
Abstract
Objective
To analyze the characteristics of invasive lobular carcinoma (ILC) compared with invasive ductal carcinoma (IDC) and to investigate the impact of histology on axillary lymph node (ALN) involvement in luminal A subtype tumors.
Methods
We retrospectively analyzed patients diagnosed with ILC or IDC from 2012 to 2016 who underwent surgery. Patients constituted 493 primary early breast cancer cases (82 ILC; 411 IDC).
Results
Compared with IDC, ILC tumors were significantly more likely to be grade 2, estrogen receptor- (ER) positive (+), have a lower proliferation rate (Ki67 <14%), and a higher pathological T stage (pT2–4). The luminal A subtype was significantly more common in ILC compared with IDC. In a multivariate regression model, grade 2, ER+, progesterone receptor-positive, pT2, and pT3 were significantly associated with ILC. Additionally, with the luminal A subtype, ALN involvement (pathological node stage (pN)1–3) was significantly more frequent with ILC versus IDC.
Conclusions
Our data suggest that grade 2, positive hormone receptor status, and higher pathological T stage are associated with ILC. With the luminal A subtype, ALN involvement was more frequent with ILC versus IDC.
Keywords
Introduction
Invasive lobular carcinoma (ILC) and invasive ductal carcinoma (IDC) represent the two most common histologic types of invasive breast cancer (BC). After IDC, which constitutes 72% to 80% of cases, ILC accounts for up to 15% of all BC cases.1–3 Loss of E-cadherin, a transmembrane protein mediating cell–cell adhesion, is responsible for the characteristic discohesive growth pattern of ILC.2,4 Compared with IDC, ILC is associated with older age at diagnosis and larger tumor size. Typically, ILC displays features associated with a good prognosis; this type is frequently characterized by low to intermediate histological grade, positive hormone receptor status, and negative expression of human epidermal growth factor receptor 2 (HER2). However, there is a tendency for late recurrences, and a higher rate of multiple metastases with a distinct pattern of involvement of distant sites.1,2,4–16 ILC is more frequently multifocal and bilateral compared with IDC, and it is difficult to define margins, clinically, and to detect it mammographically. Furthermore, the features of ILC are more difficult to define intraoperatively; therefore, mastectomy is performed more frequently than lumpectomy.5,7,8,10,13,16–22 Positive axillary lymph node (ALN) involvement represents one of the most important prognostic factors for patients with primary BC.23–26 However, data describing ALN status in ILC compared with IDC are controversial.1,6,7,10,13,14
Genetic subtypes of BC with distinct prognoses have been identified by gene expression profiling.27,28 Clinically, the combination of hormone receptor (estrogen receptor (ER), progesterone receptor (PR)) expression, HER2 status, and Ki67 by immunohistochemistry is used to define different BC subtypes as luminal A, luminal B, HER2, and triple-negative.29–32 ILC is predominantly classified as luminal A according to genetic profiling and immunohistochemistry; IDC shows a greater diversity of intrinsic subtypes.33,34
In this retrospective study, we aimed to characterize ILC compared with IDC regarding the histopathological and prognostic features (tumor grade, hormone receptor and HER2 status, Ki67, immunohistochemically-defined subtype, pathological T stage (pT), and ALN involvement). Additionally, in the luminal A subgroup, we evaluated lymph node involvement as an important prognostic factor for patients with BC.
