
Abstract
An uncommon benign condition in neonates, known as congenital epiglottic cyst, can lead to symptoms such as neonatal dyspnea, laryngeal stridor, and, in severe cases, even pose a potential threat of asphyxia-related mortality. A congenital epiglottic cyst is one of the neonatal emergencies. Fibrolaryngoscopy is the predominant method of diagnosis, and early identification, diagnosis, as well as treatment are the key points. Successful endoscopic ablation of congenital epiglottic cysts in 3 newborns was achieved through the utilization of a low-temperature plasma radiofrequency ablation system. Consequently, the purpose of this case report is to assist pediatric emergency physicians in the timely identification of congenital epiglottic cysts with the potential risk of mortality and to provide additional experience in clinical management.
Introduction
Congenital epiglottic cyst, a seldom encountered clinical condition in newborns and infants, remains an elusive ailment with an uncertain etiological basis. Manifesting as chronic or intermittent dyspnea, hoarseness, aspiration, chronic cough, or developmental delays, its emergence continues to puzzle medical practitioners. 1 Historically, laryngeal cysts have been divided into 2 types, based on De Santo; one is the ductal cyst, which retains mucous, and the other is a saccular cyst, which arises from the laryngeal saccule. 2 Moreover, congenital epiglottic cyst in newborns and infants is a rare disease being treated in the clinic, and its formation mechanism is still unidentified. Besides, the early clinical diagnosis depends on clinical symptoms and fiber optic nasopharyngeal laryngoscopy, and imagining examination if required. Furthermore, treatment options such as needle aspiration and endoscopic cyst resection, 3 low-temperature plasma radiofrequency (LPRF) for congenital epiglottic cysts in infants are rarely reported in clinical practice. Three cases of congenital epiglottic cysts in newborns and infants are reported.
Case Report 1
A male infant, aged 2 months, was hospitalized on account of experiencing breathing difficulties accompanied by choking and coughing while feeding for a duration exceeding 1 month. Moreover, upon admission, the physical examination unveiled signs of tachypnea, a faint bluish discoloration of the lips, the absence of 3 concave breath signs, unimpeded passage of the gastric tube, and the identification of a sleek cystic mass positioned on the left aspect of the epiglottis and at the base of the tongue. This mass effectively obscured the epiglottis, rendering the glottis unobservable (refer to Figure 1a). Moreover, blood examination at admission did not indicate an abnormality in coagulation, routine blood tests, as well as biochemical tests, leading to the diagnosis of congenital epiglottic cyst. During the operation, it was discovered that the viscous fluid of the pus cyst had overflowed, and part of the cyst wall was cut and sent to pathology. In addition, 1 week following the operation, the laryngoscope reexamination showed that the cyst-like neoplasm of the epiglottis and the base of the tongue disappeared, the white pseudo lemma was attached, the morphology of the epiglottis was normal, and the glottis was not exposed (poor child cooperation) (refer to Figure 1b). Similarly, the postoperative condition was stable and he was returned to the neonatal ward with tracheal intubation, and a tracheotomy was not necessary. The patient was extubated 24 hours after surgery and breathed normally without subsequent stridor. Promptly resuming oral feeding, the patient’s postoperative pathological assessment disclosed chronic mucosal inflammation marked by cystic degeneration and excessive fibrous tissue proliferation (Figure 1c). A follow-up conducted after 3 months demonstrated a complete absence of recurrence, and the child exhibited no symptoms whatsoever. Consequently, no postoperative computed tomography scan was deemed necessary.
