
Abstract
Lipoma is a benign mesenchymal tumor primarily found in subcutaneous fat. Post-traumatic lipoma (PTL) sporadically associates with blunt of penetrating trauma, but the exact mechanism remains not fully understood. This article unveils a rare case of a 32-year-old male presenting with a cervical lipoma at a previous surgical incision, an unprecedented occurrence. The patient incidentally detected the mass and underwent complete excision, with pathology confirming the diagnosis. The etiology of PTL remains speculative, with proposed mechanisms postulating inflammatory chemokines inducing preadipocyte differentiation and acute trauma causing septal rupture, allowing lipoma formation. Notably, the prior use of blade in our patient’s surgical procedure aligns with this hypothesis. The varied nature of trauma encompasses acute, blunt, and penetrating injuries. This case represents the second instance attributed to penetrating trauma and the first occurrence at a surgical incision site.
Introduction
Lipoma is a painless, slow-growing benign tumor of mesenchymal origin. 1 It can be located in all organs where fat is normally found especially the subcutaneous tissue. It is a proliferation of adipocytes with a thin fibrous surrounding capsule and that distinguishes it from pseudolipomas which are nonencapsulated herniation of the subcutaneous fat without de novo growth of adipose. 2 The incidence of lipomas is 1% of all benign tumors in the human body, 1 about 13% of all cases occur in the head and neck regions, and the most common sites are the posterior cervical triangle and forehead. 3 Transformation into a malignant tumor is uncommon, but liposarcoma appear to be the most frequent. 4 Trauma and lipoma most frequently correlate on clinical history and it is named post-traumatic lipoma (PTL). The etiology of PTL was first described in 1932 by Adair et al. 5 PTL phenomenon is still poorly understood and there are many hypotheses of the origin of it. However, none of them have been proven. 6 There is a limited number of reported PTL cases and most of them are after blunt trauma. In this article, we are presenting a case of cervical lipoma in site of surgical incision which has not been reported before.
Case Report
A 32-year-old male presented with an asymptomatic and slow-growing mass in the upper left region of the neck which was incidentally noticed after beard shaving 2 years ago. He mentioned a story of a gunshot accident 5 years ago in the left side of his face (upper the angle of mandible), where the extraction of the bullet was hindered. As a result, he experienced restricted jaw movements. Consequently, he underwent mandibular reconstruction surgery using submandibular approach (below and under the angle of mandible) at the same site as the recently noticed mass. Remarkably, there was no bruising, hematoma formation, or subsequent trauma at that site after the surgery. The mass did not affect the swallowing or breathing. There was no medical history or familial precedent pertaining to this condition. By examination a soft, mobile, nontender, nonfluctuant, and regular mass with normal sensation was noted, along with the presence of a distinct scar at the site of the previous surgical intervention (Figure 1). There was no associated cervical lymphadenopathy. Laboratory analysis was within normal range including cholesterol and partial thromboplastin time. His body mass index is 27.9 (over weight).
