
Abstract
Keywords
Introduction
In addition to the 3 nasal bones that make up the “tripod,” the location and health of the septal angle and the fibrocartilaginous connections between the lower lateral cartilages and the septum-upper lateral cartilage complex all have a role in how far the nasal tip may be pushed out. The location and integrity of the septal angle, in turn, depend on the presence of strong dorsal and caudal cartilaginous struts and an intact nasal spine. The short nose normally has none of these issues. 1
To improve projection at the tip, septocolumellar suturing can be used to move the columella forward along the septum, or the medial crural support can be lengthened using a cartilaginous strut. Although increasing projection by grafting cartilage to the tripod’s 3 legs is theoretically possible, the resulting structure is not robust enough to resist the effects of scarring. Projection can be enhanced with tip grafts, especially if they are put above the caudal border of the dome cartilage. More than one layer of cartilage may be required when the skin is exceptionally thick. 1
Nasal tip projection is the amount by which the nasal tip protrudes beyond the frontal plane of the face. Numerous nasofacial metrics have been developed to define the perfect tip position. Goode defined an optimal size of projection when the alar-facial groove to the nasal tip measures 0.55 to 0.60 of the distance from the nasion to the nasal tip, generating a 36° nasofacial angle. According to Simons, in a perfectly projected nose, the distance from the subnasale to the tip defining point would be the same as that from the subnasale to the vermilion border of the upper lip. According to Crumley’s 3-4-5 ratio, the nose should have a right-angle shape, with the nasion, tip-defining profile, and alar crease as the 3 vertices.2,3 The Anderson tripod hypothesis of tip projection will be discussed, and the most common methods for removing the projection will be described in detail, including (1) transfixion incision, (2) medial or lateral crural overlay, and (3) dome truncation. 3
More so than with any other surgical treatment, rhinoplasty requires thoroughly comprehending the patient’s goals and anxieties. 4 It is crucial to learn the patient’s motivations for pursuing rhinoplasty. Preoperatively, the patient must be given accurate information about what rhinoplasty can and cannot do. This is why so many experts advise double checking with prospective rhinoplasty patients before committing to surgery. 5
Patient satisfaction following rhinoplasty procedures involving the nasal tip was compared between the classical tongue-in-groove (TIG) technique and the triple cartilage combining suture (TCCS; flexible tongue-in-groove) in the current study.
Patients and Methods
The Otolaryngology Clinics at Bilecik Training and Research Hospital, Baypark Hospital, and Dr. Oguzhan Oguz Wellnose Clinic, as well as the Otolaryngology Departments at King Saud University, Eskisehir Osmangazi University, and Kırıkkale University, are participating in this retrospective and multicentric study. Ethics committee approval was obtained from T.R. Bilecik Şeyh Edebali University, Non-Invasive Clinical Research Ethics Committee (Date: 05.12.2023, Number: 8/4). Due to the retroactive nature of the analysis, permission is unnecessary.
Subjects
Eighty people were evaluated for this study, all of whom had rhinoplasty performed, with either the classical TIG technique 6 or the TCCS (flexible tongue-in-groove) technique 7 (Figure 1) being used on the tip area. Patients were chosen among those who submitted applications to Eskisehir Osmangazi University’s Otolaryngology Department. In all cases, open rhinoplasty protocols were followed. Forty consecutive patients undergoing each technique chosen for including patients into the groups. Forty patients were assigned to group 1 for traditional TIG technique (Figure 2). Group 2 included 40 individuals with the TCCS (flexible TIG) procedure (Figure 3). Patients in Group 1 had a mean age of 28.70 ± 8.51 (ranging from 18 to 48) years, whereas those in Group 2 had a mean age of 28.17 ± 8.56 (ranging from 18 to 53) years.
