
Abstract
Hypopharyngeal liposarcomas are extremely rare. Due to the lack of experience, pathologists and surgeons find it difficult to make a clear diagnosis and provide accurate, timely treatment. A 43-year-old man with a complaint of foreign body sensation in the throat for 6 months and swallowing difficulty for 2 months was admitted to our department. Contrast-enhanced computed tomography of the chest and larynx revealed a lesion with smooth surface in the esophagus, connected by a pedicle to the hypopharyngeal lesion. The same result was found by gastroscopy. Lateral pharyngotomy was performed for tumor removal, and after 3 weeks, the patient showed good movement of bilateral vocal cords, without dysphagia, choking cough, or hoarseness. This is the first case report of hypopharyngeal liposarcoma invading the esophagus. A thorough preoperative evaluation may be required for the proper diagnosis, prevention, and treatment.
Introduction
Liposarcoma is a malignant mesenchymal tumor, accounting for approximately 20% of all mesenchymal tumors. It is the most common malignant soft tissue tumor in humans, with a predilection for men aged 40 to 60 years. 1 Liposarcoma usually develops in the extremities, trunk, or retroperitoneal soft tissues and is extremely rare in the hypopharynx or esophagus. Although its classification as a malignant tumor is controversial, there is little evidence of malignant transformation of a liposarcoma from a benign tumor. 2 However, some experts maintain that long-standing lipoma may undergo malignant transformation. 3 More than 9% of liposarcomas occur in the head and neck. To date, only 40 cases of laryngeal liposarcoma have been reported, with the most common type being supraglottic. 4
The diagnosis of hypopharyngeal liposarcoma is challenging because in the early stage it usually does not manifest as clinical symptoms, such as cough, sleep apnea/snoring, or dysphagia. With the progression of hypopharyngeal liposarcoma, airway and swallowing obstructions may occur. The symptoms and signs of hypopharyngeal liposarcoma and lipoma are similar. Both of them present as well-defined, pedunculated, submucosal, smooth, and painless masses. 5 Therefore, they are difficult to distinguish in clinic and necessitate complete tumor removal. The confirmation depends on postoperative histopathology and immunohistochemistry. Liposarcoma in the head and neck is usually well-differentiated, with a low degree of malignancy and better prognosis compared to liposarcoma in other sites. 6 Esophageal soft tissue sarcoma, particularly liposarcoma, is rare. In 1983, Mansour et al first reported esophageal liposarcoma. 7 To date, only 42 cases have been reported in the English literature. 8 Liposarcoma can be divided into 4 subtypes: dedifferentiated, well-differentiated, myxoid, and pleomorphic.
Since hypopharyngeal and esophageal liposarcomas are rare, no case of simultaneous occurrence in a patient has been reported. Caceres et al reported large pedunculated polyps originating in the esophagus and hypopharynx. 9 Currently, there is no reported clinical case or treatment protocol of hypopharyngeal liposarcoma invading the esophagus. Herein, we report a rare case of hypopharyngeal liposarcoma involving the esophagus and describe the clinical management.
Case Report
A 43-year-old man who complained of foreign body sensation in the throat for 6 months and had a history of swallowing difficulty for 2 months was admitted to an ear, nose, and throat department for evaluation of dysphagia. The patient initially presented with laryngeal foreign body sensation, without odynophagia, hoarseness, or dyspnea. After 4 months, the foreign body sensation increased, accompanied by dysphagia, slight dyspnea during exercise, and vague pronunciation. Computed tomography (CT) of the larynx revealed a round glottic laryngeal mass on the left side. The mass showed a slightly lower density shadow with a wide base connected to the posterior wall with uneven density, clear boundary, and a maximum diameter of approximately 2.5 cm.
Contrast-enhanced CT of the chest and larynx showed a mass in the posterior part of the left hypopharynx with a size of approximately 30 × 25 mm. The mass had slightly low density with uneven internal density. The sinus piriformis had disappeared on the same side. The focus seemed to be slightly enhanced, with an obvious ring-shaped enhancement on its wall. The wall of the upper part of the esophagus was unevenly thickened and had a narrow lumen. The thoracic esophagus at the T4 to T7 vertebral levels was dilated with a 35 × 63 mm mass connected by a pedicle in its lumen to a hypopharyngeal lesion. Both lesions were considered to be have the same origin, without lymph node metastasis (Figures 1–4).

Axial computed tomography showing a mass arising from the left hypopharynx.

Axial computed tomography showing a mass in the esophagus.