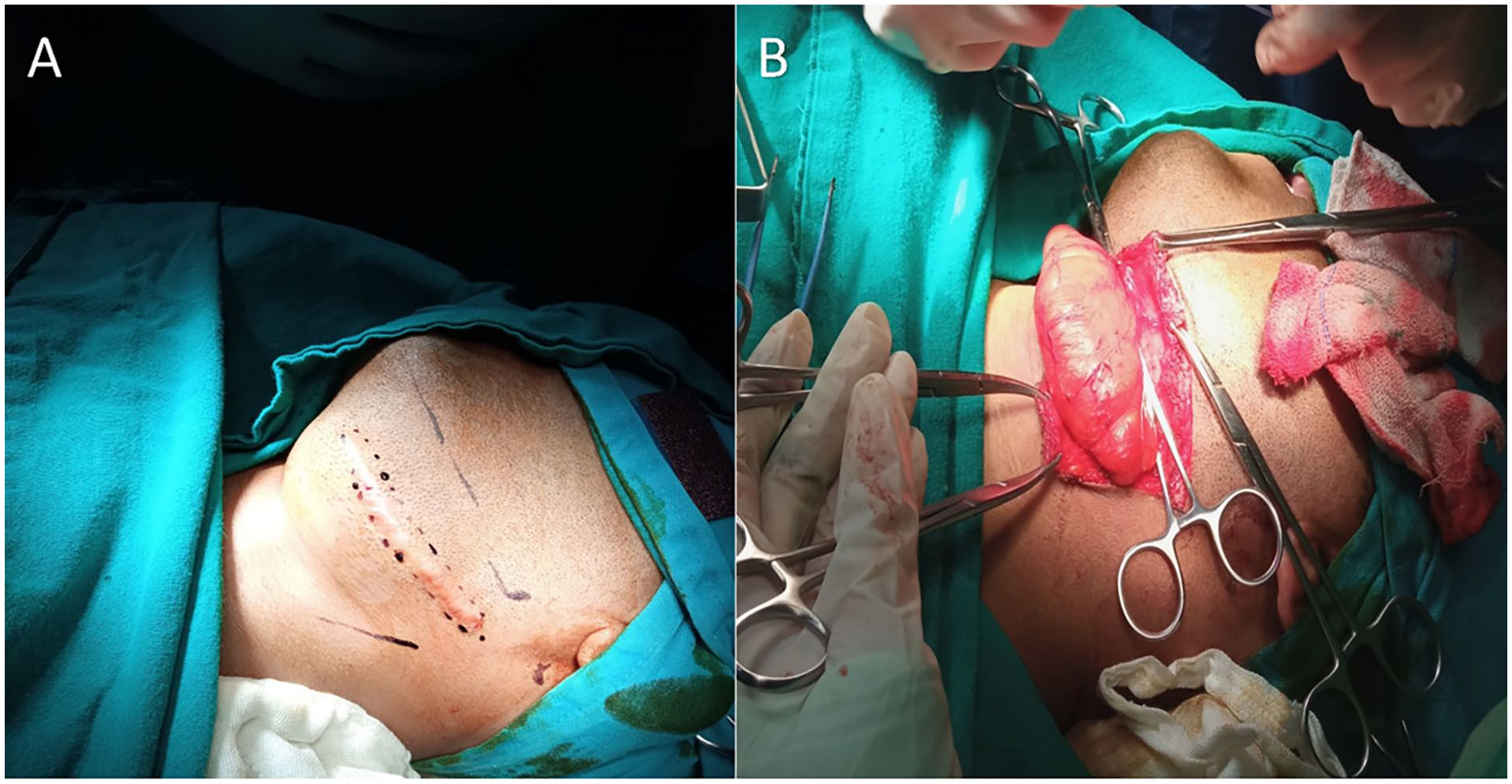
(A) View of the surgical site in addition to the distinct scar. (B) Intraoperative view of the lipoma along the surgical incision.
An ultrasound scan detected a well-defined, nonvascular, hypoechoic mass on the left side of the neck, while the computed tomography scan revealed an 8.4 cm × 2.8 cm well-demarcated, low-density mass.
The mass was completely excised via surgery, and the surgical excision was performed via transverse upper crease cervical incision that include the previous scar, then the mass was isolated from the submandibular space contents. Ultimately, the diagnosis was confirmed through pathological study, identifying it as a lipoma (Figure 2).
