
Abstract
Introduction
Congenital epiglottic cysts are rare disorders of the larynx found in neonates and infants. The cysts are mainly observed on the lingual surface of the epiglottis, present early with symptoms such as laryngeal stridor and inspiratory dyspnea, and are life-threatening in severe cases. Currently, surgical resection is the main treatment modality. However, the number of reported cases in the literature is limited, with most reported as individual cases. In recent years, low-temperature plasma radiofrequency ablation is being widely used in otorhinolaryngology. This study aimed to explore the usefulness of low-temperature plasma radiofrequency ablation for treating congenital epiglottic cysts.
Patients and Methods
Patient Information
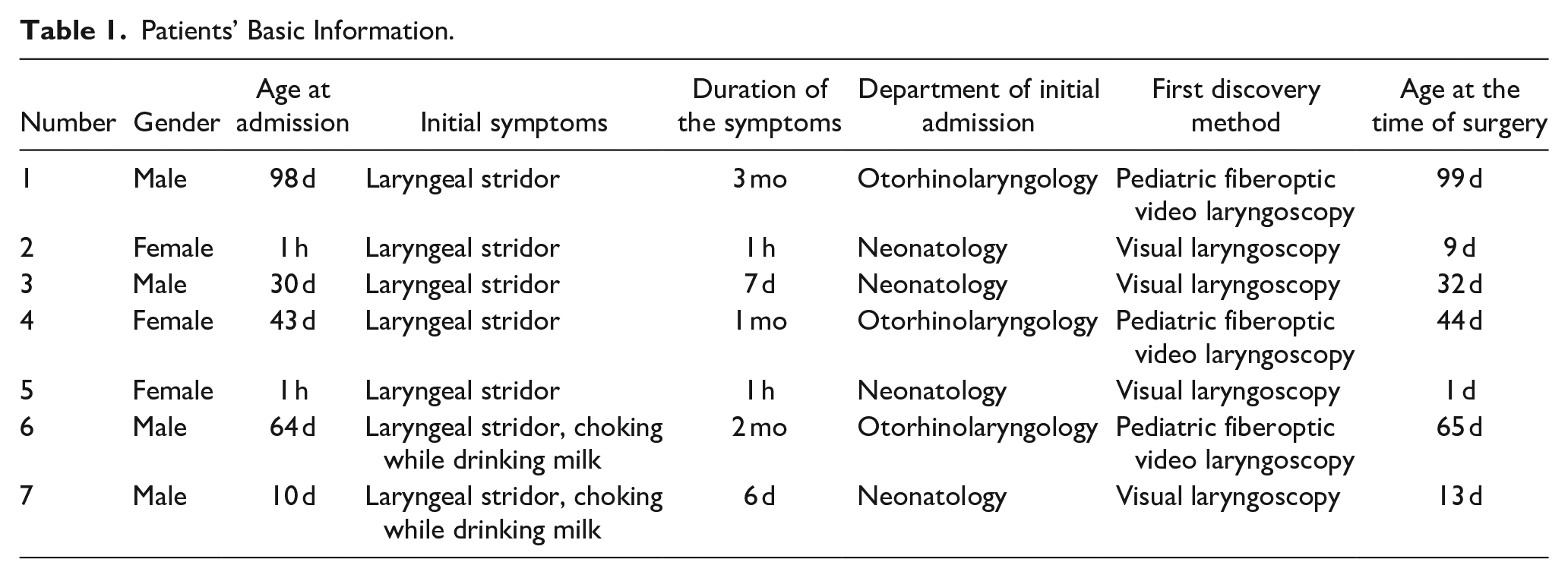
A total of 7 children (4 males and 3 females) who underwent low-temperature plasma radiofrequency ablation for the resection of congenital epiglottic cysts at the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University between March 2018 and March 2023 were selected. Of these, 2 presented with dyspnea within 24 hours of birth and required urgent endotracheal intubation. Patients’ age at the time of surgery ranged from 1 day to 99 days (average, 37.57 ± 35.01 days). The main clinical manifestations were laryngeal stridor with labored breathing. Four patients were admitted to the neonatology department and the remaining were treated in the otorhinolaryngology department. All children had preoperative epiglottic neoformation on pediatric fiberoptic video laryngoscopy or visual laryngoscopy and were pathologically diagnosed with epiglottic cysts. Routine preoperative tests such as electrocardiography; chest radiography; and blood, coagulation function, and liver and kidney function tests revealed no obvious contraindications to surgery (Table 1). The Medical Ethics Committee of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University approved this study, and all patients’ families provided informed consent (Approval Number: 2020-02).
Patients’ Basic Information.
