracted from patient files and analyzed for demographic characteristics, clinical presentation, radiologic findings, and bronchoscopy findings.
The surgical intervention was performed in the operating theater under general anesthesia. Rigid or flexible bronchoscopy was conducted using a Richard Wolf or Storz rigid bronchoscope and a Pentax flexible bronchoscope. FB extraction was carried out using various types of bronchoscopic forceps. Pediatric bronchoscopy is performed under deep sedation or general anesthesia, with continuous monitoring of vital signs. Ventilation is maintained through a side port in rigid bronchoscopy or via an endotracheal tube with an adapter in flexible bronchoscopy. High-frequency ventilation is an alternative for both types. Lidocaine spray is often used for local anesthesia, and sedation is typically achieved with propofol, sevoflurane, or both.
Standard descriptive statistics were employed in the analysis. Categorical variables were presented as absolute and relative frequencies. Continuous variables were reported as means with standard deviations or as medians, depending on their distributions. Nominal variables were compared using Pearson’s chi-square test. Continuous variables meeting parametric assumptions were analyzed using Student’s t-test. Categorical data are expressed as percentages. A P ≤ .05 was considered statistically significant. All analyses were conducted using Statistica, version 14, TIBCO Software.
Results
Demographic Characteristics
A total of 203 pediatric patients with suspected FBA were included in the study. Of these, 70.9% (n = 144) were male, and 29.1% (n = 59) were female. The median age was 1.9 years (range: 15 days-18 years; Figure 1). The majority of patients (76.4%, n = 155) were in the 0 to 3 years age group, followed by 18.2% (n = 37) in the 4 to 12 years group and 5.4% (n = 11) in the 13 to 18 years group. FBA was confirmed in 106 patients (52.2%), with a male predominance (66.0%, n = 76). The yearly distribution of confirmed cases remained stable over the 11 year period, without statistically significant variation (Figure 2). The highest monthly incidence was observed in September (14.2%, n = 15), although this finding did not reach statistical significance (Figure 3).
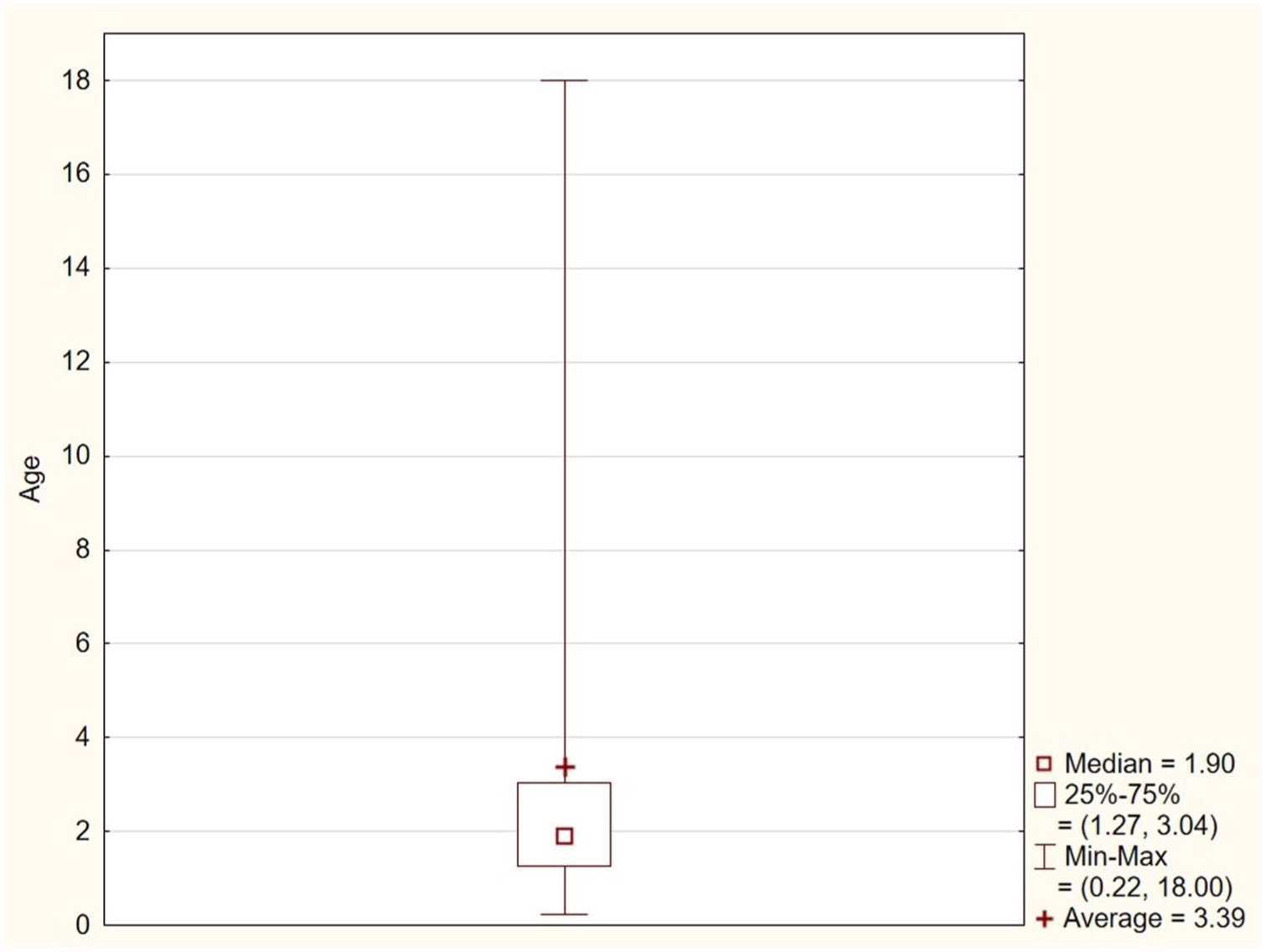
Age distribution in patients with suspected foreign body aspiration.
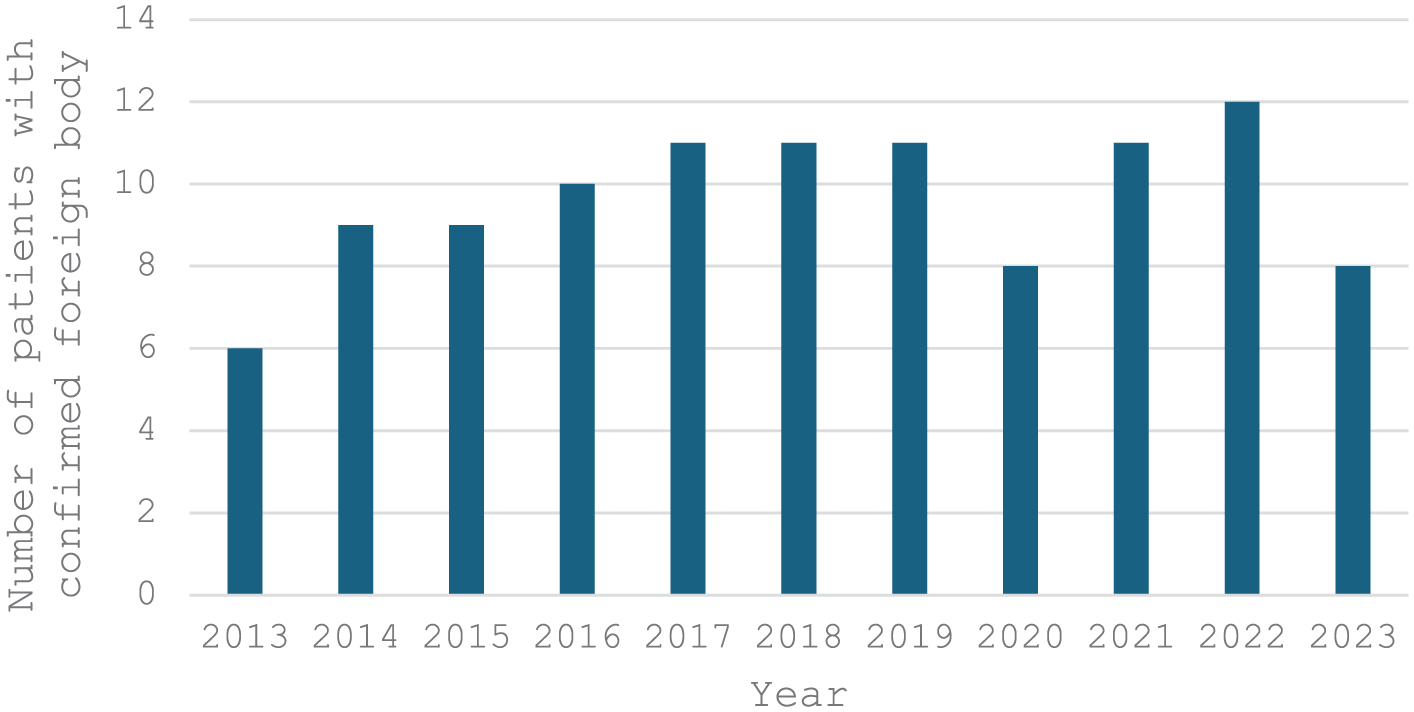
Foreign body detection over the years.