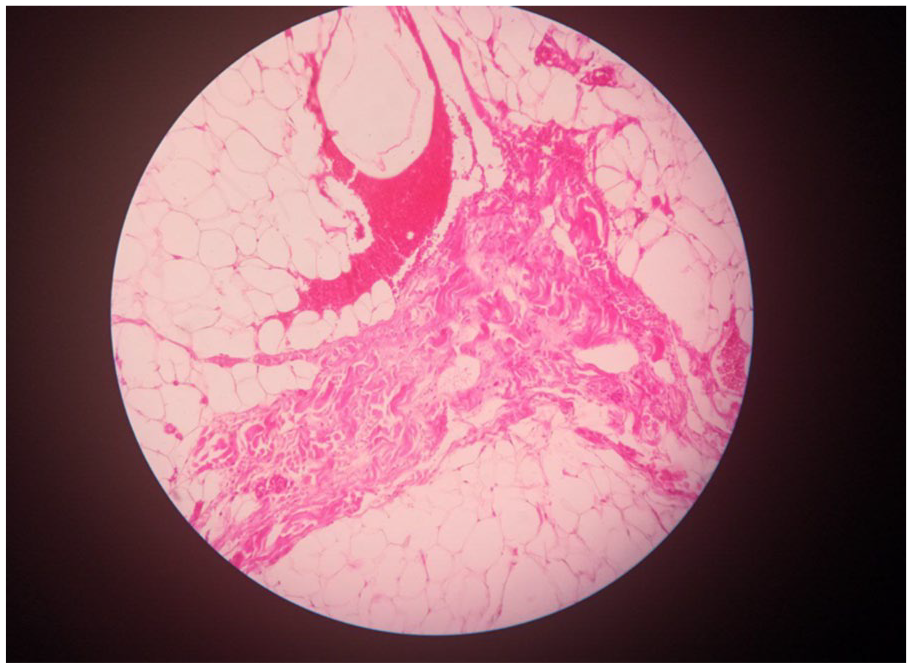
Histologic examination shows polygonal fatty cells, mild focal leukocytic infiltrate, thick fibrous septa, and hemorrhage without atypical cytologic features.
Discussion
PTLs are soft tissue neoplasms of fat cells that develop after trauma. 2 Genetic factors are implicated in lipoma development, with approximately two-thirds of patients exhibiting genetic alterations. These changes involve the HMGA2 gene and chromosomal aberrations at 12q13-15, playing a role in the tumor’s pathogenesis. 7 The types of traumas include acute or blunt trauma and penetrating injuries.2,5,6 Our patient is the second case resulting from penetrating trauma, the first being a lipoma in the parotid gland. In addition, this is the first case at the site of surgical incision. 3 The patient became aware of the mass approximately 18 months following the previous surgery. This falls within the timeframe of 5 months to 6 years, a range noted in medical literature for the development of lipomas after trauma.2,4 There is no proof of a specific hypothesis of origin of PTLs. However, one of them had postulated the role of inflammatory chemokines in inducing the differentiation of preadipocytes into mature adipocytes forming new adipose tissue, and the presence of lymphocytes in some fields of our histological studying might support this mechanism. 5 The other theory suggests that acute trauma leads to a rupture of the septa that separates fat from the tissue above it, which allows lipoma formation in that place as a result of the fat herniation through the damaged part. The previous use of the blade in our surgical work and tissue cutting might support this hypothesis. 4
The mass exhibited a slow growth pattern, incidentally noticed by the patient while shaving his beard, without presenting any compression symptoms, despite its considerable length of 8.2 cm in the neck. Given that the mass was nonsymptomatic, the cosmetic concern prompted the patient to opt for surgery. Despite various surgical techniques aimed at minimizing incision size to preserve cosmetic appearance, we chose a complete surgical excision along the length of the mass to remove the previous substantial scar in the same area. 8
Conclusion
The report details a distinctive case involving a 32-year-old male harboring a cervical lipoma at a prior surgical site, an unprecedented occurrence in PTLs. The extension of the mass along the same path as the previous surgical incision and scar strongly supports the surgical incision as an unprecedented cause in medical literature. Despite trauma’s correlation, the precise etiology of PTLs remains uncertain, warranting deeper exploration for enhanced diagnostic strategies and patient care optimization.
Footnotes
Acknowledgements
The authors are grateful for their colleges and mentors in Al-Mouwasat Hospital.
Author Contributions
MH: Contributed to original draft and design of the study and publishing of the final manuscript.
KJH and MYI: Contributed to original draft and collect data of the case presentation and interpretation of the results.
AA: Supervising and editing some points in the final manuscript.
All authors read and approved the final manuscript.
Data Availability
The data that support the findings of this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases. Written informed consent was acquired from the patient for publication of this article.