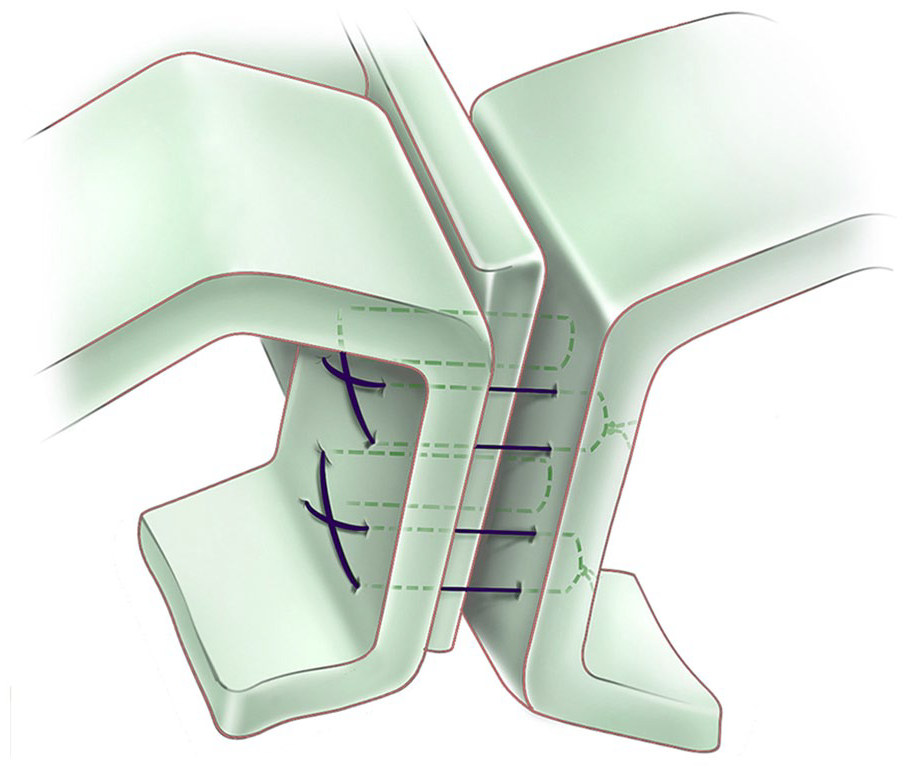
Triple cartilage suture (flexible tongue-in-groove) technique. 7
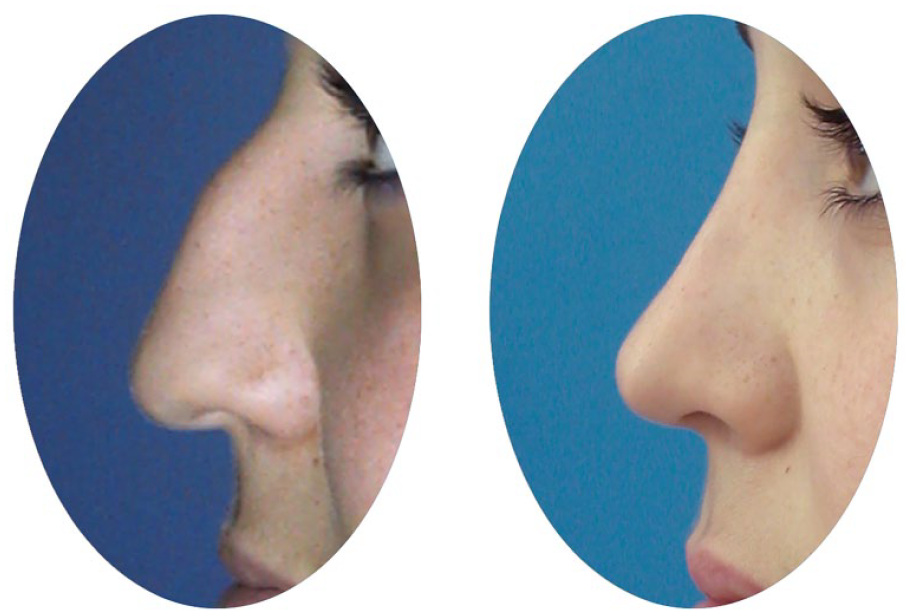
Traditional tongue-in-groove (TIG) technique: preoperative and postoperative first-year view.
