
Abstract
A 48-year-old man diagnosed with rheumatoid arthritis was treated with methotrexate for 10 years. He presented left tonsil ulceration and ipsilateral cervical lymphadenopathy. A tonsillar biopsy revealed tuberculosis. The patient received antituberculous therapy for 8 months with a positive response. However, after resumption of methotrexate due to worsening rheumatoid arthritis, symptoms recurred. The patient initiated antituberculous therapy once more for 6 months, and methotrexate was stopped. At regular follow-up, the patient showed a positive clinical response with resolution of tonsillar ulceration and lymphadenopathy after 14 months of antituberculosis treatment.
Introduction
Tuberculosis is a highly contagious infectious disease caused by Mycobacterium tubercular bacilli and is one of the main causes of morbidity and mortality worldwide.
The disease mainly affects the lungs. Extrapulmonary infection accounts for only 10% to 15% of all tuberculosis cases and may occur especially in lymph nodes. 1 Oral cavity tuberculosis is a rare medical condition that can be primary or secondary. 2 It rarely occurs in tonsils due to the antiseptic effect of saliva and the presence of saprophytes in the oral cavity, which is protected by a thick layer of squamous cells. Primary tonsillar tuberculosis, a rare entity, accounts for 0.5% of all tuberculosis cases. Lesions usually appear as a single ulceration that can mimic a malignant neoplasm. Immunocompromised patients are the most vulnerable to this disease, especially those who received immunosuppressive drugs.3,4 The risk of tuberculosis appears to be higher in patients receiving Tumor necrosis factor (TNF) inhibitors than in those receiving methotrexate.
In this article, we report a rare case of primary oropharyngeal tuberculosis associated with lymph node involvement in a male patient treated with methotrexate.
Case Report
A 48-year-old male presented to our ENT department with a 2 week history of initial left odynophagia, dysphagia, fever (38°C), and then cervical swelling. There was no history of asthenia, anorexia, or weight loss; however, he had a history of night sweats.
He had no relevant personal or family history of tuberculosis and had received a correct Bacillus Calmette–Guérin (BCG) vaccination at a young age. He was a nonsmoker and did not consume alcohol.
The patient had rheumatoid arthritis for 18 years and had been treated with oral methotrexate (7.5 mg per week) for the past 10 years.
Physical examination revealed unilateral hypertrophy of the left palatine tonsil, with a large ulcer covered with a whitish coating at its upper pole (Figure 1). On palpation, the tonsil was hard and infiltrated with minimal bleeding. There was no trismus. A tender left cervical lymphadenopathy (levels II and III) was also found.
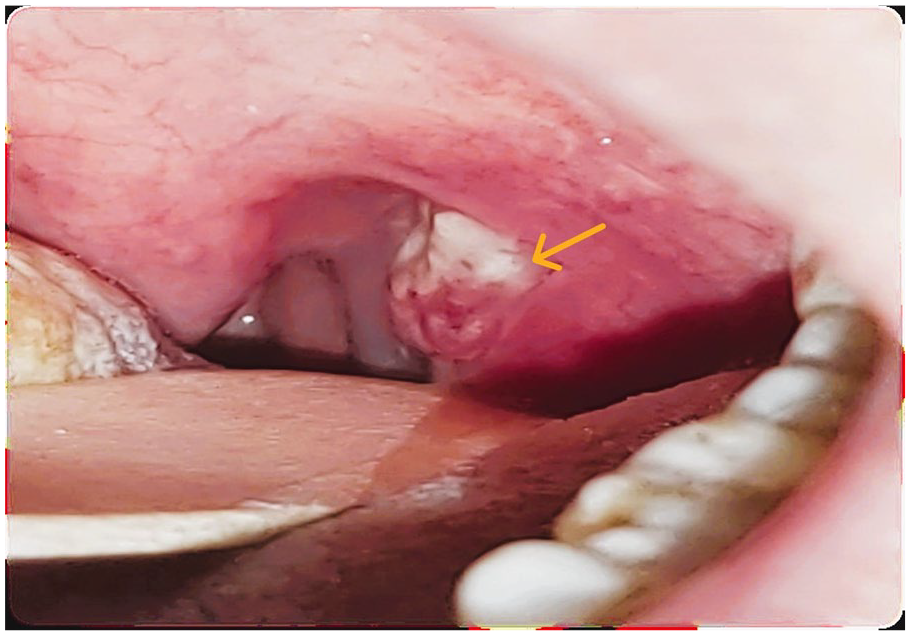
The initial clinical presentation: enlarged and ulcerated left tonsil.