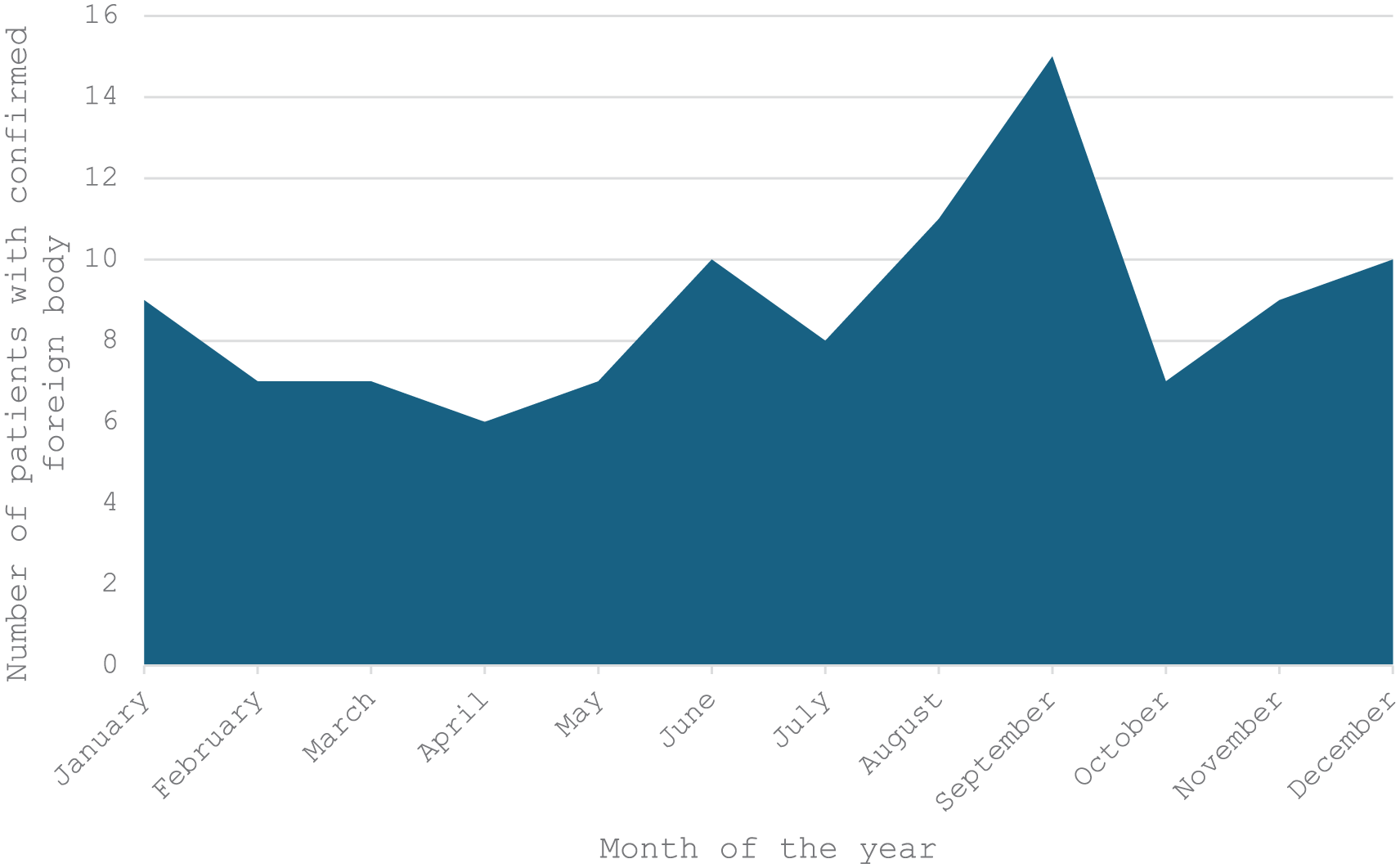
Positive foreign body detection during the year.
Clinical and Radiological Findings
The presenting symptoms most frequently reported were cough (63%, n = 128), wheezing (25.1%, n = 51), vomiting (24.6%, n = 50), choking (23.2%, n = 47), fever (11.0%, n = 22), stridor (9.4%, n = 19), and cyanosis (6.4%, n = 13; Figure 4).