Patients and methods
Study population
We retrospectively analyzed consecutive patients with primary ILC or IDC early BC diagnosed between 2012 and 2016 who underwent surgery. All patients were treated at the Department of Obstetrics and Gynecology at Vienna General Hospital. Early BC was defined as disease without distant metastasis. Lobular carcinoma was routinely determined by experienced pathologists according to morphology in hematoxylin & eosin (H&E)-stained slides. In addition, immunohistochemical staining for E-cadherin was performed to diagnose ILC. Women with mixed IDC/ILC, metastatic disease at the time of diagnosis, history of previous cancer, or previously treated with neoadjuvant chemotherapy were excluded from the analysis. Bilateral BC was diagnosed in eight patients. Clinicopathological data constituted age at diagnosis, tumor morphology, tumor grade; ER, PR, and HER2 status; Ki67, pT stage, and pathological node (pN) stage. Both ILC and IDC were routinely graded by experienced pathologists according to the grading system of Elston and Ellis. 35
Immunohistochemical/fluorescence in situ hybridization analysis for ER, PR, HER2, and Ki67
Immunohistochemical assessment of ER, PR, HER2, and Ki67 was performed using the Ventana BenchMark Ultra system (Ventana Medical Systems Inc., Tucson, AZ, USA). The following antibodies were used for staining: clone SP1 against ER, clone 1E2 against PR, clone 4B5 against HER2, and clone 30-9 against Ki67 (Ventana Medical Systems Inc.).
ER and PR status were considered positive if ≥1% of the tumor nuclei stained, according to the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guideline. 36 HER2-positivity was defined as staining of >10% of the tumor cells as proposed by the updated ASCO/CAP clinical practice guideline. HER2 staining also needed to be strong and circumferentially membranous. In cases of HER2 immunohistochemistry (IHC) 2+, we performed fluorescence in situ hybridization (FISH). 37 According to Cheang et al., Ki67 <14% was considered a low proliferation rate, and Ki67 ≥14% was considered a high proliferation rate. 31
Breast cancer subtypes according to IHC and FISH analysis
ER, PR, HER2, and Ki67 results were used to create BC subtypes, which we defined as: luminal A (ER+ and/or PR+, HER2−, low Ki67); luminal B/HER2-negative (ER+ and/or PR+, HER2−, high Ki67); luminal B/HER2-positive (ER+ and/or PR+, HER2+, low or high Ki67); HER2-positive (ER−, PR−, HER2+); and triple-negative (ER−, PR−, HER2−). 38
Statistical analysis
Descriptive statistics were performed to determine the characteristics of the two histopathological groups (ILC and IDC). Additionally, we compared the pN stage in luminal A subtype tumors in both groups. The Chi-square and Fisher’s exact (for smaller sample sizes) tests were used to investigate the proportions of the clinicohistopathological characteristics between ILC and IDC. Logistic regression was performed to identify independent parameters associated with ILC and IDC. Associations were summarized using odds ratios (OR) and corresponding 95% confidence intervals (CI) derived from the model estimates. We excluded all unknown/undetermined values from the analysis. Statistical significance was considered at p<0.05 (two-tailed), and we performed all statistical analyses using the statistical software package R version 3.4.1 (www.r-project.org).
Ethics approval and consent to participate
This study was approved by the ethics committee of the Medical University of Vienna (2035/2018). All procedures performed in our study were in accordance with the ethical standards of the institutional ethics committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. According to the ethics committee of the Medical University of Vienna, written informed consent was not required owing to the retrospective design of this study.
Results
Of 485 consecutive patients with primary ILC or IDC early BC, we analyzed 493 BC cases; 82 (16.6%) ILCs were compared with 411 (83.4%) IDCs. The clinicopathological characteristics of the patients are presented in Table 1. The mean age at diagnosis in the total population was 59.1 years (range: 28–92 years, standard deviation (SD): 12.7 years). We found no significant difference in the distributions of age at diagnosis between ILC and IDC. The luminal B subtype was identifed in 50.0% of ILCs and in 50.9% of IDCs.
Characteristics of the patients and tumors

*ILC vs IDC, chi-square or Fisher’s exact test; unknown/undetermined values were excluded from the analysis
BC, breast cancer; ER, estrogen receptor; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; HER2, human epidermal growth factor receptor 2; pN, pathological node stage; pT, pathological T stage; PR, progesterone receptor; SD, standard deviation
The results of the H&E and IHC staining of ILC and IDC are shown in Figure 1. Tumor grade was significantly different between ILC and IDC (p<0.001), and grade 2 was more common among ILCs (80.5%) compared with IDCs (44.3%). ER-positive status was found in 98.8% of ILCs versus 86.6% of IDCs (p<0.01), and PR-positive status was found in 82.9% of ILCs and in 73.0% of IDCs, with a marginally significant difference (p=0.05). Regarding HER2, there was no significant difference between the groups. We found a lower proliferation rate (Ki67 <14%) more frequently in ILC (48.8%) compared with IDC (35.8%) (p=0.03). The pT distribution differed significantly between ILC and IDC (p=0.01); ILC was more often diagnosed at a higher pT stage (pT2–4) (46.3%) compared with IDC (28.3%). The proportion of pN-positive status (pN1–3) did not differ significantly (ILC: 34.1%, IDC: 28.5%).

