
Abstract
Significance Statement
Patients with benign vocal fold masses often present with glottic insufficiency, hoarseness, and voice strain. Voice misuse is a common cause of vocal fold masses in professional singers. While voice therapy and treating laryngopharyngeal reflux can be effective, microsurgical excision or laser reduction of the masses may be needed.
Case
This 24-year-old male presented with limited range and associated neck and throat pain that had progressed gradually. He was a pop and rock music singer. He had studied voice but was not taking singing lessons at the time of his first visit. He was diagnosed with reflux laryngitis and started on medications. He was found to have bilateral fluctuating vocal fold paresis, and his stroboscopic examinations showed bilateral anterior vocal fold masses that contributed to his glottic insufficiency and related compensatory muscle tension dysphonia (Figures 1 and 2). He began voice therapy and singing training to improve symptoms, but the dysphonia persisted. He was taken to the operating room to shrink masses with a laser.
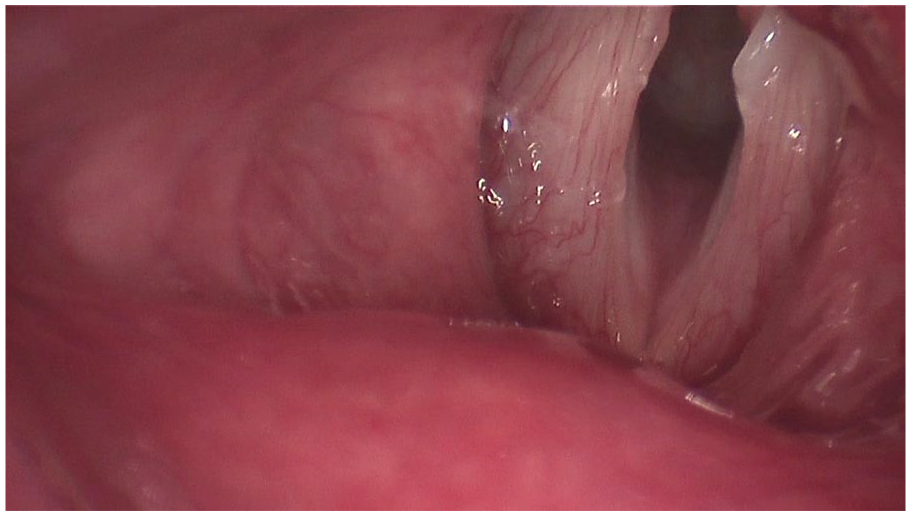
Strobovideolaryngoscopy showing anterior vocal fold masses. There is an apparent posterior lesion on the left, but it is secretion.
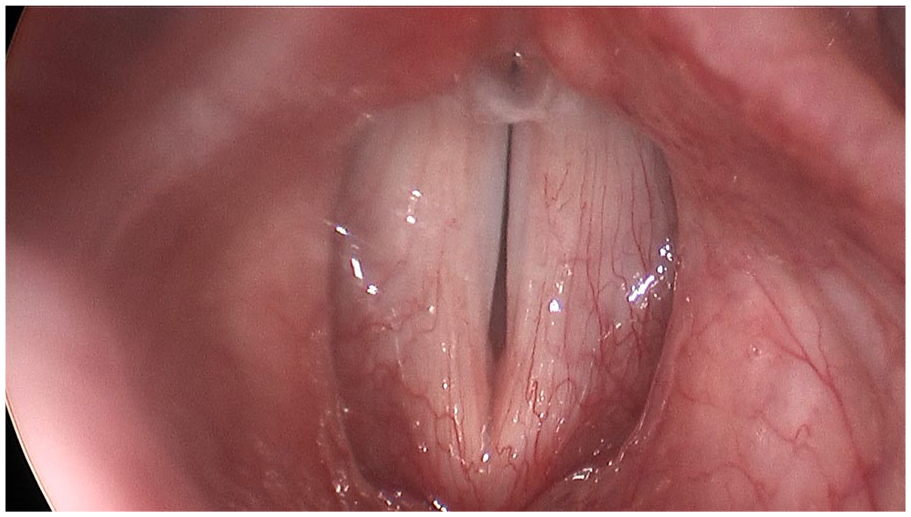
Strobovideolaryngoscopy showing a glottic gap adjacent to the masses.
Discussion
Benign vocal fold masses commonly lead to a disruption in the vibratory properties of the mucosa and to glottic insufficiency due to mass effect. They are usually diagnosed with laryngoscopy, ideally with stroboscopy, and can be classified as vocal fold nodules, polyps, cysts, or other lesions. Patients frequently present with voice strain, fatigue, and hoarseness.1,2 Although vocal fold masses are multifactorial and complex, the common etiology in professional singers is voice overuse and/or misuse. 3 They usually can be prevented by proper voice technique acquired through effect training. The first-line therapy for vocal fold masses is behavioral intervention through voice therapy by a speech-language pathologist or phoniatrist. While some vocal fold masses respond well to voice therapy, others do not show substantial symptomatic improvement. Treating possibly aggravating factors such as laryngopharyngeal reflux also is recommended. Microsurgical excision of masses or other surgical treatment may be needed. Although the senior author almost never uses laser reduction of masses in the striking zone of the vocal fold, it can be safe and effective adjacent to the anterior commissure.1,2
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.