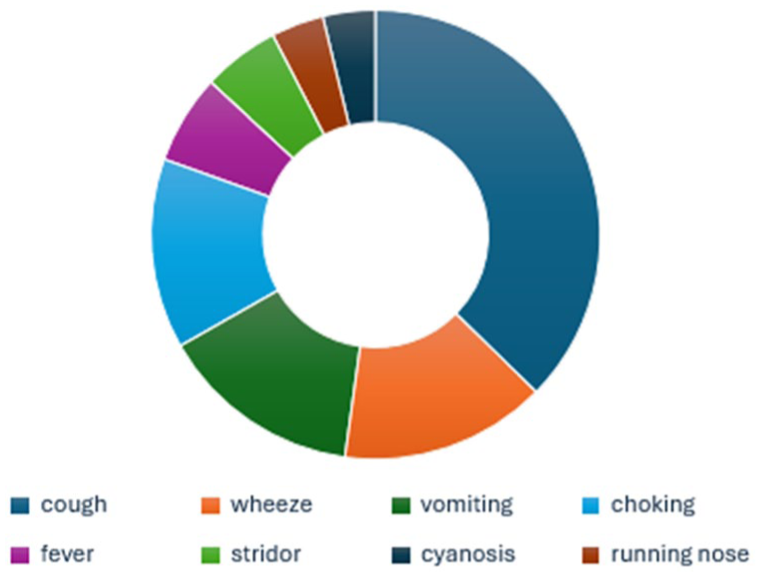
Clinical symptoms of suspected FBA. FBA, foreign body aspiration.
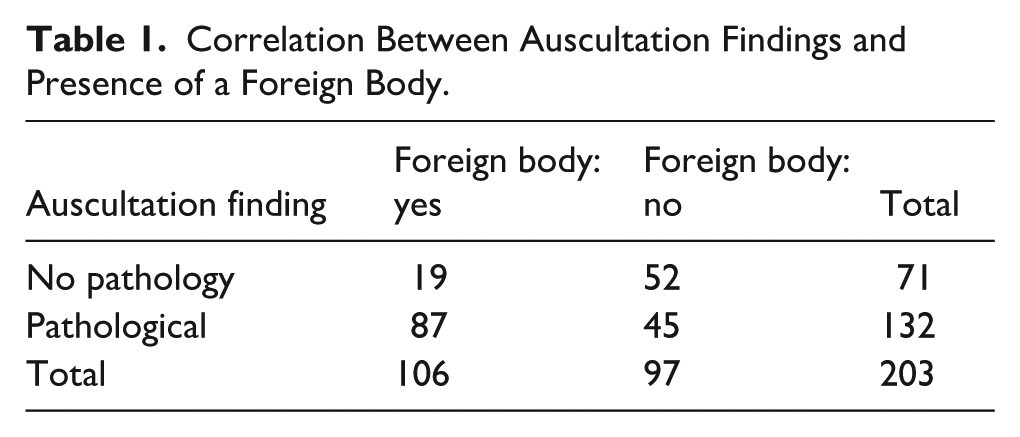
Auscultation was abnormal in 65.0% of cases (n = 132), with wheezing and rhonchi (26.1%, n = 53), diminished breath sounds (25.6%, n = 52), and crackles (14.3%, n = 29), the findings most commonly detected (Figure 5). There was a statistically significant association between abnormal auscultation and confirmed FBA (χ2 = 27.83, P < .00001; Table 1).