Morphology and immunohistochemical phenotypes of invasive lobular carcinoma (ILC)
In the total population, luminal A, luminal B, HER2-positive, and triple-negative subtypes accounted for 36.7%, 50.7%, 4.1%, and 8.3%, respectively; one tumor (0.2%) was unassigned. Compared with IDCs, ILCs were significantly more likely to be luminal A (34.5% versus 47.6%, respectively) (p=0.004) (Figure 2).

Distributions of breast cancer subtypes in ILC and IDC (comparison: p=0.004) (luminal A: ER+ and/or PR+, HER2−, low Ki67; luminal B/HER2−: ER+ and/or PR+, HER2−, high Ki67; luminal B/HER2+: ER+ and/or PR+, HER2+, low or high Ki67; HER2+: ER−, PR−, HER2+; and triple-negative: ER−, PR−, HER2−).
In a univariate analysis of the clinicopathological factors associated with ILC versus IDC, tumor grade, ER and PR status, proliferation rate (Ki67), and the pT stage were predictor variables. However, when these features were entered into a multivariate regression model and adjusted for age, only grade 2 (OR: 6.88; 95% CI: 2.68–17.68; p<0.001), ER+ (OR: 11.99; 95% CI: 1.62–88.42; p=0.015), PR+ (OR: 2.09; 95% CI: 1.08–4.05; p=0.028), pT2 (OR: 2.18; 95% CI: 1.29–3.70; p=0.004), and pT3 (OR: 3.57; 95% CI: 1.25–10.18; p=0.017) were associated with ILC (Table 2).
Logistic regression analysis of ILC versus IDC: univariate and multivariate analysis

*adjusted for age at diagnosis
BC, breast cancer; CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; LR, logistic regression; OR, odds ratio; PR, progesterone receptor; pN, pathological node stage; pT, pathological tumor stage
Among luminal A tumors, pN0 was found in most of the cases (76.8%). Compared with the IDC group, significantly more ILCs presented with positive ALN involvement (pN1–3) (16.9% versus 30.8%, respectively) (p=0.04) (Table 3, Figure 3).
Pathological node stage in luminal A tumors
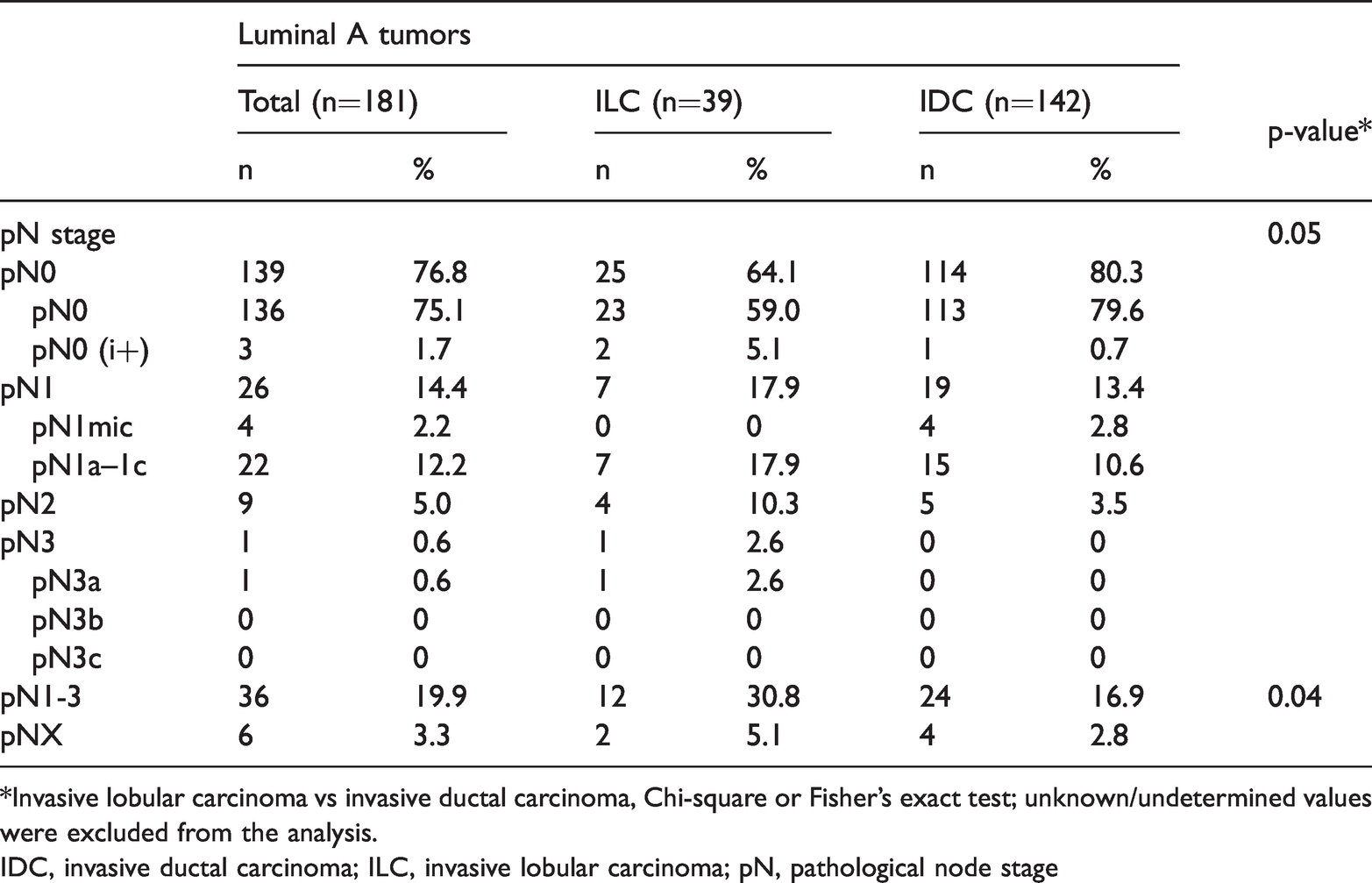
*Invasive lobular carcinoma vs invasive ductal carcinoma, Chi-square or Fisher’s exact test; unknown/undetermined values were excluded from the analysis.
IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; pN, pathological node stage
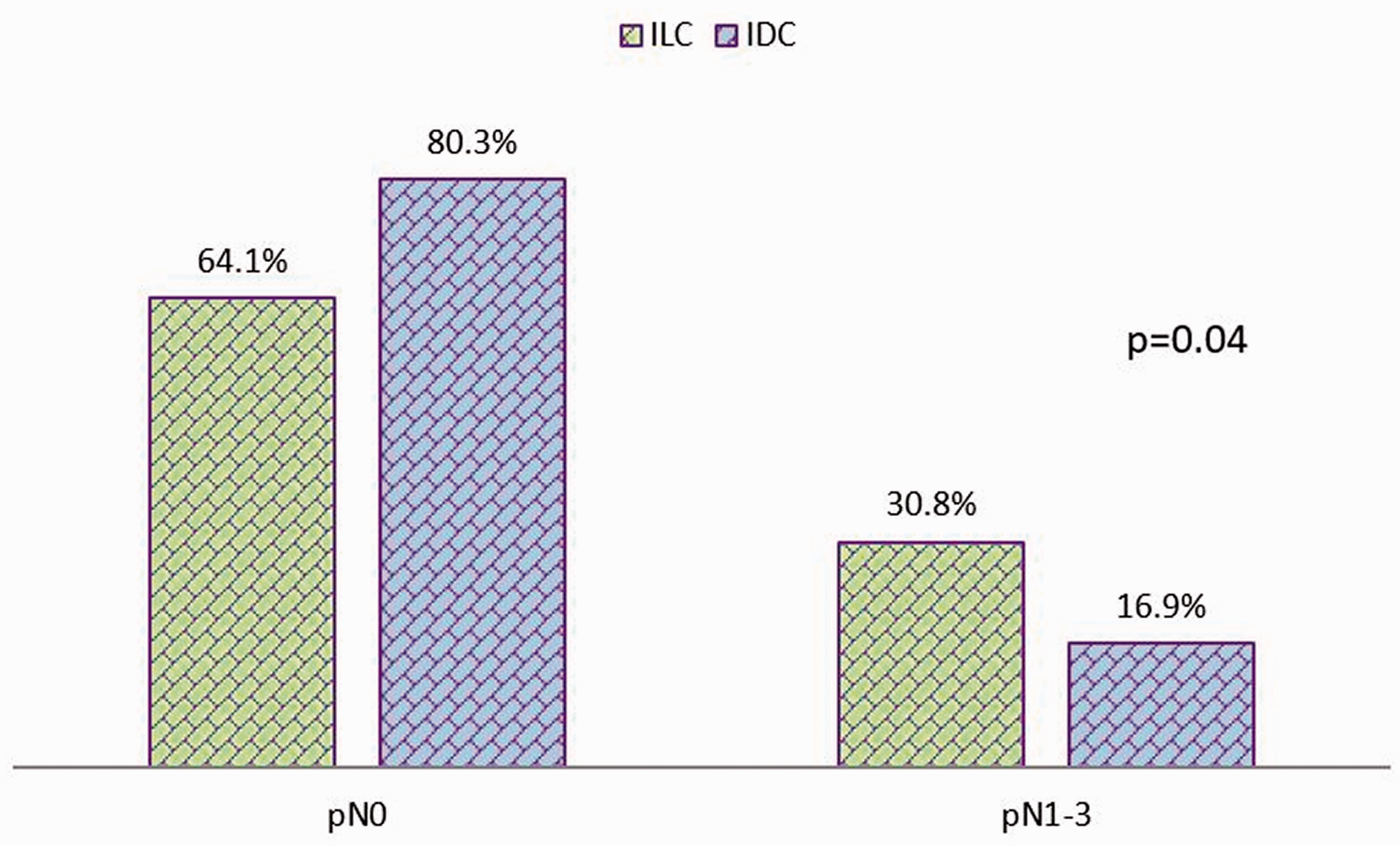
Axillary lymph node (ALN) involvement in the same immunohistochemically-defined luminal A subset of patients
Discussion
Our results showed that intermediate tumor grade, positive hormone receptor status, and larger tumor size were associated with ILC. A lower proliferation rate (Ki67) was found more frequently with ILC (48.8%) compared with IDC (35.8%) (p=0.03), and the subtype distributions differed significantly between both histological groups: luminal A was significantly more common with ILC (47.6%) compared with IDC (34.5%) (p=0.004). We found no significant difference regarding ALN involvement between ILC and IDC. However, in the patients with the luminal A subtype, we found an association between positive nodal status and ILC.
Our analysis showed that age at diagnosis did not differ significantly between patients with ILC or IDC. This has been reported previously in several studies;17,18,21,39,40 however, ILC was associated with older age at diagnosis.7,9,13,14,34,41–43 According to our findings, lower tumor grade in ILC was observed in different studies comparing these tumors with IDC.8,9,13,14,34,40,41 Our results showed that ILC was associated with a larger tumor size, as seen in several previous trials.1,7–10,13–15,17,34,40,41 In contrast, some studies reported no difference in tumor size between ILC and IDC.18,21,39,42
As in our study, positive ER status was found more frequently with ILC in several trials.10,13,21,39 Additionally, ILC was associated with a higher rate of hormone receptor (HR)-positivity.7,9,40,41,44 In contrast, more ER-negative tumors were observed with ILC than with grade-matched IDC in a British trial comparing both histologic groups. 1 Our analysis showed that HER2 expression did not differ significantly between ILC and IDC; however, reports of more HER2-negative tumors with ILC exist,7,40,41,44 and several studies revealed that ILC was more often slowly proliferative;7,40,44 our results were similar.