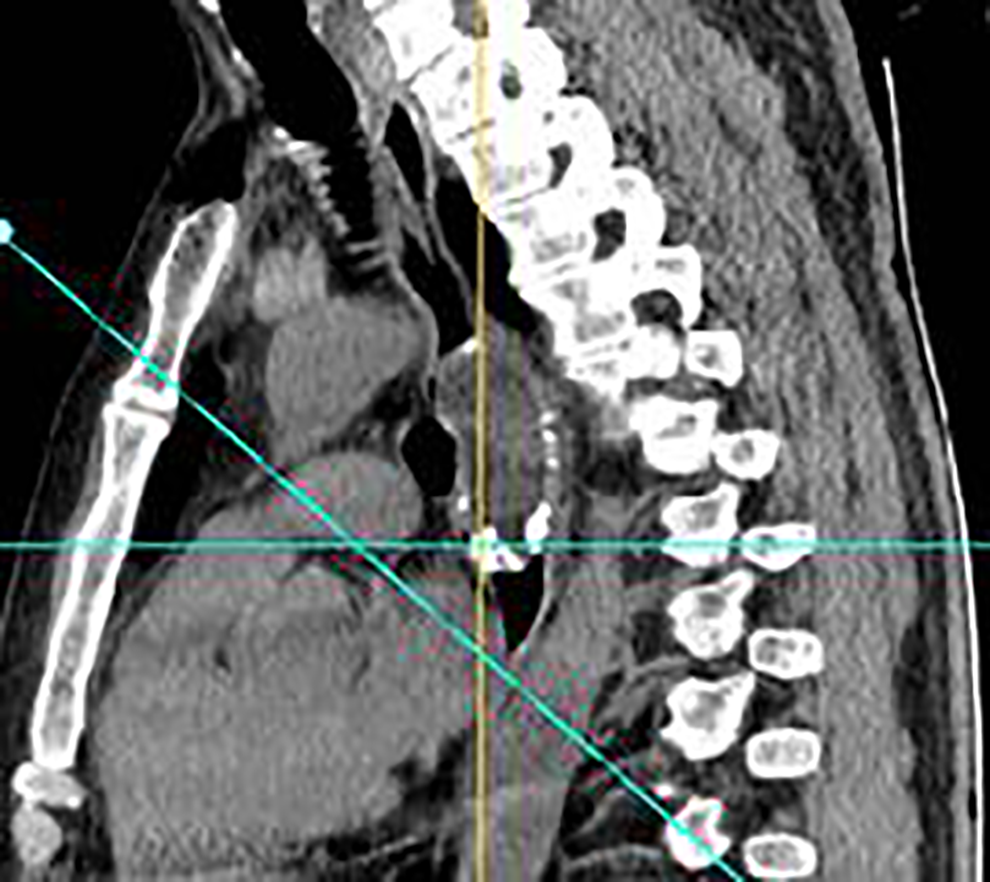
Sagittal computed tomography showing a mass with a pedicle in the esophagus.

Coronal computed tomography showing a mass in the esophagus with obvious calcification.
Considering that the hypopharyngeal mass was sufficiently large to block the glottis, we made a tracheotomy in the patient to avoid asphyxia during gastroscopy. Gastroscopy showed that the long pedicle connecting the 2 large lesions could be seen from the left sinus piriformis to an extent of 30 cm from the incisor, which was free from the surrounding area. The surface was smooth, without obvious ulceration or erosion (Figures 5 and 6).
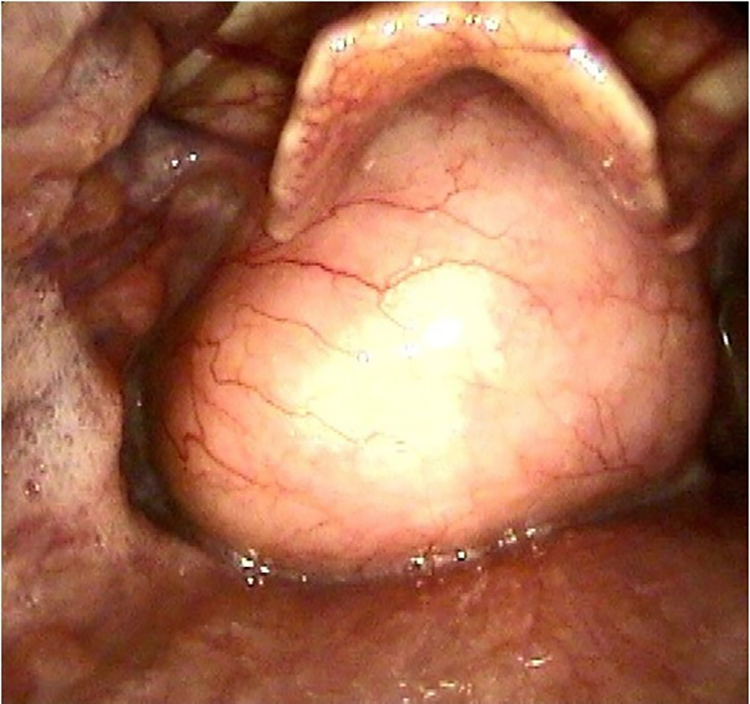
Endoscopic image of a mass in the hypopharynx.
