
Abstract

Significance Statement
Primary tumors of the retropharyngeal space are uncommon, and lipomas are particularly rare. Although benign, they may cause significant compression due to their slow growth. Radiology is pivotal in the diagnosis as it provides localization beyond the physical examination.
A 70-year-old male patient was admitted to our clinic with drug intoxication. He had a known history of hypertension, diabetes mellitus, and hypercholesterolemia for 15 years. He had also undergone bypass surgery 8 years ago. The decision was made to intubate the patient, who had a Glasgow Coma Score of 3 and a saturation of 65 to 70 on arrival. The patient could not be intubated after 2 attempts and a tracheostomy was performed through an emergency incision. Subsequently, the saturation increased to 90 and the patient was followed up in the intensive care unit, and computed tomography (CT) scans of the brain, neck, and chest were performed. The CT images of the neck showed a well-circumscribed hypodense lesion with a mean density of −98 Hounsfield units, measuring approximately 40 mm × 96 mm × 120 mm, extending from the right retropharyngeal region to the medial aspect of the left carotid sheath. There were thin linear septations within the lesion. Anteriorly, there was significant compression of the air column, especially at the supraglottic level of the larynx (Figure 1). With these features, the lesion was diagnosed as a retropharyngeal lipoma. The patient’s brain CT scan was unremarkable. Opacities in the posterobasal segments of the bilateral lungs on chest CT were interpreted as suggestive of aspiration pneumonia and medical treatment was initiated. During follow-up, the patient’s Glasgow Coma Scale score was 13 and he was followed up in the psychiatric ward. Magnetic resonance (MR) imaging performed for lipoma showed that the lesion in the retropharyngeal area was hyperintense on T1- and T2-weighted images, suppressed on fat-suppressed sequences, and did not restrict diffusion (Figure 2). Surgery was recommended due to significant air column obstruction, but the patient refused. The patient was discharged with recommendations.
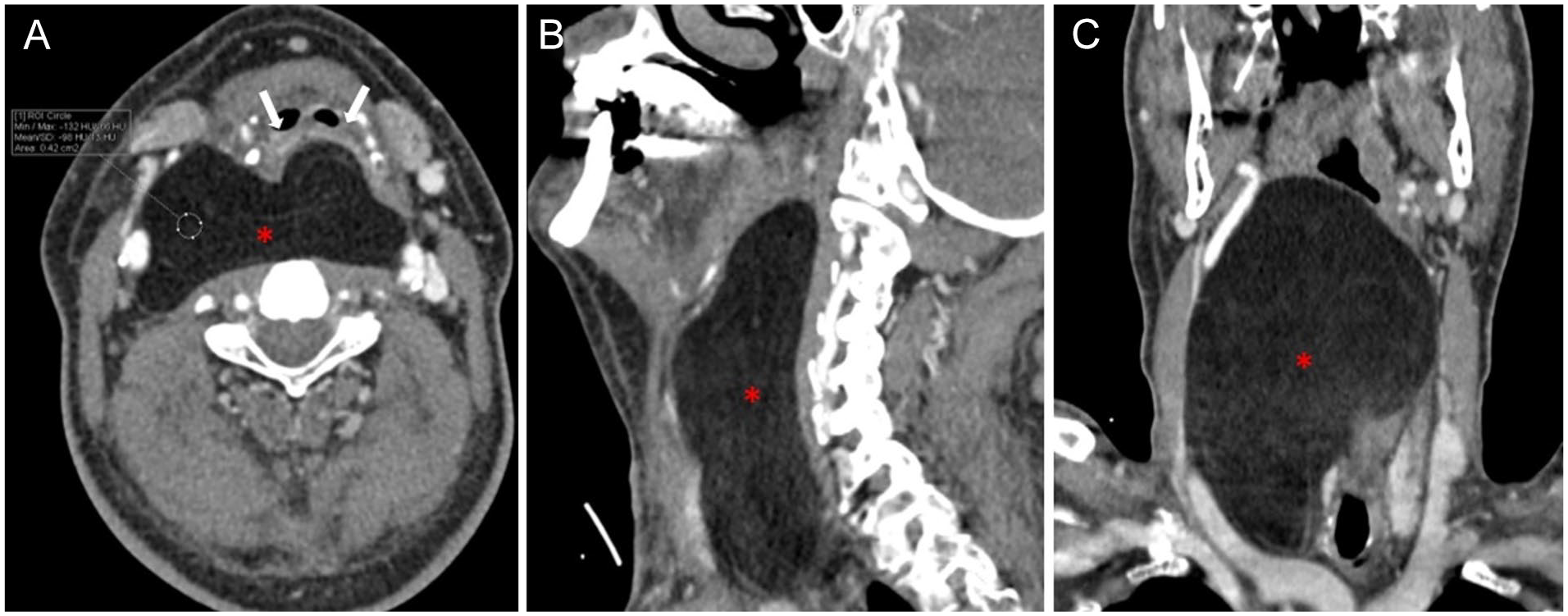
Axial (A), sagittal (B), and coronal (C) contrast-enhanced CT images show a smoothly circumscribed, noncontrast enhancing lesion (asterisk) with fat tissue density (−98 HU). The lesion causes significant compression of the air column anteriorly (arrows). CT, computed tomography.
