
Abstract
Introduction
Tinnitus, characterized by the subjective perception of sound in the absence of external acoustic stimuli, affects a global population exceeding 600 million individuals. 1 In Asia, the prevalence of tinnitus among adults aged 20 to 54 years ranges from 16.0% to 20.5%. 2 Individuals afflicted with tinnitus are at an elevated risk for developing various comorbid conditions, including insomnia, anxiety, and depression, ultimately leading to a diminished quality of life when compared to the general population.
Despite the high prevalence of tinnitus, only approximately one-quarter of individuals affected seek medical assistance for tinnitus-related symptoms. 3 This study categorizes tinnitus into 2 distinct types: asymptomatic tinnitus (AT) and symptomatic tinnitus (ST), based on the presence of associated symptoms such as insomnia, concentration difficulties, and emotional, psychosomatic, and interpersonal issues. The term “AT” denotes a perceived sound without accompanying severe tinnitus-related symptoms warranting treatment, while “ST” signifies both a subjectively perceived sound and the presence of tinnitus-related symptoms necessitating specialist intervention. Among these symptoms, psychosomatic issues can significantly diminish individuals’ quality of life. 4 Research has shown that the severity of tinnitus exhibits a negligible correlation with audiometric parameters, in contrast to psychological distress, including anxiety and depression, which are stress-related factors. 5
The reasons why some show tinnitus-related symptoms but others do not, remain controversial. Stress is an organism’s response to environmental assaults. Long-time exposure to abnormally high-level stress may lead to a pathological status, sometimes mentally. 6 Chronic stressful life events are significant environmental factors that substantially affect the development of depression and anxiety disorders. 7 Extreme or prolonged exposure to stress often disrupts the individual’s physiological and psychological functioning, leading to a variety of mood- and psychiatry-related disorders. 8
It is a challenge to measure stress and its effect on an individual’s health. We analyzed the association between stress and tinnitus-related symptoms by focusing on major stressful life events, which are easier to quantify using a questionnaire based on the Social Readjustment Rating Scale (SRRS). Instead of the degree of stress, we quantified the number of stressful events that is a subjective index.
Tinnitus is not a disease, but a symptom. Hiller et al held that some tinnitus symptoms could be categorized as somatic symptoms. In recent years, psychosomatic researches have yielded lots of findings indicating the important role of stress in tinnitus development. 9 The purpose of this study was to investigate the relationship between stress and ST.
Methods
Participants and Procedure
This study enrolled 183 participants who had visited the clinic between April 2020 and April 2023. Participants’ demographic information was collected with a case report form, covering gender, age, body mass index (BMI), degree of education, marital status, noise exposure history, and vascular risk factors, including history of smoking, drinking, diabetes mellitus, hypertension, and hyperlipidemia. Inclusion criteria were as follows: (1) patients who had tinnitus symptoms lasting more than 3 months; (2) able and willing to give written informed consent and comply with the requirements of the study protocol. The exclusion criteria were: (1) with middle or inner ear anomaly; (2) have hypertension, diabetes, and other systemic diseases; (3) with severe psychiatric illness and cognitive impairment.
All participants were assigned to 3 groups: (1) AT group showing a perception of sound without tinnitus-related symptoms and having never sought for professional help; (2) ST group showing not only a perception of sound but also tinnitus-related symptoms and having consulted specialists for help; (3) Control group of healthy participants who had visited the clinic for a physical checkup.
Audiological Examination
Pure-tone audiometry
All patients underwent pure-tone audiometry (PTA) using an audiometer (Astera Conera Denmark) in a soundproof booth with background noise levels below 18 dB. Audiometric thresholds for air and bone conduction were assessed at frequencies of 0.25, 0.5, 1, 2, 3, 4, 6, and 8 kHz. The hearing loss range was described depending on the PTA parameters: low frequency, 125 to 500 Hz; mid frequency, 1 to 3 kHz and high frequency, 4 to 8 kHz.