He was previously treated with several broad-spectrum antibiotics (amoxicillin-clavulanic acid, gentamicin, metronidazole) and oral analgesics for 8 days without improvement.
The patient was afebrile and had a normal performance status. The rest of the physical examination, including nasal endoscopy, did not reveal any other abnormal findings.
Therefore, the patient was admitted for further medical investigations. The patient’s blood cell count and chemistry were within normal range.
Cervical computed tomography (CT) scan showed hypertrophy of the left tonsil and surrounding tissues, suggesting peritonsillar abscess.
There were multiple ipsilateral lymphadenopathies with contrast-enhancing areas of liquified hypodensity (Figure 2). Histology of lymph node aspiration revealed nonspecific necrosis.
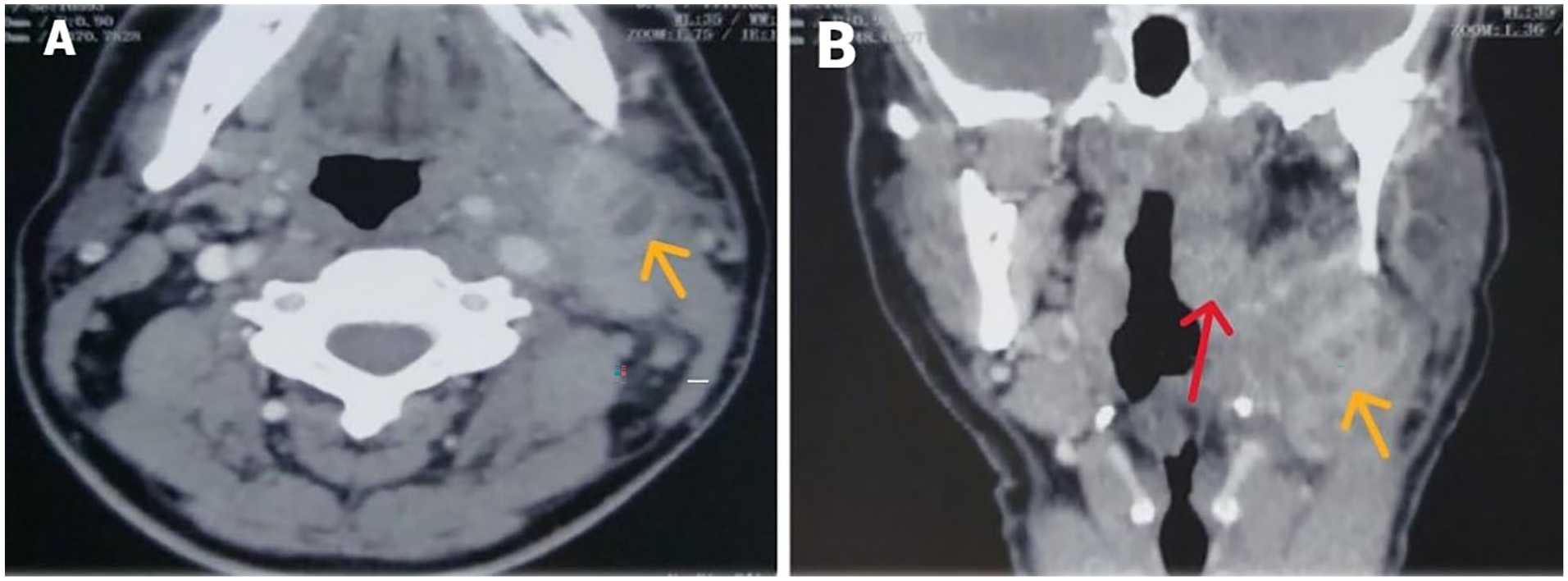
CT scan images in axial and coronal sections showing adenopathies in the left carotid sheath with central necrosis (A), left peritonsillar abscess (red arrow) with a group of adenopathies within the III level (yellow arrow), the largest one measuring 45 mm × 28 mm (B). CT< computed tomography.