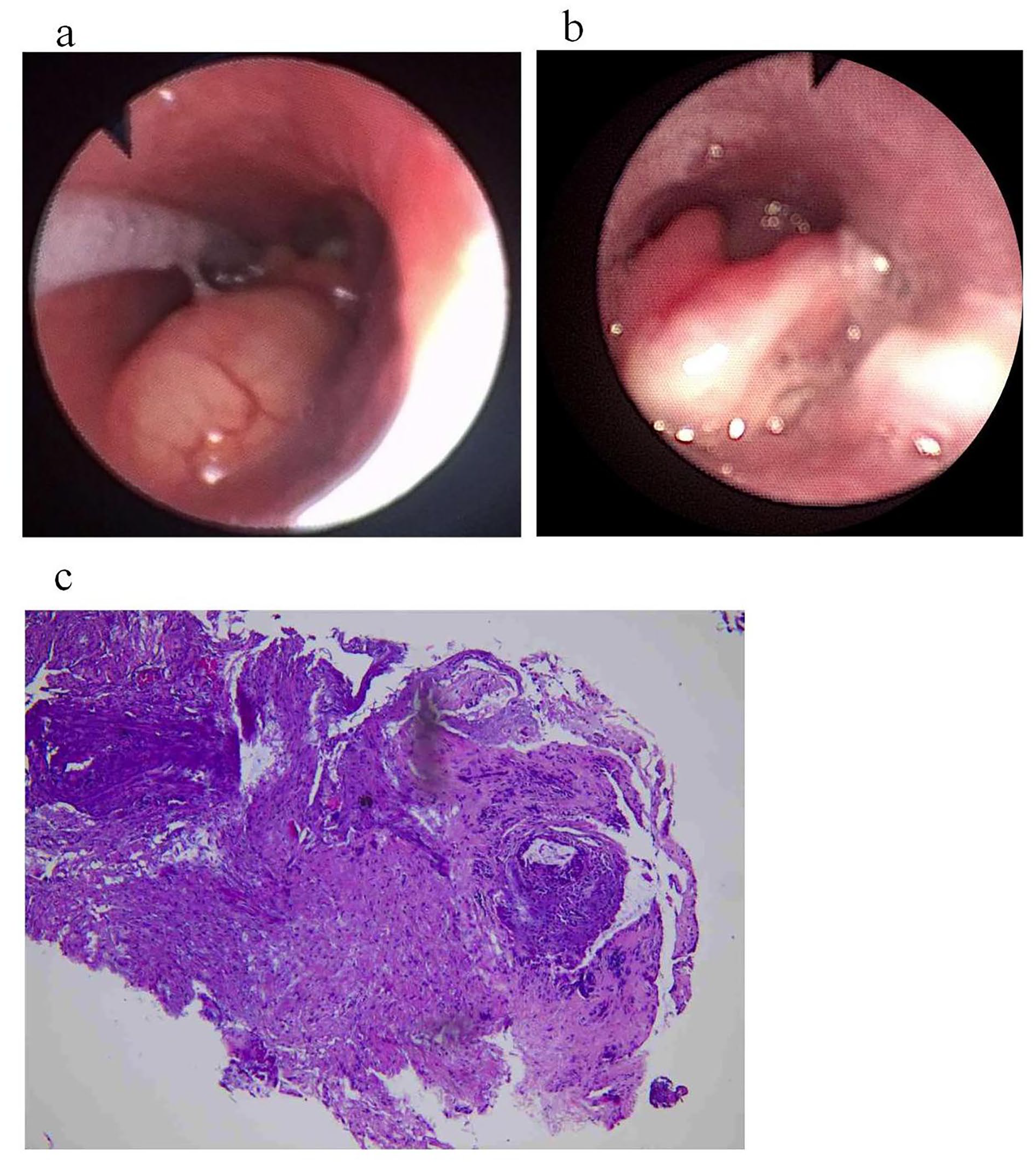
(a) A cyst-like mass on the lingual surface of the epiglottis was seen under an electronic fibrolaryngoscope. (b) After low-temperature plasma ablation, the mass disappeared, a small amount of white pseudomembrane was attached, and there was no swelling of the epiglottis. (c) Hematoxylin-eosin staining showed chronic mucosal inflammation with cystic degeneration and fibrous tissue hyperplasia.