Distortion-product otoacoustic emissions
The Otoacoustic Emissions (OAE) screener (Otoread Interacoustics Denmark) was used to conduct the distortion-product otoacoustic emissions (DPOAE) measurements. DPOAE are generated using a pair of closely spaced pure-tone frequencies (f1 and f2) presented simultaneously at a level of 55 dB Sound Pressure Level (SPL) for f1 and 65 dB SPL for f2 (with a frequency ratio of f1/f2 = 1.22). DPOAE were deemed present if the signal-to-noise ratio was at least 3 dB. Distortion products were represented on a DP-gram with the f2 frequency on the horizontal axis and the DPOAE amplitude of the 2f1-f2 distortion product (DPOAE level) on the vertical axis. The amplitudes were recorded at frequencies 0.125, 0.75, 1.0, 2.0, 3.0, 4.0, 6.0, and 8.0 kHz. A passing score required obtaining at least 4 out of the 8 observed frequencies.
The pitch and loudness of the tinnitus
The pitch and loudness of tinnitus were assessed through a tinnitus analysis conducted contralateral to the ear experiencing tinnitus in unilateral cases and contralateral to the ear with the most severe tinnitus in bilateral cases. A 1 kHz pure tone was presented contralateral to the (most severe) tinnitus ear at 10 dB above the patient’s threshold in that ear. The frequency of the tone was adjusted to match the perceived pitch of the patient’s tinnitus, and the intensity was adjusted to match the loudness of the tinnitus. Tinnitus loudness was calculated by subtracting the absolute tinnitus loudness from the audiometric threshold at that frequency.
Assessment Instruments
Tinnitus Questionnaire
Tinnitus-related distress was assessed with the Tinnitus Questionnaire (TQ). Tinnitus-related symptoms were assessed by the Chinese version of the Mini TQ, which provides a quick and reliable assessment (with a Cronbach’s alpha of 0.86). 10 The Mini-TQ is an abridged, 12-item version of the TQ.
Tinnitus Handicap Inventory
Tinnitus-related handicap evaluated by the Tinnitus Handicap Inventory (THI) is highly correlated with the severity of tinnitus. 11 Hence, THI was administered to quantify and qualify the severity of tinnitus by evaluating both the emotional burden and degree of daily disruption caused by the condition. 12 This assessment is composed of 25 items with scores ranging from 0 to 100 and categorized into 5 levels: light (0-16), mild (18-36), moderate (38-56), severe (58-76), and catastrophic (78-100).
Social Readjustment Rating Scale
SRRS, a self-administered questionnaire, was selected to assess 43 common stressful life events in the preceding 6 months. 13 In the questionnaire, each event was given a score from 11 to 100, with a total score of 1466 (the sum of “the weighted life change units” that represents the quantity of stress). According to the SRRS protocols, Grade 1 (score <150) reflect low level of stress, Grade 2 (150-299) at a 50% risk of illness in the near future, and Grade 3 (>300) at an 80% risk of developing a stress-related illness. Higher score represents heavier life stress. The stress grade of each individual stress was recorded.
Statistical Analysis
One-way analysis of variance (ANOVA), χ2 test, Student’s t test, Mann-Whitney U test, and Fisher’s exact test were used for the clinical variables and scores of SRRS of all participants. When an ANOVA examined any significant differences between groups, the Bonferroni corrections were used to adjust them for multiple testing. Binary logistic regression was carried out to determine significant risk factors contributing to ST. Adjusted odds ratio (OR) and the corresponding 95% confidence interval (95% CI) for all subjects were calculated. All analyses were performed with SPSS 27.0 (IBM, Chicago, IL, USA). P < .05 was considered statistically significant.
Results
As shown in Table 1, 183 subjects were included in our study: 88 (48.1%, 52 men, 36 women) in ST group, 45 (24.6%, 25 men, 20 women) in AT group, and 50 (27.3%, 28 men, 22 women) in control group. The mean (±SD) SRRS scores were as follows: 110.29 ± 32.91 in AT group, 186.12 ± 79.74 in ST group, and 102.12 ± 21.39 in control group. These results were similar to the findings in other studies. 14 A significant intergroup difference in SRRS score was found (F = 42.591, P < .001). The mean SRRS score in ST group was higher than that in AT and control group, but no difference occurred between AT and control group. Compared to AT group and control group, subjects in ST group had lower BMI and higher current drinking.