In this study, we demonstrated a significantly different distribution in BC subtypes between both histological groups. In ILC tumors, the luminal A, luminal B, HER2-positive, and triple-negative subtypes accounted for 47.6%, 50.0%, 1.2%, and 0%, respectively. In 1.2% of ILCs, the subtype was unknown. Iorfida et al. evaluated ILC regarding its biological features. 45 According to IHC reactivity, approximately half of all ILCs were classified as luminal B (48.5%). Luminal A, HER2-positive, and triple-negative subtypes accounted for 34.9%, 0.4%, and 1.5%, respectively; the status of 14.7% of the ILCs could not be determined. 45
In a Belgian study, ER, PR, and HER2 status were used to define different subtypes. 14 ILCs were more frequently ER+/PR+/HER2− (85.3%) compared with non-ILCs (67.0%). The HER2-positive and triple-negative subtypes were very rare among ILCs (0.7% and 1.3%, respectively) relative to non-ILCs (4.9% and 11.2%, respectively) (p<0.001). 14 Williams et al. investigated cases of ILC and IDC from the Carolina Breast Cancer Study (CBCS) and The Cancer Genome Atlas project (TCGA). Subtypes were analyzed according to differences in gene expression patterns (ribonucleic acid (RNA)-based intrinsic subtypes) and immunohistochemically. Only ER, PR, and HER2 were used to create IHC-based subtypes: luminal A (ER+ and/or PR+, HER2−); luminal B (ER+ and/or PR+, HER2+); HER2-positive (ER−, PR−, HER2+); and triple-negative (ER−, PR−, HER2−). According to IHC, the majority of ILCs and IDCs were classified as luminal A (CBCS: 89% and 58%, TCGA: 86% and 55%, respectively). Luminal B accounted for 6% (CBCS)/9% (TCGA) of ILCs and for 10% (CBCS)/18% (TCGA) of IDCs. 34 In our study, the majority of patients were classified as luminal B (ILC: 50.0%, IDC: 50.9%) suggesting that using Ki67 for subtype definition increases the detection of luminal B tumors.
Our findings showed an association between positive pN status and ILC in luminal A tumors. Published data describing ALN status in ILC compared with IDC are controversial. Most studies demonstrated that ALN involvement did not differ between ILC and IDC.5,7,9,13,20,21,39,40,42,43,46 However, some studies showed an association between ILC and a higher incidence of positive ALN involvement.1,10,15,41 In contrast, other studies have reported less frequent ALN positivity in ILC.6,14
It is important to note that the patients in our study were very homogenous. This was a monocentric study, all patients underwent surgery, and patients with recurrent disease or primary metastatic disease were excluded.
The limitations of this study are the retrospective design and the small sample size; however, despite the small sample size, our results were similar to previously published data. Further studies with larger sample sizes are warranted. Categorizing BC subtypes using both IHC and gene expression profiling should be performed in future studies. Finally, we did not differentiate between the histological subtypes of ILC tumors (e.g. classic, solid, alveolar).
In conclusion, our results showed that grade 2, positive hormone receptor status, and higher pT stage (pT2–3) were associated with ILC. With the luminal A subtype, ALN involvement was more frequent with ILC versus IDC.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
SD, CP, and CFS contributed to study conception and design. SD, KT, and CFS provided the findings and contributed to the literature search. SD, NH, MI, JM, and CT contributed to collecting and assembling the data. All authors contributed to data analysis and interpretation. SD, CP, and CFS contributed to writing the manuscript. All authors reviewed and approved the manuscript.