Case Report 2
An 8-day-old boy was admitted to the hospital for dyspnea for 5+ days, and the child was admitted to another hospital due to “poor feeding.” On the same day, he developed dyspnea, which manifested as moaning, shortness of breath, lack of apnea, lack of irritation, restlessness, and drowsiness. Immediately after non-invasive-assisted positive pressure ventilation, dyspnea was nevertheless evident and oxygen saturation could not be recovered, and they were transferred to our hospital for treatment. Furthermore, physical examination at admission revealed 3 concavity signs (−): an unobstructed gastric tube, a smooth cystoid mass on the left side of the lingual surface of the epiglottis, and a spacious glottis (refer to Figure 2a and b). APTT: 32.8 seconds, D-dimer: 1.27 μg/mL, white blood cell count: 25.15 × 109/L, absolute neutrophil count: 13.73 × 109/L, and biochemistry was normal. Upon bedside assessment, the anteroposterior position of the chest revealed a mild increase in bilateral lung density, leading to a provisional diagnosis of the congenital epiglottic cyst. During the operation, the viscous yellow secretion was spilled, and part of the cyst wall was cut off and sent to pathology. Moreover, 2 weeks following the operation, the laryngoscope reexamination illustrated that the cyst-like neoplasms on the lingual surface of the epiglottis disappeared, the white pseudo lemma was attached, and the epiglottis had normal morphology, and the glottis was not exposed (poor child cooperation) (refer to Figure 2c). The postoperative condition was stable and he was returned to the neonatal ward with tracheal intubation. The patient underwent extubation 24 hours following the surgical procedure and exhibited unimpeded respiration without any subsequent occurrence of stridor. He swiftly resumed oral feeding. Subsequent postoperative pathological analysis indicated the presence of epidermal mucosal polyps characterized by squamous epithelial cell proliferation (refer to Figure 2d). A follow-up performed 1 month later indicated no signs of recurrence and the child was completely asymptomatic.
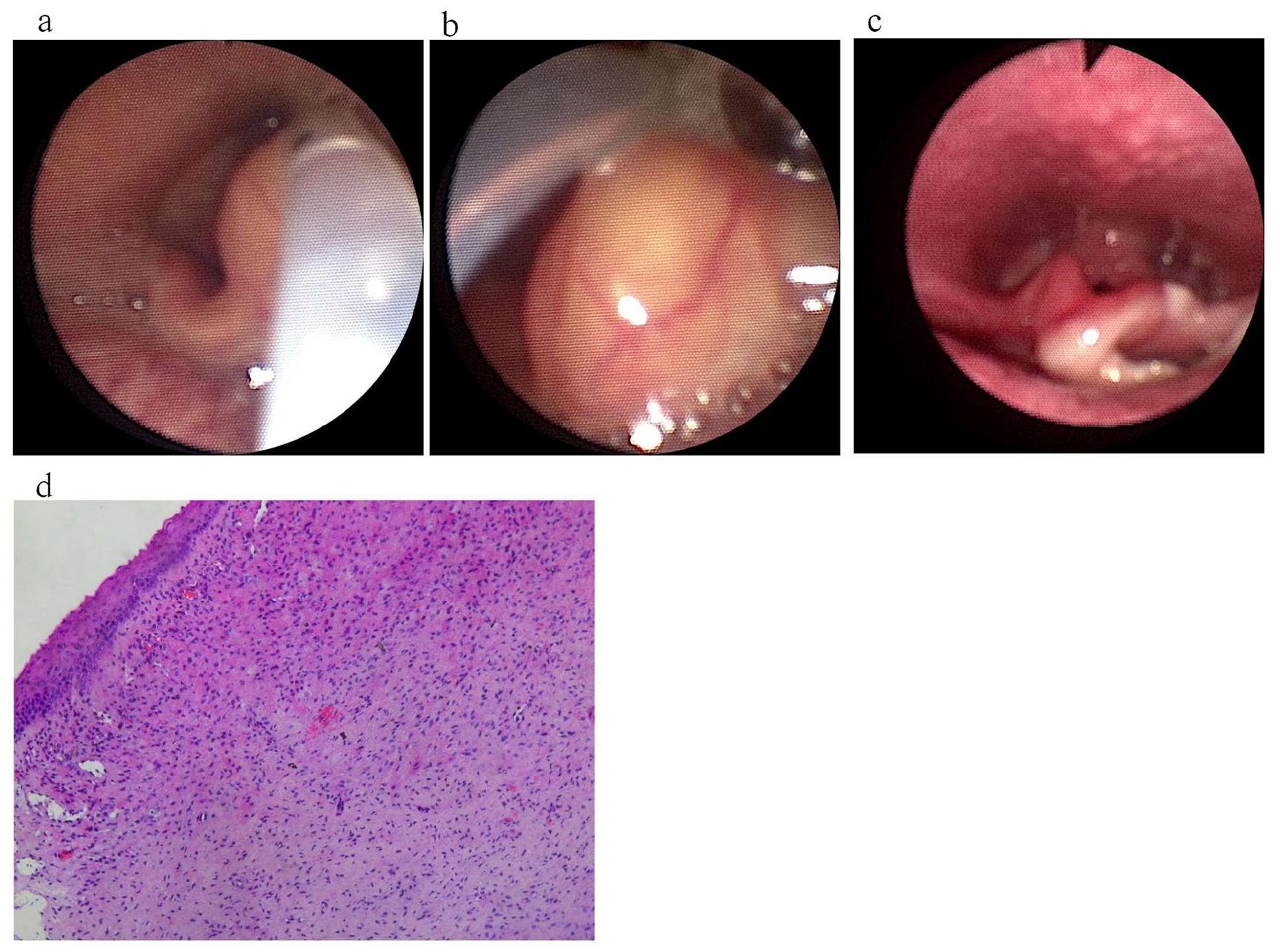
(a, b) The electronic fibrolaryngoscope showed a yellow cyst-like mass on the left side of the lingual surface of the epiglottis, and the gastric tube was patent and in place. (c) The mass disappeared after ablation, and there was no swelling in the operative area and epiglottis mucosa. (d) Hematoxylin-eosin staining showed epidermal mucosal polyps with squamous epithelial cell proliferation.