Demographic and Clinical Characteristics of the Study Population.
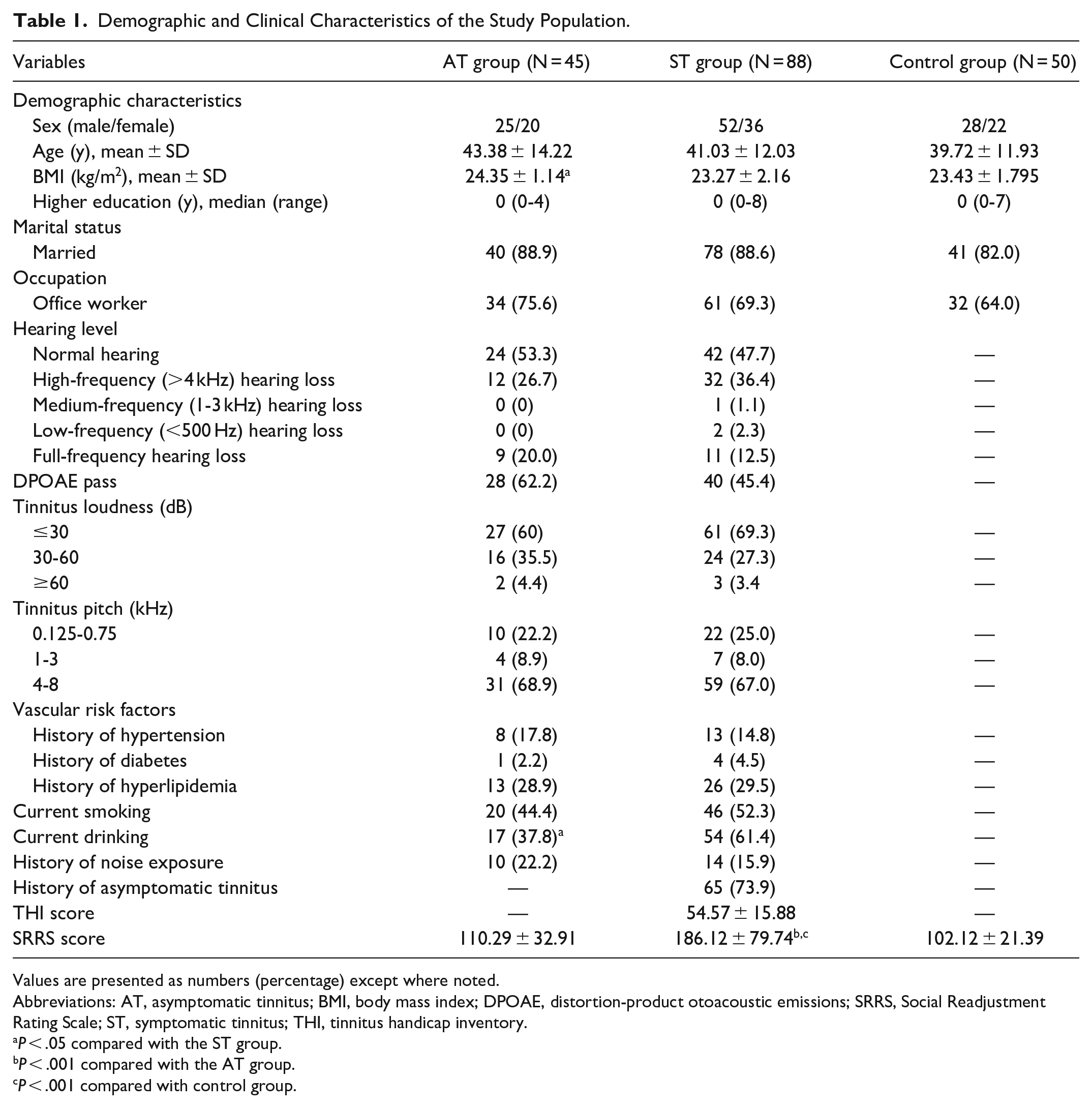
Values are presented as numbers (percentage) except where noted.