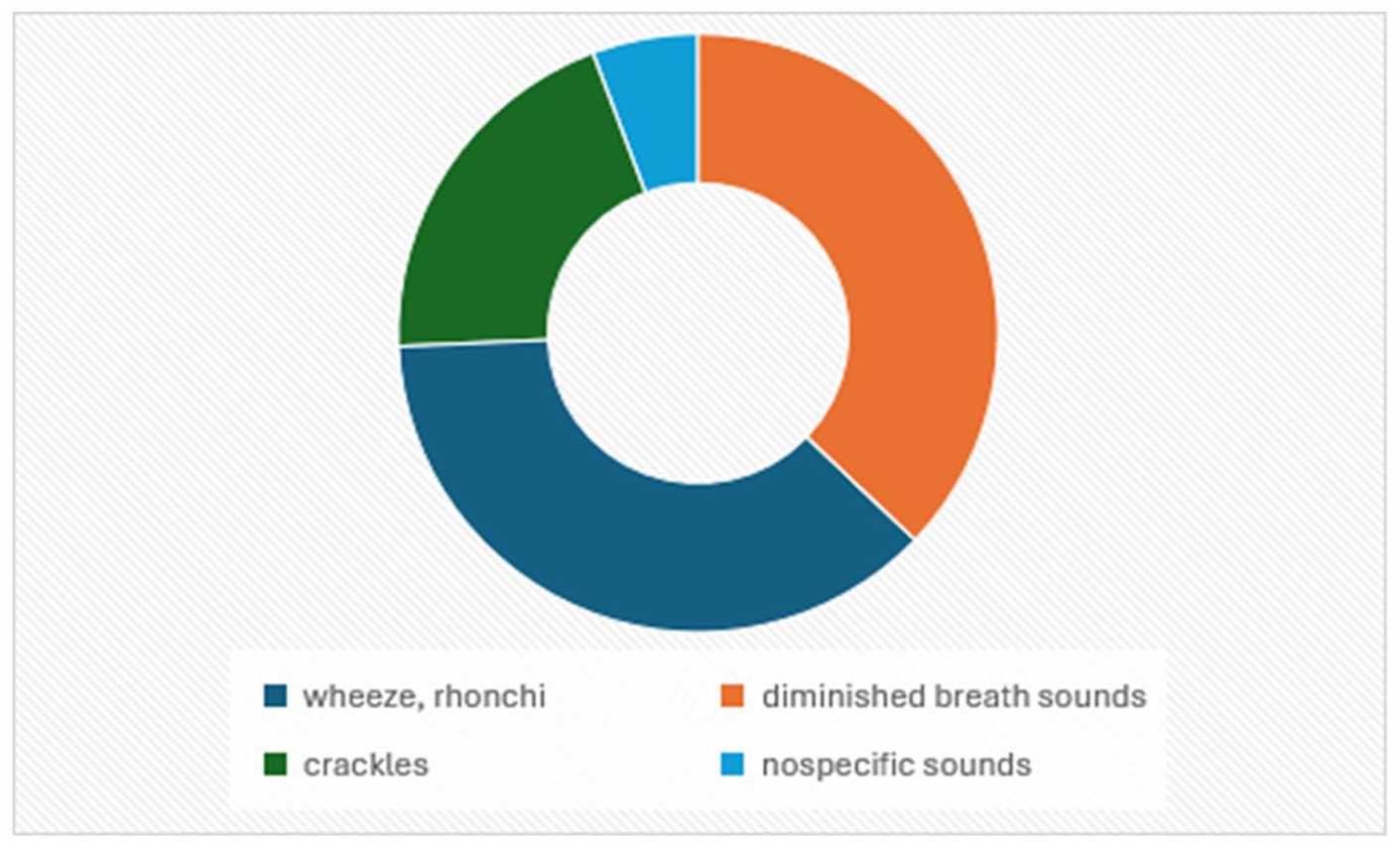
Auscultation findings in FBA. FBA, foreign body aspiration.
Correlation Between Auscultation Findings and Presence of a Foreign Body.
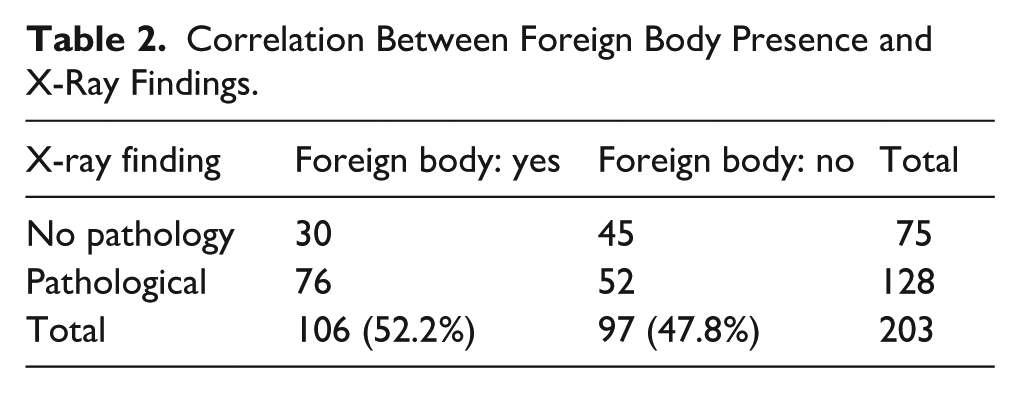
Pathological chest radiographs were present in 62.1% (n = 126), while 37.9% (n = 77) showed no abnormalities. The most frequent radiographic abnormalities included prominent bronchovascular markings (50.4%, n = 63), hyperinflation (15.2%, n = 19), reduced lung transparency (15.2%, n = 19), and visible radiopaque FBs (3.2%, n = 4). The diagnostic performance of chest X-ray for FB detection was evaluated by calculating the false positive and false negative rates, as well as positive predictive value (PPV) and negative predictive value (NPV). Out of 203 cases, 106 (52.2%) had confirmed FBs. Chest X-ray showed pathological findings in 128 cases, including 76 true positives and 52 false positives. Among 75 normal X-rays, 45 were true negatives and 30 false negatives. The PPV was 59% and the NPV 60%, indicating limited accuracy of chest X-ray in detecting FBs. A significant correlation was observed between pathological chest X-ray findings and confirmed FBA (χ2 = 6.79, P = .00473; Table 2).