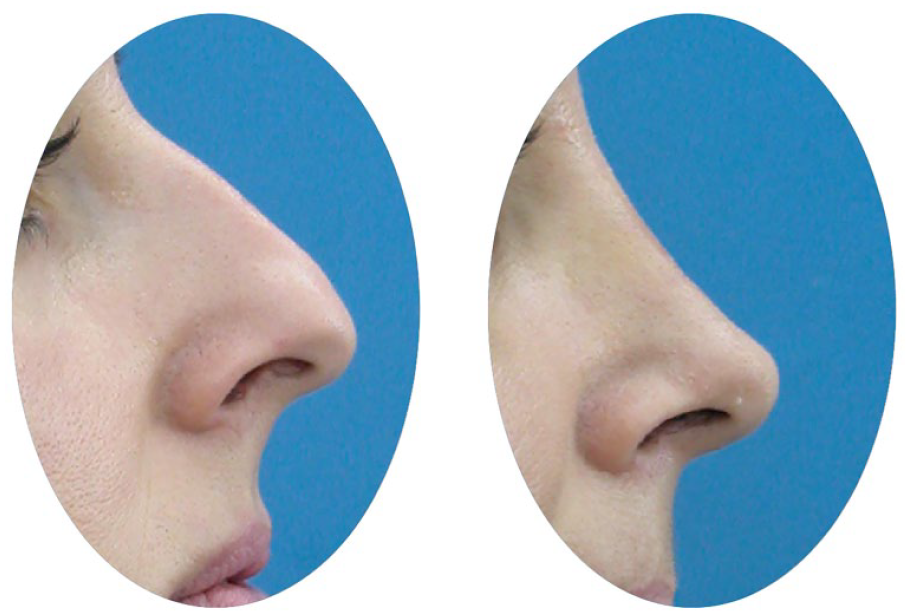
Triple cartilage combining suture (TCCS; flexible tongue-in-groove) technique: preoperative and postoperative first-year view.
Inclusion Criteria
Patients who underwent TIG or TCCS techniques.
At least 1 year follow-up evaluation of the patients.
Exclusion Criteria
The study did not include patients who did not come for 1 year follow-up.
Methods
All patients in groups 1 and 2 were evaluated by the criteria written below at preoperative, postoperative first month, and postoperative first year:
Rhinoplasty Outcomes Evaluation Questionnaire (ROE): There are a total of 6 questions covering psychological, interpersonal, and physiological factors on this scale. The ROE asks patients to assess the look and function of their nose, emotional confidence, and desire for change, as well as the manner in which their nasal appearance affects their personal, social, and professional lives. Each of the 6 items is graded on a scale from 0 (the most negative) to 4 (the most positive) points. The scaled instrument score is calculated by taking the overall score and dividing it by 24, then multiplying the result by 100. The scale runs from 0 to 100, with 0 indicating the least satisfied patients and 100 the most satisfied ones.8-10
Tip projection (cm)
Nasal dorsum length (cm)
Tip projection ratio (Goode): As the nasion (N), alar base-cheek junction (A), tip defining point (T) were found, the Goode ratio wase defined as AT/NT.11-13
Nasofrontal angle
Nasolabial angle
Statistical Analysis
The data collected in this study were analyzed using the SPSS for Windows 16.0 software (SPSS, INC, an IBM Company). Mann-Whitney U test, independent samples t test, and Spearman’s rho efficient test were used.
A value of P < .05 was considered statistically significant.
Results
In the TIG group, there were 10 males (25.0%) and 30 females (75.0%). In the TCCS group, there were 14 males (35.0%) and 26 females (65.0%; P = .329, χ2: 0.952).
Follow-up times of the TIG group were 84.32 ± 19.38 months (ranging from 60.0 to 132.0 months), and of the TCCS group was 87.47 ± 18.01 months (ranging from 63.0 to 142.0 months; P = .305).
ROE Scores and Measurement Values at Preoperative, Postoperative First Month, and First Year
Preoperative, postoperative first-month and first-year tip projection (P = .013, P = .022, and P = .020, respectively), and nasal dorsum length values (P = .009, P = .020, and P = .020, respectively) of the TCCS group were significantly lower than those in the TIG group (Table 1).
ROE Scores and Measurement Values at Preoperative, Postoperative First Month and First Year.