Methods
Children were assessed preoperatively by an anesthesiologist, and if intubation was difficult, a portion of the cyst fluid was aspirated using a puncture needle to reduce the cyst volume. After successful orotracheal intubation, a supporting laryngoscope was inserted, the base of the tongue was lifted, and the cyst was fully and clearly visualized using an endoscope or microscope. A low-temperature plasma surgery system (ArthroCare ENT Cobrator II system; ArthroCare Corporation) was used for epiglottic cyst resection. During surgery, microsurgical laryngeal forceps were used to clamp and pull up the cyst wall, and using the matching low-temperature plasma (EIC7070-01; ArthroCare Corporation), the cyst was cut and ablated along the junction of the cyst wall and normal tissue. While cutting, hemostasis was performed to ensure that the surgical field was clear, the depth reached the surface of the perichondrium, and the cyst was completely removed. Simultaneously, electrocoagulation was performed on the base of the cyst. The epiglottis cartilage and the surrounding normal tissues were preserved. During the operation, the cutting gear of low-temperature plasma was 5 to 6, the coagulation gear was 3 to 4. The cutting and coagulation operation measures were implemented in the form of control pedal. Following surgery, antibiotics were administered to prevent infection. In addition, budesonide suspension atomization detumescence were used for symptomatic relief of inflammation.
Results
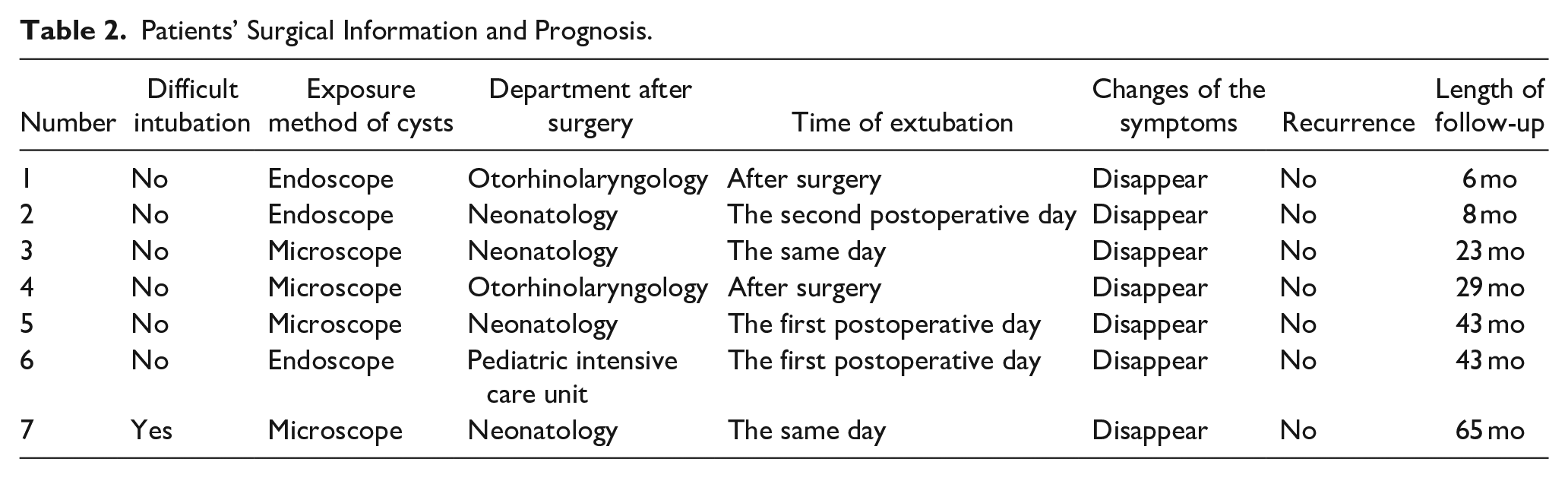
One child was difficult to intubate but was successfully intubated after aspiration of cyst fluid. The procedure was successfully completed without a tracheostomy in all children. Two patients returned to the ENT ward postoperatively, and 5 patients returned to the pediatric intensive care or neonatology ward with postoperative tracheal intubation; of these, 2, 2, and 1 patient were extubated on the same day, first postoperative day, and second postoperative day, respectively. Laryngeal stridor and dyspnea improved significantly after extubation in all children. The patients were followed up for 6 months to 5 years postoperatively, with no recurrence and the efficacy was satisfactory (Table 2).
Patients’ Surgical Information and Prognosis.