Correlation Between Foreign Body Presence and X-Ray Findings.
The combined diagnostic performance of auscultation and chest radiography is presented in Table 3. Both auscultation and X-ray findings are independently associated with the detection of an FB. However, auscultation demonstrates a stronger predictive value, as reflected by a higher chi-squared statistic and lower P value.
Correlation Between Auscultation and X-Ray Findings and Foreign Body Aspiration.

Bronchoscopy Findings
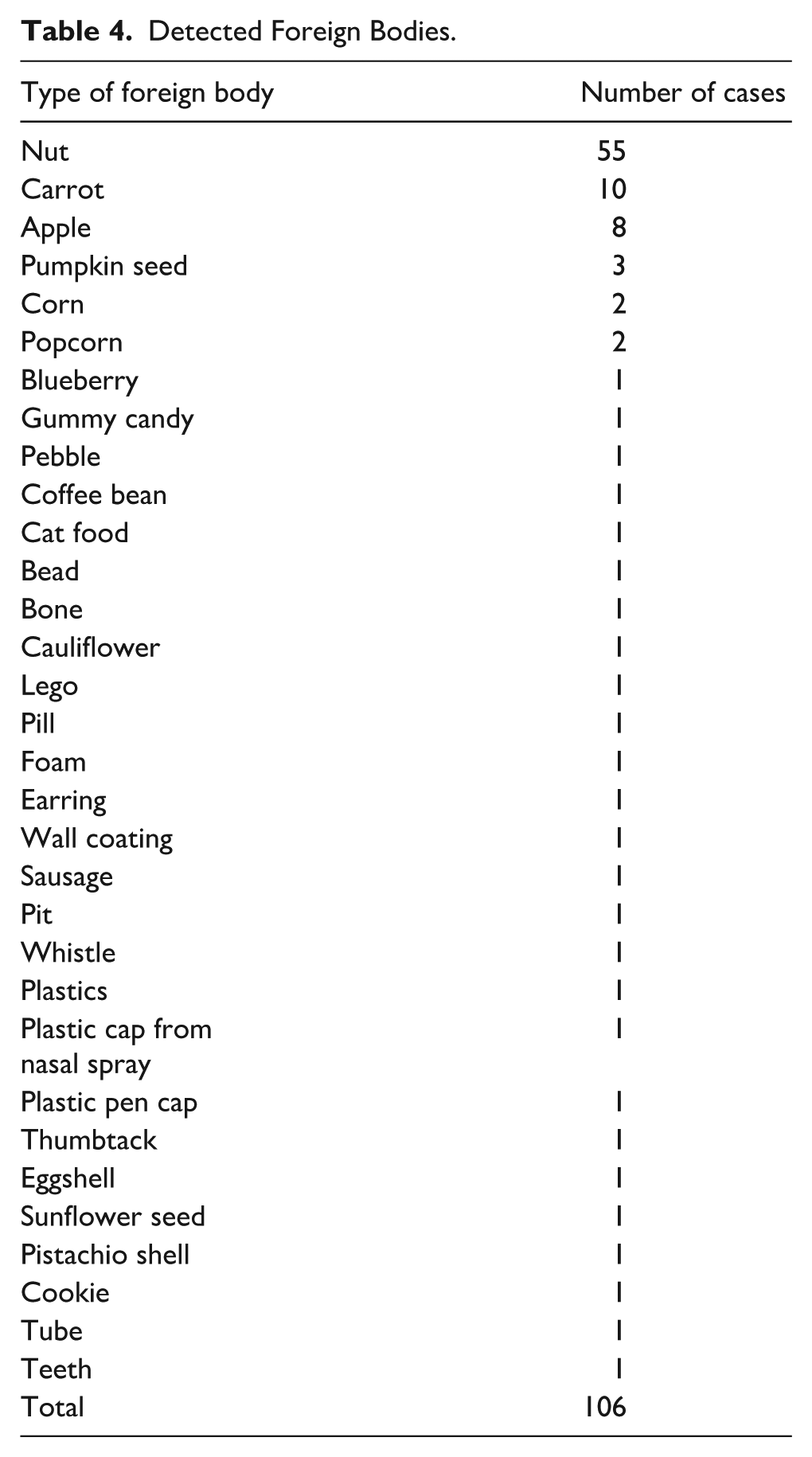
The most frequent location of FBs was the right bronchial tree (47.2%, n = 50), followed by the left bronchial tree (34.9%, n = 37), both bronchi (8.5%, n = 9), and the trachea (8.5%, n = 9). In 1 case (0.9%), the FB was located in the nasopharynx. Organic FBs accounted for 86.8% (n = 92) of cases, with inorganic materials comprising 13.2% (n = 14). The object most frequently identified was a nut (51.9%, n = 56), followed by carrot (9.4%, n = 10), apple (7.6%, n = 8), pumpkin seed (2.8%, n = 3), and popcorn (1.9%, n = 2). Additional FB types are listed in Table 4.
Detected Foreign Bodies.
Procedural and Hospitalization Data
A total of 203 bronchoscopic procedures were performed: 145 rigid bronchoscopies (71.4%), 40 flexible bronchoscopies (19.7%), and 18 combined procedures (8.9%). Control bronchoscopy was conducted in 81.1% (n = 86) of patients. Repeat controls were necessary in 10 patients, including 7 who underwent 2 procedures, 2 who underwent 3, and 1 who required 4. Most control procedures were indicated following nut aspiration, primarily to assess for residual airway obstruction or ongoing inflammation. The mean interval from symptom onset to bronchoscopy was 58.6 hours, with a median of 18.5 hours. The mean duration of hospitalization was 4.3 days overall and 4.7 days for patients admitted to the general pediatric ward and 3.2 days for those requiring care in the pediatric intensive care unit, depending on clinical severity and perioperative needs.
Discussion
FBA is a life-threatening condition encountered in pediatric emergency care and requires prompt recognition and urgent intervention. Children ages 1 to 3 years are at the highest risk due to developmental and anatomical factors.4,6,7 In our study 81.1% of patients with confirmed FBA were within this age group. Several studies have demonstrated a male predominance among FBA cases,3,7,8 which is also consistent with our findings.