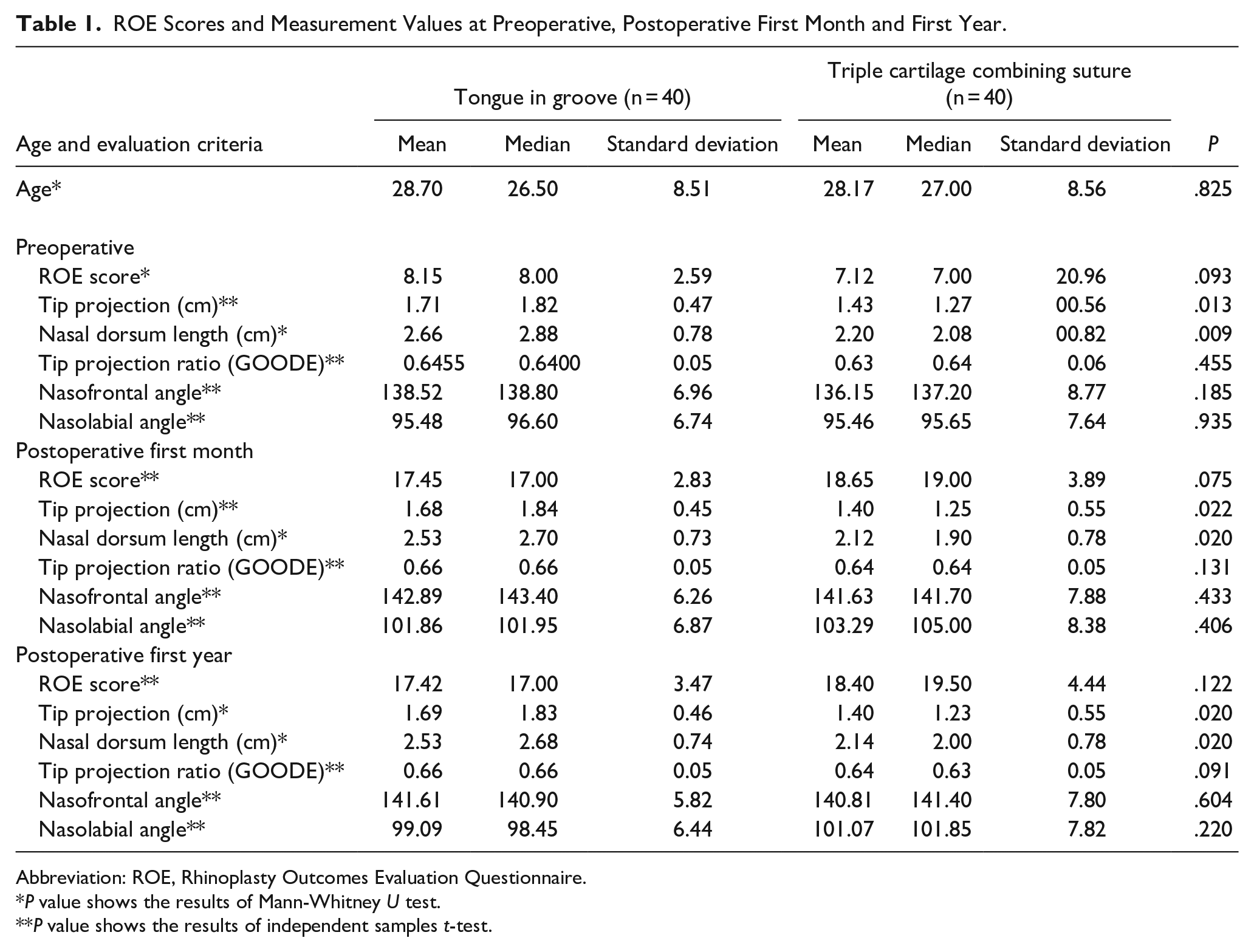
Abbreviation: ROE, Rhinoplasty Outcomes Evaluation Questionnaire.
P value shows the results of Mann-Whitney U test.
P value shows the results of independent samples t-test.
There were no significant differences between TIG and TCCS groups for ROE scores (P = .093, P = .075, and P = .122, respectively), tip projection ratio (GOODE; P = .455, P = .131, and P = .091, respectively), nasofrontal angle (P = .185, P = .433, and P = .604, respectively), and nasolabial angle values (P = .935, P = .406, and P = .220, respectively) at each of the preoperative, postoperative first month, and postoperative first year (P > .05; Table 1).
Correlation Test Results
There was a positive correlation between the postoperative first month and postoperative first year’s ROE scores (P = .000, r = .766; Table 2).
Correlation Test Results.