Discussion
Epiglottic cysts can be classified as congenital or acquired. Congenital epiglottic cysts originate from the endodermal and mesodermal cells in the embryonic stage and are a rare embryonic disorder. They have a thin cyst wall and are caused by pathological blockage of the laryngeal ependymal sac or gland tube. The incidence of congenital epiglottic cysts is relatively low (approximately 1.82/100,000 newborns). 1 Because the pharynx is narrower in neonates and infants than in adults, clinical symptoms of congenital epiglottic cysts can occur during the early postnatal period, even if the cyst volume is small. Congenital epiglottic cysts usually manifest as difficulty in feeding, wheezing, and vague crying. In severe cases, cyanosis, dyspnea, or suffocation may occur. Children often require hospitalization owing to lower respiratory tract symptoms such as neonatal pneumonia, aspiration pneumonia, bronchitis, and in severe cases, pneumothorax and pneumomediastinum; therefore, pediatricians who focus on pulmonary symptoms and ignore the pharyngeal condition may miss the diagnosis, leading to treatment delay. 2 Delayed diagnosis and treatment pose a threat to the growth and development of the child, and even their life. 3,4 During neck examination, obvious wheezing sounds can be heard near the chin and gradually weaken down to the anterior superior sternum, which is different from the physical signs of lung lesions and helps identify upper respiratory tract lesions in the early stages. It has also been suggested that neck position-dependent fluctuation in symptoms is a diagnostic clue. 5
Electronic laryngoscopy is the easiest and most direct test to diagnose congenital epiglottic cysts, provides a comprehensive view of the cyst location and size, and allows exclusion of other lesions in the larynx. 6 A congenital epiglottic cyst typically presents as a translucent cystic mass with a smooth surface near the base of the tongue or epiglottis. Prevention of cyst rupture and avoiding spillage of cystic fluid are necessary to prevent aspiration or asphyxia. An initial diagnosis can be made using electronic laryngoscopy to ensure minimal pharyngeal irritation and trauma. However, once a congenital epiglottic cyst is diagnosed, surgery should be performed as soon as possible. In this study, epiglottic cysts were primary diagnosed using pediatric fiberoptic video laryngoscopy in 3 children and visual laryngoscopy in 4 children. The differential diagnosis of congenital epiglottic cysts includes thyroglossal duct cysts, ectopic thyroid glands, and congenital laryngomalacia; and B-ultrasound, computed tomography, and magnetic resonance imaging of the neck are helpful for the diagnosis.
Surgical resection is the preferred treatment for congenital epiglottic cysts. Common surgical options include cyst incision and fluid extraction, CO2 laser resection, low-temperature plasma radiofrequency ablation, and high-frequency electrocautery. 7,8 Neonates and infants with narrow and concealed pharyngeal cavities, abundant submucosal lymph nodes in the larynx, loose connective tissue, and repeated irritation are prone to edema. In addition, the blood supply to this site is abundant, and intraoperative bleeding can easily cause blurring of the surgical field. Neonates and infants have smaller surgical cavities than adults. If it is difficult to resect the cyst completely, part of the cyst fluid may be aspirated to reduce the cyst volume, and the cyst wall may be excised in blocks. Resection of most of the cyst wall and exposure of the basal part to avoid healing of the residual cyst wall may prevent recurrence and achieve therapeutic purposes. 9 Postoperative complications include bleeding, epiglottic cartilage necrosis, defects, deformation, and epiglottis—tongue-base adhesions.
High-frequency electrocautery is a conventional surgical method and has several disadvantages such as greater thermal damage to the surrounding normal tissues, longer postoperative wound healing time, higher incidence of postoperative complications, and higher recurrence rates. CO2 laser resection and low-temperature plasma radiofrequency ablation are minimally invasive techniques that have emerged in recent years. CO2 laser generate strong thermal effects that can cut, vaporize, and solidify biological tissues. The advantages include efficient soft tissue incision, minimal thermal damage, and a mild postoperative inflammatory response, that are conducive to wound healing. However, it requires expensive equipment, cumbersome operations, and surgeons with high proficiency to avoid serious consequences, such as laser injury. 10
Low-temperature plasma radiofrequency ablation is increasingly used for otolaryngological procedures, such as tonsillar adenoidectomy, excision of nasal masses, and excision of laryngeal masses. 11 -14 Shorter operation time, fewer patient complications, and a higher treatment efficiency than conventional procedures have been confirmed by otolaryngologists. Application of low-temperature plasma radiofrequency ablation for the treatment of early glottis carcinoma results in small thermal damage to the tissue owing to the low cutting temperature. Furthermore, intraoperative bleeding is less, and the surgical time is short, thereby reducing the impact on the patient. In addition, postoperative wound pain is mild, recovery is rapid, and the incidence of adhesions is low. 15 However, it is less commonly reported for the treatment of epiglottic cysts. In our department, low-temperature plasma radiofrequency ablation has recently been used to treat congenital epiglottic cysts. The cyst is exposed under a microscope or endoscope to distinguish the cyst wall from normal tissue, and low-temperature plasma radiofrequency ablation is used to resect the cyst and prevent damage to the surrounding tongue base and normal tissue of the epiglottis. After surgery, close attention should be paid to the child’s respiratory condition; antibiotic therapy and other symptomatic treatments can be administered to promote recovery. In our study, all 7 patients recovered well postoperatively; no surgical complications occurred, and no recurrence was observed during follow-up.
Low-temperature plasma radiofrequency ablation has some limitations such as higher cost, relatively coarse low-temperature plasma, and lower precision than CO2 laser. However, it has a better hemostasis effect, a shorter operation time, and faster postoperative recovery compared with CO2 laser resection. 16 Moreover, combining low-temperature plasma radiofrequency ablation with microscopy or endoscopy can improve the surgical precision and reduce damage in neonates and infants.
Conclusion
In conclusion, the study findings indicate that low-temperature plasma radiofrequency ablation is suitable for the treatment of congenital epiglottic cysts. This study included a small number of cases, and further studies with larger sample sizes are required.
Footnotes
Data Availability Statement
The data used and analyzed in this study are included in the article or are available from the corresponding and first authors on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.