Abbreviations: AT, asymptomatic tinnitus; BMI, body mass index; DPOAE, distortion-product otoacoustic emissions; SRRS, Social Readjustment Rating Scale; ST, symptomatic tinnitus; THI, tinnitus handicap inventory.
P < .05 compared with the ST group.
P < .001 compared with the AT group.
P < .001 compared with control group.
Table 2 illustrated a significant correlation between AT and ST group in SRRS score (P < .001). The proportion of subjects with Grade 1 SRRS score in AT group was higher than that in ST group, but in Grade 2 subjects, this proportion was lower (P < .001). There were no values recorded for the AT group in Grade 3. The trend was that the population of lower SRRS scores was mainly in AT group. The proportion of higher SRRS scores in ST group exceeded that in AT group.
SRRS Scores in AT and ST Group.
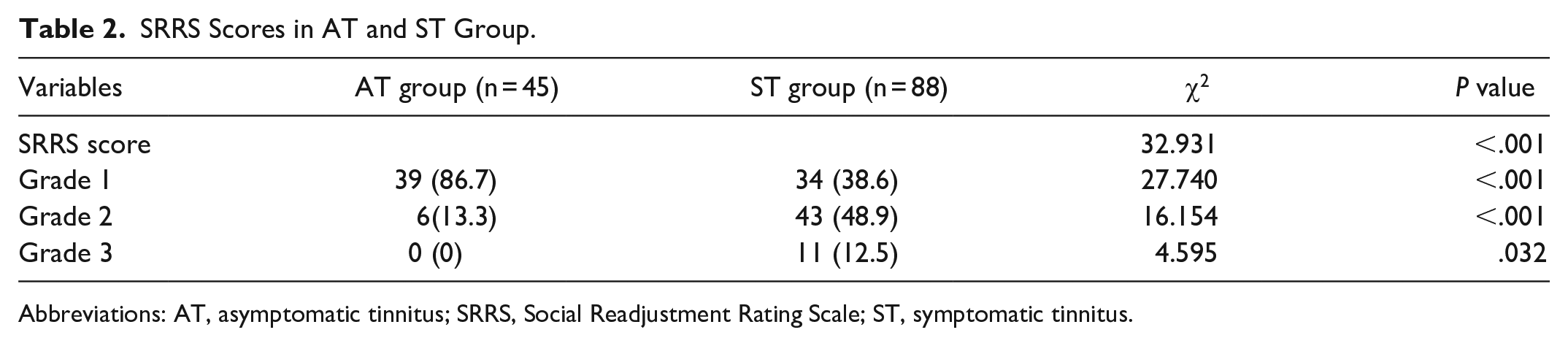
Abbreviations: AT, asymptomatic tinnitus; SRRS, Social Readjustment Rating Scale; ST, symptomatic tinnitus.
Logistic multiple regression analysis was performed in all tinnitus patients. The positive or negative sign of the coefficient B indicates the direction of the relationship between a given independent variable and the dependent variable, while the OR indicates the magnitude of change in the probability of the dependent variable event in case of a 1-unit change in the independent variable. The occurrence of ST was taken as a dependent variable, score in Grade 1 as the reference of SRRS score. As seen in Table 3, Grade 2 score was independently associated with the occurrence of ST (OR 11.921, 95% CI 3.613-39.333, P < .001). Given the absence of Grade 3 score in AT group, no detailed value for 95% CI was presented. Moreover, the BMI was significantly correlated with the occurrence of ST. The effect of current drinking was not significant (P = .141) in the regression analysis.
Multivariate Logistic Model of the Clinical Determinants of ST.