Case Report 3
A 5-day-old boy was admitted to the hospital due to dyspnea for 5+ days. Besides, an oval cyst about the size of a quail egg was noticed in the pharynx under the laryngoscope, which was treated by a gastric tube, and the child was transferred to our hospital for treatment. At admission, a physical examination revealed 3 concave respiratory signs (−): an unobstructed gastric tube, and an electronic laryngoscope revealing a smooth yellowish mass on the right lingual surface of the epiglottis (Figure 3a). Moreover, the routine blood test illustrated that the absolute neutrophil count was 10.09 × 109/L, and the blood coagulation and biochemical tests were normal. In addition, the position of the chest anteroposterior on the bedside: bilateral lung texture slightly increased and blurred; changes after tracheal intubation. Except for that, the considered diagnosis was a congenital epiglottic cyst, and thyroid ultrasound revealed that the size and shape of the thyroid gland were normal, the capsule was smooth, the echo was homogeneous, and there were no detected nodules. Color Doppler Flow Imaging (CDFI) represented normal blood flow signals in the glands, and no enlarged lymph nodes were detected in the neck. During the operation, it was determined that the viscous yellow secretion was overflowing and part of the cyst wall was cut and given to pathology (Figure 3b-d). Furthermore, the postoperative condition was stable and the patient was returned to the neonatal ward with tracheal intubation, and the patient was extubated 24 hours after surgery and breathed normally without subsequent stridor; consequently, he quickly resumed oral feeding. Postoperative pathology revealed bleeding in the epidermal mucosa, small blood vessels in the lamina propria, scattered inflammatory cell infiltration, and partial hyperplasia of fibrous tissue (Figure 3e). A follow-up performed 2 weeks later demonstrated no sign of recurrence and the child was completely asymptomatic.