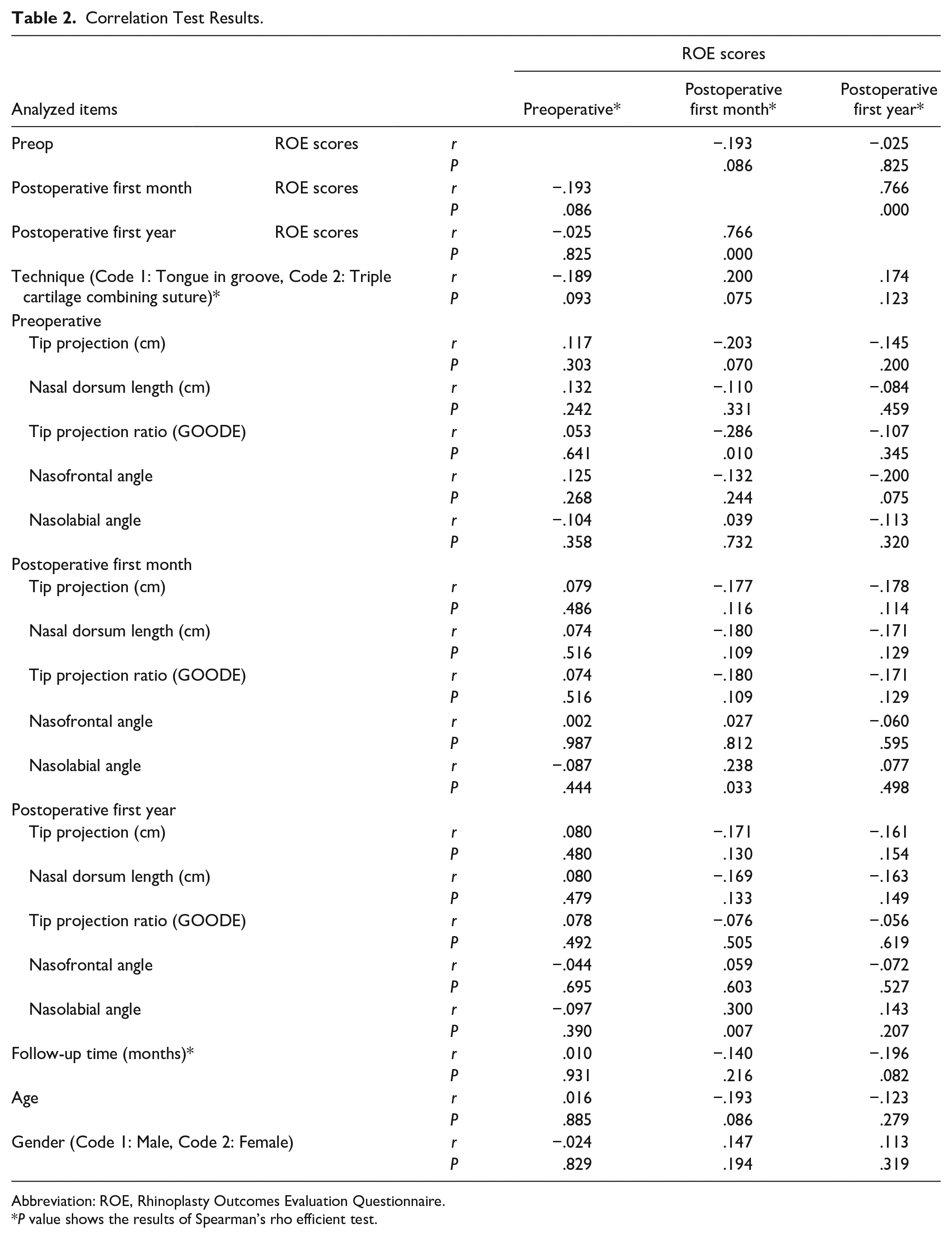
Abbreviation: ROE, Rhinoplasty Outcomes Evaluation Questionnaire.
P value shows the results of Spearman’s rho efficient test.
In patients with lower preoperative tip projection ratio (GOODE) values, ROE scores increased at the postoperative first month (P = .010, r = −.286; Table 2).
At, the postoperative first month (P = .033, r = .238) and first year (P = .007, r = .300), in patients with higher nasolabial angle values, ROE scores increased postoperative first month (P < .05; Table 2).
Discussion
As the nose shape greatly influences face attractiveness, rhinoplasty has a considerable effect on facial beauty. People with unattractive noses can get good outcomes from rhinoplasty surgery. Preoperative planning for rhinoplasty is aided by a plethora of information provided by the new guidelines. 14 By creating a more harmonious overall facial profile, cosmetic rhinoplasty can boost self-perception and confidence. 15
This study examined how TIG and TCCS procedures for reshaping the nose tip affected patient satisfaction. Patients in the TIG group were followed for 84.32 ± 19.38 months, whereas those in the TCCS group were followed for 87.47 ± 18.01 months. Our data indicated that the TCCS group had shorter noses, shorter tip projections, and nasal dorsum length measurements before and after surgery, as well as after 1 year.