The timing of FBA cases in our study showed a seasonal pattern, with the highest incidence in September, followed by August, June, and December. This differs from other studies, which often report peaks in November and December. 7 The increased cases in late summer and early autumn in our cohort may relate to school holidays and outdoor activities during these months, leading to greater exposure to potential FBs and less supervision. The December peak aligns with festive seasons, such as Christmas, when children are exposed to small food items and decorations. Recognizing these seasonal variations is important for tailoring preventive education and public health efforts to local contexts.
FBA typically presents with symptoms such as coughing, dyspnea, wheezing, a choking episode, or hoarseness.1,7 -10 However, Raviv et al found that a history of choking or coughing does not reliably predict FBA and that symptoms like fever or rhinorrhea do not rule it out. 11
Auscultation findings in FBA cases are variable and may include unilateral decreased breath sounds, wheezing, or localized rhonchi.1,9,12 These findings, while suggestive, are not pathognomonic and must be interpreted in conjunction with clinical history and imaging.
Chest radiography is a widely used initial diagnostic tool in suspected FBA, though it may be normal in up to 30% of cases.1,12 Typical signs include unilateral hyperinflation, mediastinal shift, or atelectasis. In our cohort, the most frequent radiographic finding was prominent bronchovascular markings, a nonspecific finding seen also in other respiratory conditions. Chest X-ray showed limited accuracy in detecting FBs, with a PPV of 59% and NPV of 60%. Among 203 cases, many false positives (52) and false negatives (30) were observed, indicating that radiographic findings alone are insufficient for diagnosis.
We observed a statistically significant correlation between positive FBA diagnosis and the combination of abnormal auscultation and pathological radiographic findings. The highest proportion of confirmed cases 59.4% was found when both modalities were abnormal, whereas only 4.7% were confirmed when both were normal. When considered independently, auscultation showed stronger predictive value than did chest radiography, supporting its importance in the clinical assessment of suspected FBA.