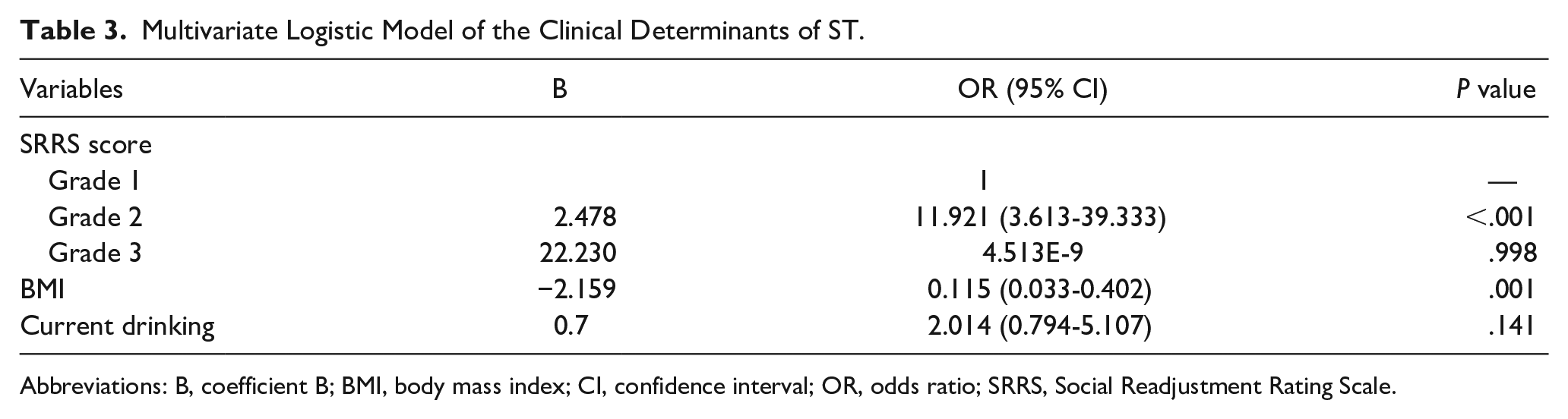
Abbreviations: B, coefficient B; BMI, body mass index; CI, confidence interval; OR, odds ratio; SRRS, Social Readjustment Rating Scale.
As presented in Figure 1, there was a positive correlation between SRRS score and THI score, indicating that the severity of tinnitus was positively associated with stress.
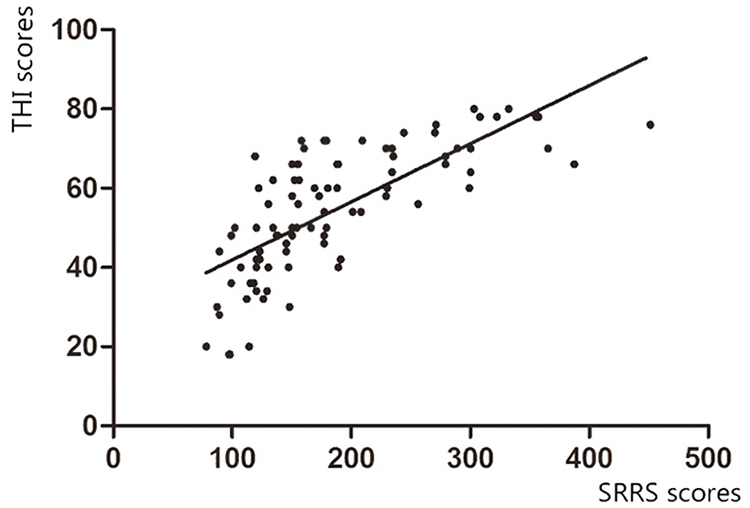
The scatter diagram of the correlation between SRRS scores and THI scores. THI, Tinnitus Handicap Inventory; SRRS, Social Readjustment Rating Scale.
Discussion
To date, the etiology of tinnitus remains unidentified; however, numerous studies have suggested that dysfunction in the auditory system may be a contributing factor. 15 Our research similarly found that individuals in the AT and ST cohorts exhibited hearing impairments of 46.7% and 52.3%, respectively, aligning with prior investigations. 16 The presence of tinnitus-related symptoms was found to detrimentally affect the quality of life for those affected by the condition, with 73.9% of patients in the ST group reporting a history of AT. Individuals may perceive tinnitus, or the sound of AT, as a normal bodily function akin to heartbeat, pulse, breath, and bowel sounds, thereby not experiencing discomfort or seeking medical intervention. Clinical observation suggests that patients with tinnitus may remain asymptomatic in the absence of perceived stress. However, significant levels of stress have the potential to disrupt this equilibrium.