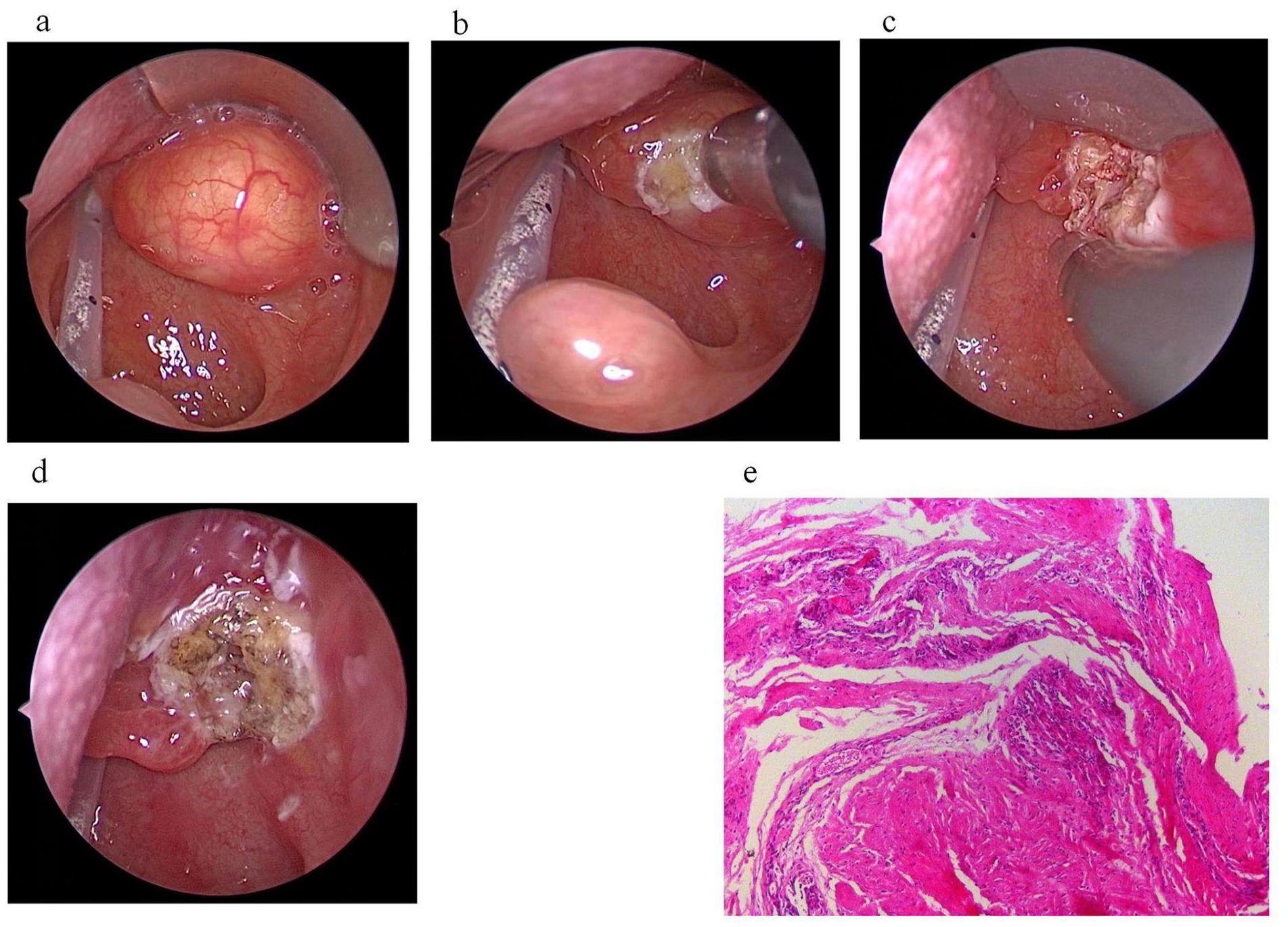
(a) The electronic laryngoscope showed a smooth yellowish mass on the right side of the lingual surface of the epiglottis. (b-d) After ablation, the tumor disappeared, the surgical area became flat, and there was no swelling of the epiglottis and the surrounding mucosa. (e) Hematoxylin-eosin staining showed hemorrhage in the epidermal mucosa, small blood vessels in the lamina propria, scattered inflammatory cell infiltration, and partial fibrous tissue hyperplasia.
Discussion
Initially documented and reported by Abercrombie in 1881, the congenital laryngeal cyst is a rare cause of airway obstruction in infants, with an estimated incidence of 1.82 to 3.49 per 100,000 live births. The majority of laryngeal cysts arise from the vallecula, the aryepiglottic fold, or the ventricle saccule. 4 An epiglottic cyst is one of the most prevalent disorders in otolaryngology. Moreover, DeSanto et al. revealed that epiglottic cysts accounted for approximately 52% of all laryngeal cysts. 5 Congenital epiglottic cysts are fatal for newborns and infants and manifest clinically as dyspnea, stridor, or dysphagia. Besides, congenital epiglottic cysts are rare and their cause is unknown, although they originate from obstruction of the submucosal gland duct as well as expansion of the secondary glandular organ. 6 Except for that, some researchers have divided congenital throat cysts into 2 types, in which the congenital epiglottis cyst belongs to type I. 7 While congenital epiglottic cysts are non-malignant growths, in neonates and infants, substantial cysts located in the epiglottis can potentially obstruct the airway, leading to either respiratory impediments or instances of food inhalation that might result in foreign body obstruction of the trachea. Such occurrences elevate the potential peril of death by asphyxia.