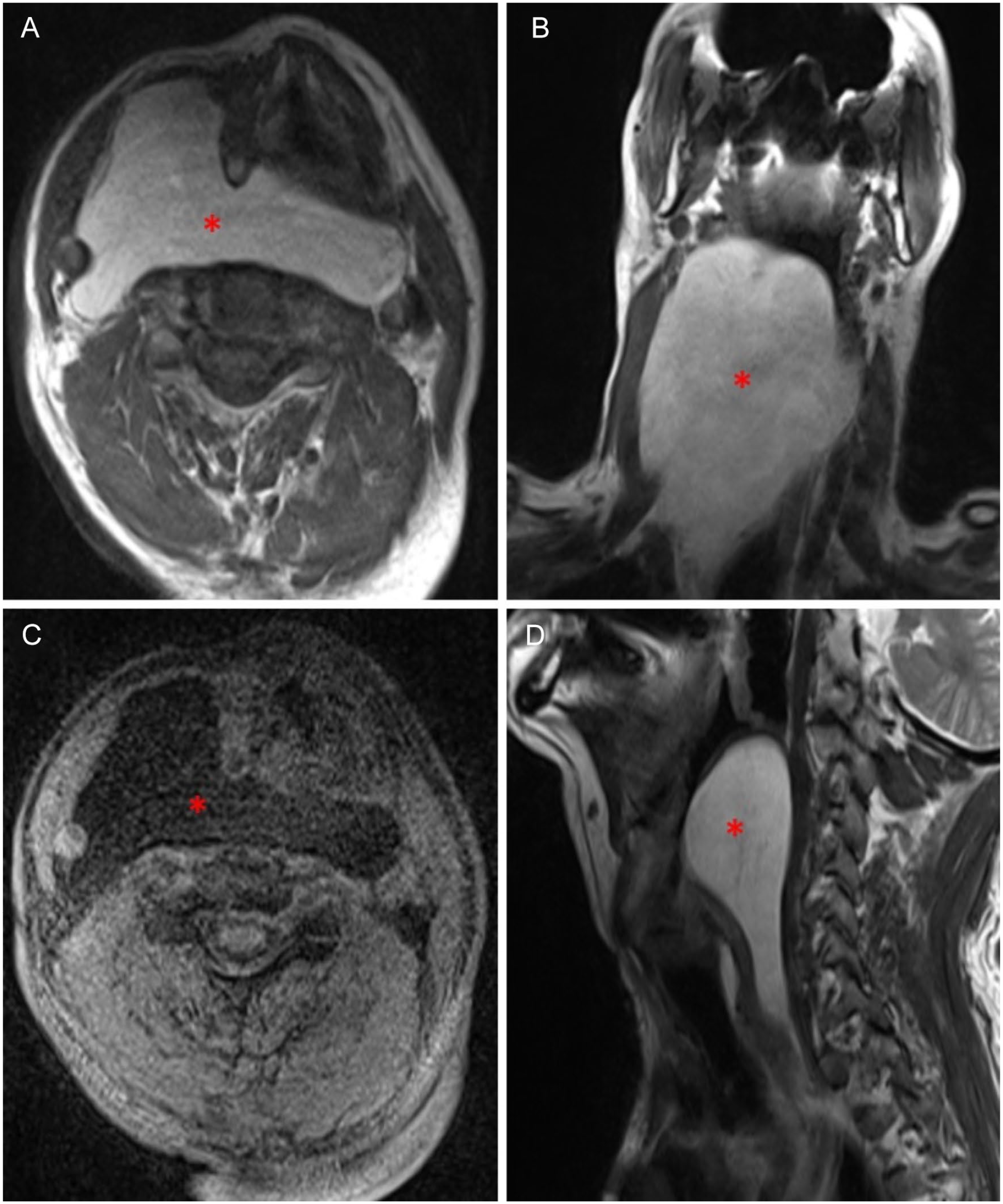
On the MR images, the lesion (asterisk) appears hyperintense on the T1 axial (A) and coronal (B) slices, suppressed on the axial slice fat-suppressed T1-weighted sequence (C), and hyperintense on the T2-weighted sagittal slice (D). MR, magnetic resonance.
The retropharyngeal space is between the buccopharyngeal and alar fascia and contains adipose tissue, lymph nodes, and blood vessels. Primary tumor of this space extending from the skull base to the mediastinum is very rare. Lipomas, which are benign mesenchymal tumors, are common and 13% of them are located in the head and neck region. It is 2 times more common in males and the average age of presentation is 50 years. However, lipoma in the retropharyngeal region is very rare and less than 100 cases have been reported in the literature. Since lipomas are slow-growing lesions, they are usually detected incidental and are asymptomatic. Symptoms that develop when they grow are usually related to compression and these are dysphagia, snoring dyspnea, dysphonia, obstructive sleep apnea, daytime somnolence, and neck swelling.1-3 Radiological imaging is crucial because the retropharyngeal area is far from the inspection. Histopathology is necessary for the definitive diagnosis of lipoma. However, on CT imaging, a well-demarcated, noncontrasting, fat tissue density (−50 to −150) appearance without infiltration and calcification is typical. MR imaging is mostly used in preoperative planning. Lipoma is hyperintense on T1-weighted imaging and suppressed on fat-suppressed sequences. It may contain fine septations. Surgical resection via transoral or transcervical approaches is preferred in treatment.2-5
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.