Stress, stemming from either internal or external sources, has the potential to disrupt homeostasis. Organisms can mitigate these disruptions through various mechanisms to maintain physiological stability. However, when stress-induced disturbances surpass a certain threshold, they may result in psychosocial consequences, such as a diverse array of behavioral, somatic, and cognitive symptoms. 17 In addition, alterations in the central nervous system may occur, promoting the development of neural pathways that facilitate adaptation, including heightened arousal, vigilance, and focused attention. In the presence of prolonged and intense stress, individuals may experience neuropsychiatric symptoms, including anxiety and depression, which can render them more vulnerable to adverse life events. Numerous clinical studies suggest that individuals with preexisting mental health conditions exhibit heightened sensitivity to auditory stimuli, such as noise, in comparison to those without such histories. Consequently, tinnitus may be perceived as a disruptive noise rather than a benign sound in individuals experiencing heightened stress levels.
As per the neurophysiological model proposed by Jastreboff, tinnitus frequently elicits heightened levels of annoyance and anxiety as a result of its connection to negative stimuli or ongoing stress. 18 Tinnitus may serve as a warning signal to the brain, triggering symptoms related to anxiety, impaired concentration, sleep disturbances, and various emotional, psychosomatic, and interpersonal challenges when the sympathetic branch of the autonomic nervous system and limbic system become excessively activated. Therefore, if the stimulation continues, a detrimental cycle of stress and the tinnitus may ensue. As illustrated in Figure 1, there is a positive correlation between the intensity of tinnitus and stressful life events. Recent studies have delved into the connections between stress and tinnitus, revealing that the majority of individuals experiencing tinnitus also report varying degrees of stress, ranging from mild to severe. 19 Zirke et al demonstrated a significant relationship between stress levels and the severity of tinnitus. 20 Individuals with tinnitus exhibited heightened stress reactivity and amplified psychological distress, as evidenced by their physiological responses to stress-inducing tasks. 21 Furthermore, research indicated a correlation between stress levels and the severity of tinnitus, as measured objectively by levels of cortisol and other stress-related hormones.
Statistical significance was observed in the relationship between alcohol consumption and stress levels, as well as in the association between BMI and chronic stress. Previous research supports the notion that alcohol consumption can serve as a coping mechanism for stress. Chronic stress has been linked to metabolic disorders, including insulin resistance and obesity, which are closely tied to stress hormones such as corticotropin-releasing hormone and cortisol. The discrepancy between our BMI results and the specified mechanism suggests that the extent and duration of stress experienced by individuals with tinnitus may have influenced the outcomes.
Conclusion
In conclusion, this study investigated the relationship between ST and stress. The results showed that the SRRS scores in the ST group were significantly higher than those in the AT group and the control group. SRRS score (Grade 2) was identified as an independent risk factor for the occurrence of ST, and there was a positive correlation between SRRS scores and THI scores. These findings suggest a close relationship between stress and ST, but further clarification of their relationship is needed through prospective cohort studies.
Methodological Considerations
First, due to the absence of Grade 3 SRRS score in AT group, the width of 95% CI was infinite, and no detailed reference interval was presented. Our relatively small sample size limited the generalizability of our findings. Second, the data from self-report questionnaires might be influenced by method/recall bias. Third, the perceived stress might derive from other events.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Medical Health Science and Technology Project of Zhejiang Province (No. 2024KY1481) and Ningbo Top Medical and Health Research Program (No. 2023030514).
Data Availability Statement
The fully anonymized data that supported the findings of this article are accessible on reasonable request.
Ethical Statement
This study protocol was approved by the Medical Ethics Committee and the Human Research of the Hospital.
Informed Consent
Written informed consent was obtained from all participants.