There was a favorable relationship between ROE scores in the first month and the first year after surgery. Lower preoperative tip projection ratio (GOODE) values and greater nasolabial angle values were connected to higher ROE ratings, demonstrating patient satisfaction. Despite the lack of statistical significance, it is hypothesized that the TCCS group’s reduced tip projection results may be linked to higher patient satisfaction due to their more realistic look.
The triple cartilage combines the suture (TCCS) method to fuse the 2 medial crural cartilages with the septal cartilage. It is a variation on previously published nasal approaches, as are most modern methods. While maintaining the patient’s natural appearance and feel, this method may be used to accomplish nasal tip rotation, reliably alter tip position, and reduce excess columellar show. 7
Correcting excessive columellar show and keeping caudal deviation under control is possible using the TIG procedure. It can be coupled with an external or endonasal rhinoplasty to manage nasal tip rotation and projection without compromising the lobular cartilaginous complex. It is often used in tandem with other septorhinoplasty techniques. During the TIG procedure, a gap is formed between the medial crura and the caudal septum, and the crura is then moved cephalon-posteriorly onto the septum. The TIG method is a tried-and-true, repeatable approach to controlling columellar show and producing consistent, repeatable tip rotation and projection. 16
Facial proportions are quantitative indicators for judging facial beauty and attractiveness. Nasofrontal, nasolabial, nasofacial, nasomental ratios, nasal tip projections, and nasal lengths are facial parameters and proportions.17-19 Despite variations in average face dimensions and ratios among age ranges, races, and sexes, 20 optimal facial proportions have been identified across ethnicities and sexes. 21
The degree to which patients are satisfied with their rhinoplasty is a qualitative and subjective measure of the procedure’s success. 22 Patient satisfaction and the positive outcome of rhinoplasty depend on several criteria, including but not limited to gender, 23 patient perception, 24 preoperative nose shape, 25 nasal breathing function, 26 and patient psychology. 25
A thorough evaluation of the nose and nasal airway before rhinoplasty and an understanding of what the patient and surgeon hope to achieve are prerequisites for good outcomes. In addition to these issues, a consideration of several intra- and postoperative points, such as restoring the normal anatomy, correcting the deformity using incremental control, and preserving the nasal airway during surgery as well as during postoperative care and the proper management of complications, lead to a successful rhinoplasty outcome. 26
Changes in facial characteristics and proportions, as well as greater satisfaction with nose shape, were documented 6 months following rhinoplasty in research by Zojaji et al. 27 However, the face proportions were not correlated with the level of enjoyment.
Body dysmorphic disorder was found to be a predictor of postoperative unhappiness, 28 according to research by Picavet et al. Patients who meet the “SIMON” characteristics (single, immature, masculine, overexpecting, and narcissistic) are not the best candidates for rhinoplasty, according to Gorney.29,30
Khansa et al 31 discovered that men were less satisfied with their rhinoplasty results than women and were less specific when describing their unhappiness. One new approach to investigating postoperative cosmetic surgery patient discontent can be found in their social media feeds.
In the present study, a natural look after rhinoplasty was connected to improved patient satisfaction outcomes determined by ROE ratings.
Conclusion
Lower projection ratio (GOODE) and greater nasolabial angle values were connected ROE ratings for patient satisfaction following rhinoplasty32,33 of the tip. Despite the lack of statistical significance, it is hypothesized that the TCCS group’s reduced tip projection results may be linked to higher patient satisfaction due to their more realistic look.
Footnotes
Acknowledgements
None.
Author Contributions
Sameer Ali Bafaqeeh: Planning, designing, literature survey, active intellectual support. Nuray Bayar Muluk: Planning, designing, literature survey, statistical analysis, writing, active intellectual support, submission. Zeynel Öztürk: Planning, designing, literature survey, active intellectual support. Oğuzhan Oğuz: Planning, designing, literature survey, active intellectual support. Halil İbrahim Altiner: Planning, designing, literature survey, active intellectual support. Cemal Cingi: Planning, designing, literature survey, data collection, active intellectual support, English editing.
Availability of Data and Materials
All data for this study are presented in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Committee Approval
Ethics committee approval was taken from T.R. Bilecik Şeyh Edebali University, Non-Invasive Clinical Research Ethics Committee (Date: 05.12.2023, Number: 8/4).
Informed Consent
There is no need for informed consent because the data were evaluated retrospectively.