In our department, we do not use a formal scoring system to decide on bronchoscopy. The decision to proceed with bronchoscopy is based on a comprehensive clinical assessment, including patient history, clinical condition, auscultation findings, and chest X-ray results. All these factors are considered together to guide the indication for bronchoscopy.
The nature of aspirated FBs varies by region, influenced by local diet, cultural practices, and exposure to small objects. Organic materials, such as nuts, seeds, and food particles, are most commonly aspirated in many regions.5,13 Nonorganic objects, including plastic and metal components, are also frequently encountered, especially in older children. 14 Our findings align with these trends, with organic materials being the most frequently aspirated.
The right main bronchus is the most common site for FB lodgment due to its wider and more vertical anatomy. 6 In our study, the majority of FBs were located in the right bronchial tree, followed by the left bronchus and trachea. Nevertheless, some studies have reported left-sided predominance.15,16
Bronchoscopic removal of tracheobronchial FBs is a technically demanding procedure leading to potential complications, such as migration, bleeding, hypoxia, bradycardia, bronchospasm, tracheal laceration, and even death.7,12,17 Rigid bronchoscopy remains the gold standard for FB extraction, offering superior airway control and a wide range of retrieval instruments.18,19 Flexible bronchoscopy provides better access to distal airways and is considered by some authors to be a safe and effective alternative. 10 In certain cases, such as aspiration of metal pins or slippery objects, a combined approach is recommended. 20 A novel technique, recently described, using a 3 mm gold-plated neodymium magnet under fluoroscopic guidance, enabled safe retrieval of distal metallic FBs. 21
Safia et al performed a meta-analysis comparing flexible and rigid bronchoscopy in pediatric FBA and concluded that both methods are safe and effective. 22 However, significant heterogeneity among studies limits the ability to generalize these findings. Therefore, an individualized approach—based on patient characteristics, clinical context, and surgeon expertise—is advised. Our results support the primary role of rigid bronchoscopy in acute airway management while emphasizing the adjunctive value of flexible bronchoscopy in specific scenarios, such as chronic cough, suspected airway malacia, or unexplained stridor.
Secondary bronchoscopy is recommended in patients with persistent symptoms to rule out residual organic material or to remove granulation tissue, thereby preventing complications such as bronchiectasis or lobectomy. 5
Hospital length of stay may vary depending on local health care practices and economic factors Skoulakis et al reported stays ranging from 1 to 11 days, with 65.5% of patients discharged within 2 days. 23 In our cohort, the mean hospitalization was longer, consistent with local clinical protocols.
Limitations
This study has several limitations. Its retrospective single-center design may introduce selection bias and limit generalizability. Variability in radiographic interpretation by different radiologists and clinicians (inter- and intra-observer variability) was not formally assessed, which could affect the reproducibility of findings. In addition, heterogeneous chest X-ray protocols—including differences in projection (AP vs lateral), image quality, and technical factors—may have influenced diagnostic accuracy. Bronchoscopy was used as the reference standard; however, not all patients underwent this procedure, potentially leading to misclassification of true positive and false negative cases. Finally, the relatively small sample size limits the statistical power and precision of predictive value estimates. Future prospective multicenter studies with standardized imaging protocols and assessment of interobserver agreement are warranted to validate these findings.
Conclusions
FBA remains a pediatric emergency that requires prompt recognition and timely intervention. Our study demonstrates that chest radiography, although widely used as an initial diagnostic tool, has limited accuracy when used in isolation. With a PPV of 59% and an NPV of 60%, chest X-ray findings often lead to both false positive and false negative results. While auscultation alone showed a higher predictive value, the combination of clinical examination and imaging significantly improves diagnostic reliability. These results emphasize the importance of a structured diagnostic approach that integrates clinical assessment, radiographic evaluation, and early bronchoscopy. Focusing on timely diagnosis, particularly in high-risk age groups, and implementing individualized management strategies are key to reducing morbidity associated with this potentially life-threatening condition.
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from the Ethical Committee of University Hospital in Brno (03-041120/EK).
Consent to Participate
Informed consent for data processing was obtained from the parents or legal guardians at the time of patient admission. Given the retrospective nature of the study, no additional consent was required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Health of the Czech Republic, Conceptual Development of Research Organization (FNBr, 65269705), and Masaryk University in Brno (MUNI/A/1543/2024).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.