The diagnosis of congenital epiglottic cyst is primarily based on clinical symptoms and nasopharyngeal fiber laryngoscopy. On the whole, nasopharyngeal fiber laryngoscopy can be employed to confirm the diagnosis. Accordingly, gastroesophageal reflux, laryngomalacia, paralysis of the vocal cord, and esophagotracheal fistula should be differentiated from congenital epiglottic cysts. None of these conditions are recognized to cause a worsening of breathing difficulties based on neck position; therefore, the distinctive indicator for congenital laryngeal cysts is airway blockage due to alterations in neck positioning. 8 Inspiratory breathing problems occur on the condition that sucking is interrupted or when coughing, choking, blurred crying, and breathing difficulties are affected by posture. Even a triple concave respiratory sign may be present, and congenital epiglottic cysts should be considered.
Treatment of congenital epiglottic cysts should be based on the symptoms of children and the size of the cyst. For neonates afflicted by sizable cysts with partial glottis exposure, a temporary alleviation of the condition can be achieved through the application of laryngeal spray anesthesia using direct laryngoscopy, followed by the aspiration of cystic fluid. This approach is commonly employed to mitigate instances of acute obstruction within the upper respiratory tract. Its merits encompass a straightforward and expeditious procedure. However, it bears the drawback of a propensity for recurrence, rendering it inadequate as a definitive solution. As an alternative, a 2-stage surgical resection presents a viable option. Furthermore, for those with small cysts and acceptable glottic exposure, tracheal intubation can be performed first, and subsequently, surgical resection can be conducted. 7 Simple cysts can be removed by a laryngoscope, which is prone to bleed after the operation, damages the epiglottic mucosa, causes obvious local edema, and then dyspnea will not be relieved. 9 Surgical resection techniques include direct laryngoscope laryngeal forceps for removal of the cyst wall, external cervical approach for removal of the cyst, dynamic cutting system for removal of the cyst, low-temperature plasma resection of the cyst, and CO2 laser resection. 10 Postoperative complications of surgery should be avoided as much as possible, and the method with small trauma, mild postoperative mucosal reaction, and low recurrence rate of the cyst should be selected. Furthermore, LPRF ablation is widely employed in otolaryngology because of its small intraoperative injury, rapid postoperative recovery, as well as low recurrence rate. Currently, ablation of a congenital epiglottic cyst with LPRF is rarely reported in clinical literature.
LPRF ablation is a new technology that has been rapidly developed in recent years. It adopts the energy of LPRF to form a thin plasma layer between the electrode and the tissue and causes the lesion tissue to liquefy and fall off following denaturation at a lower temperature (approximately 40-70°C), to reduce the damage of the tissue, drastically decrease the pain of patients and shorten the recovery period. The treatment of head and neck hemangioma has currently yielded positive results. When LPRF technology is combined with endoscopic technology, on the condition that the tumor is rich in blood vessels, it can decrease the volume of the tumor, as well as has the functions of resection, hemostasis, irrigation, suction, minimally invasive and precise treatment of nasal, pharyngeal, and laryngeal lesions, reduce bleeding, as well as postoperative mucosal swelling, and subsequently reduce the incidence of complications.11, 12 LPRF is preferred for newborns and infants with young age and low immunity. The tissue of the epiglottic cyst was subjected to carbonization and subsequently vanished. Throughout the surgical procedure, minimal bleeding and negligible harm were inflicted upon the adjacent tissues of the pediatric patients. After the operation, the children were transferred to the neonatal department, and the tracheal intubation was effectively removed 24 hours following the operation, and the patient was discharged from the hospital.
Conclusion
The low-temperature plasma system integrates ablation, hemostasis, and suction. In addition to low-temperature operation, it retains benefits in a precise location, light collateral damage, noncarbonization of the wound surface, 13 light postoperative response, fewer complications, and faster recovery, in comparison to traditional operation. In combination with the endoscopic system with different angles, it can fully expose the surgical field and is particularly suited for the surgical treatment of congenital epiglottic cysts in newborns and infants, a technique that deserves to be more widely used in the clinic. 14
Footnotes
Acknowledgements
Not applicable.
Author Contributions
All the authors contributed to the conception and design of the study. Material preparation, data collection, and analysis, GSS and CCX and writing—original draft preparation, LQL and YHP. All authors participated in the review and editing of the previous versions of the manuscript. All authors have read and approved the final manuscript.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written consent has been obtained from the patients to publish all relevant data.