A left tonsil biopsy was also performed. Histological examination of biopsied tissue revealed a granulomatous inflammatory process with necrosis suggestive of tuberculosis (Figure 3).
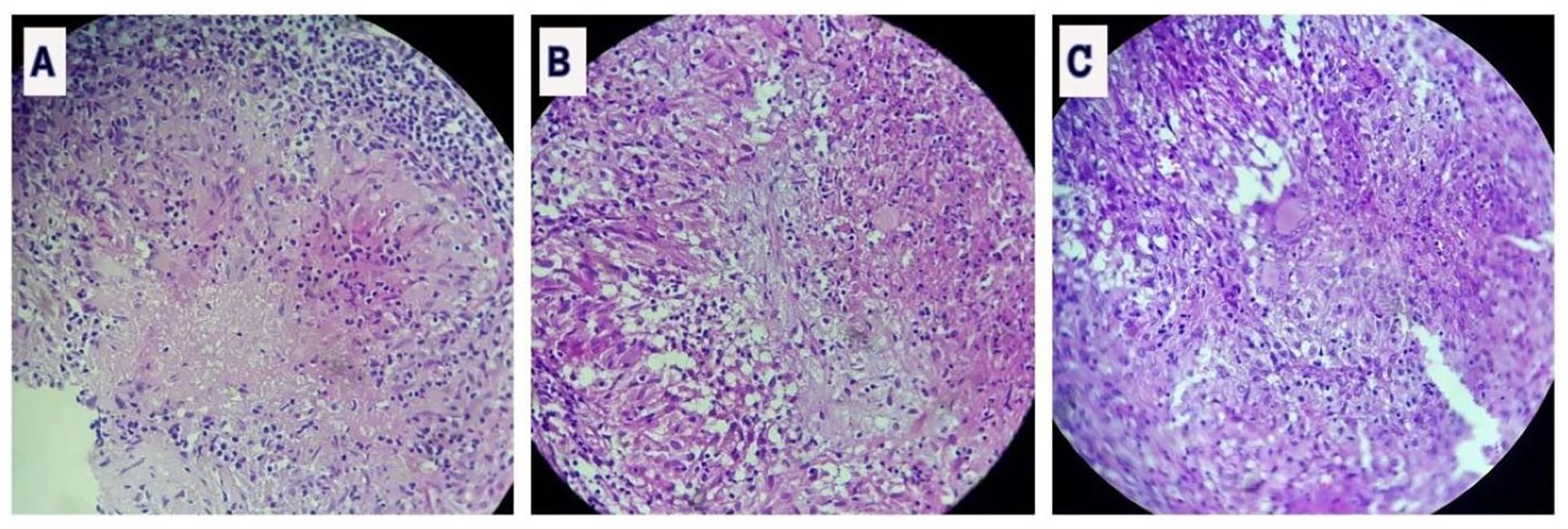
Microphotograph of histopathological examination of the specimen showing in (A) epithelioid cell granulomas with caseous necrosis, in (B) well-defined epithelioid granulomas, and in (C) epithelioid granulomas made of epithelioid cells, lymphocytes, and Langhans-type of giant cells.
The acid-fast bacillus sputum smear was negative and the chest radiograph was unremarkable.
Based on these histopathological results, methotrexate was discontinued. Subsequently, the patient was started on antituberculous therapy with isoniazid (300 mg daily), rifampicin (600 mg daily), ethambutol (1100 mg daily), and pyrazinamide (1200 mg daily) for 2 months, followed by a 2-drug regimen of rifampicin and isoniazid, (at the same dose) for the next 6 months.
The tonsillar ulcer gradually healed and the cervical lymphadenopathy decreased in size.
After 8 months of antituberculous therapy, methotrexate was reintroduced due to worsening rheumatoid arthritis, leading to a relapse of tuberculosis along with left tonsillar enlargement and tender cervical swelling.
A CT scan revealed multiple lymphadenopathies with collections that lead to a cervicotomy. The intraoperative aspect was evocative of tuberculosis: an accidental rupture of the capsule released a purulent liquid with the caseum. Samples were taken for tuberculosis Polymerase Chain Reaction (PCR), which yielded positive results.
Histopathological examination of the operative specimen revealed no evidence of malignancy.
The patient underwent another 6 month course of antituberculous therapy and methotrexate was interrupted.
Rheumatoid disease was managed with courses of corticosteroid and anti-inflammatory drugs during exacerbations.
After an 18 month follow-up, the patient was asymptomatic with complete resolution of oral cavity lesions and associated cervical lymphadenopathy.
Discussion
Primary oropharyngeal tuberculosis is a rare condition that accounts for 0.05% to 5% of all tuberculosis cases, often originating in the tonsils or soft palate.2,4
The disease can result from direct Mycobacterium inoculation via infected sputum or inhaled droplets. Literature suggests possible bloodstream seeding of the tonsils with mycobacteria.5,6
It may be either primary or, most commonly, secondary. According to this point, primary tuberculosis usually occurs in younger patients, whereas secondary tuberculosis is seen mostly in the elderly, particularly when health status declines with immunodeficiency and frequently simulates tonsillar malignancy.
In addition, immunodeficiency exacerbates tuberculosis occurrence and recurrence. 6
Cases of oral tuberculosis in rheumatoid arthritis patients treated with TNF inhibitors and methotrexate have been documented. However, the use of a methotrexate-based monotherapy drug has not been associated with oral tuberculosis. 7
Our case involved a patient with primary oral tuberculosis under methotrexate treatment for 10 years.
Methotrexate is a biological agent known to be an antimetabolite and antirheumatic agent that has an immunosuppressive role in some immune-mediated diseases (rheumatoid arthritis and psoriasis) and acts in addition as a chemotherapy agent used to treat certain types of cancers such as non-Hodgkin lymphoma, acute lymphoblastic leukemia.7,8
The use of anti-TNF factors alone or in association with methotrexate has been revolutionary in the treatment of rheumatoid arthritis, and despite the required pretreatment screening, it is also associated, even at lower doses, with a higher risk of developing active tuberculosis. 9
Diagnosis of tuberculosis post-TNF inhibitor use typically occurs within a relatively short period, ranging between 3 months to 6 years.
However, as in our case, oral tuberculosis can occur after years of methotrexate treatment.
Screening for latent tuberculosis using a pretreatment test should be considered in all patients receiving anti-TNF inhibitors.7,10,11
Based on our case, we believe that the risk of tuberculosis in patients receiving methotrexate therapy is not negligible despite lower doses, especially in the endemic region. Therefore, annual tuberculosis testing is crucial for high-risk patients.
According to the literature, the most common symptom was sore throat. Odynophagia and hoarseness of voice were also reported, usually in association with recurrent or chronic tonsillitis. Since tonsillar tuberculosis is a challenging diagnosis, a differential diagnosis should be made and includes mainly malignancy, traumatic ulcer, aphthous ulcer, and lymphoreticular malignancies.4,5
Therefore, a histopathological examination of tonsil samples is necessary to confirm diagnosis, 11 as was the case for our patient who presented with suggestive signs of malignancy: tonsillar ulceration and ipsilateral lymphadenopathy.
As reported in scientific studies, tonsillar tuberculosis can be effectively treated with a 2 month regimen of rifampicin, isoniazid, pyrazinamide, and ethambutol, followed by 4 months of rifampicin and isoniazid without complications.12-14 Our patient was treated for 14 months with antitubercular therapy due to lymph node involvement.
Conclusions
Tuberculosis of the tonsil with lymph node involvement, in the absence of pulmonary tuberculosis, is an uncommon form of extrapulmonary tuberculosis. It is more commonly seen in immunosuppressed patients.
Histopathological examination plays an important role in the diagnostic process, as it can be challenging. Early diagnosis and treatment are essential for reducing morbidity and mortality.
Footnotes
Acknowledgements
No acknowledgments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case was obtained from the Ethics Committee of Sidi Bouzid Hospital (Approval NO. 73), on November 12, 2023.
Statement of Informed Consent
Written informed consent was obtained from the patient for his anonymized information to be published in this article.