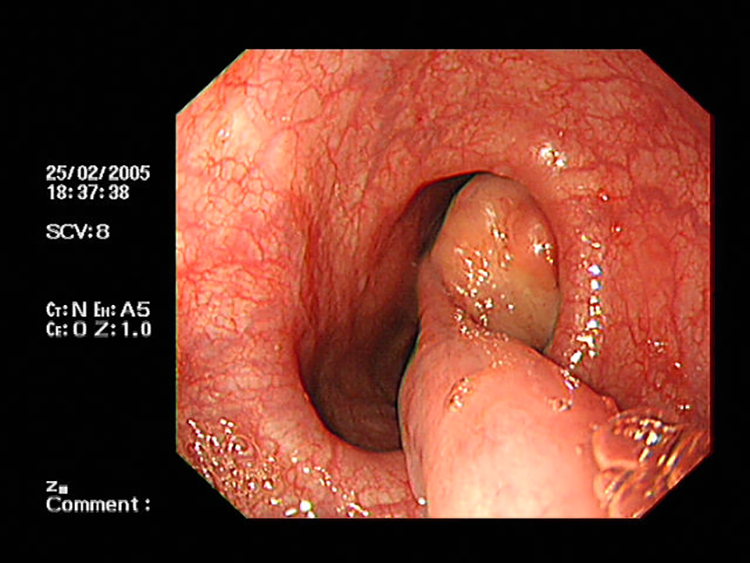
Endoscopic image of a mass with a pedicle in the esophagus.
General anesthesia was induced by intubation through a previous tracheotomy. After a thorough preoperative evaluation, lateral pharyngotomy was performed for tumor removal. The procedure is outlined below.
An oblique incision was made in the anterior cervical trachea and extended toward the left side up to the front of the sternocleidomastoid muscle. After opening the platysma muscle, the superior horn of the left thyroid cartilage was exposed, separated, and excised. Pulling the thyroid cartilage to the right side, laryngopharyngeal mucosa was dissected vertically at the lower edge of the left thyroid cartilage plate. A smooth, hard mass with a diameter of 3 cm appeared in the left sinus piriformis, connected to its inner wall. The root base extended to the esophagus and was connected to the esophageal wall at the entrance. The chief surgeon extended the index finger into the esophagus and found that the pedicle was free from the esophagus. After dilating the entrance of the esophagus, the pedicle was pulled up slowly to expose a 4 × 6-cm2 solid mass. The mass was resected together with a 10-cm long pedicle (Figures 7–10). The surgery area was sutured layer by layer. Pathological findings were consistent with an atypical lipomatous tumor or a highly differentiated liposarcoma (Figures 11 and 12).
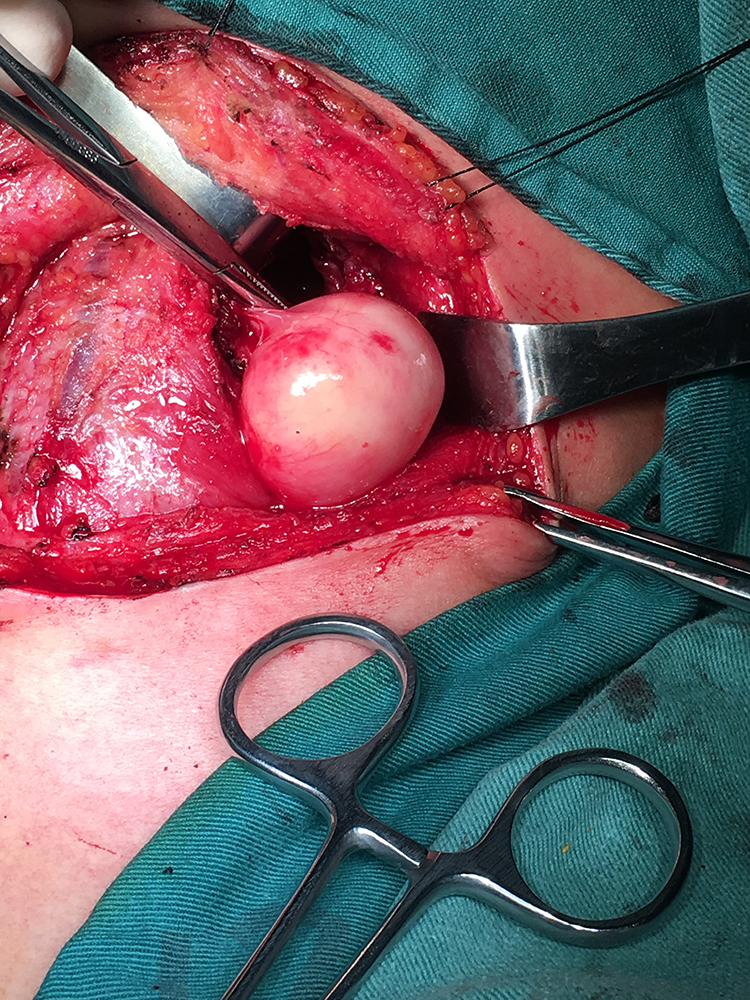
A cut in the laryngopharyngeal mucosa vertically at the lower edge of the left thyroid cartilage plate showing a smooth hard mass with a diameter of 3 cm in the left sinus piriformis.
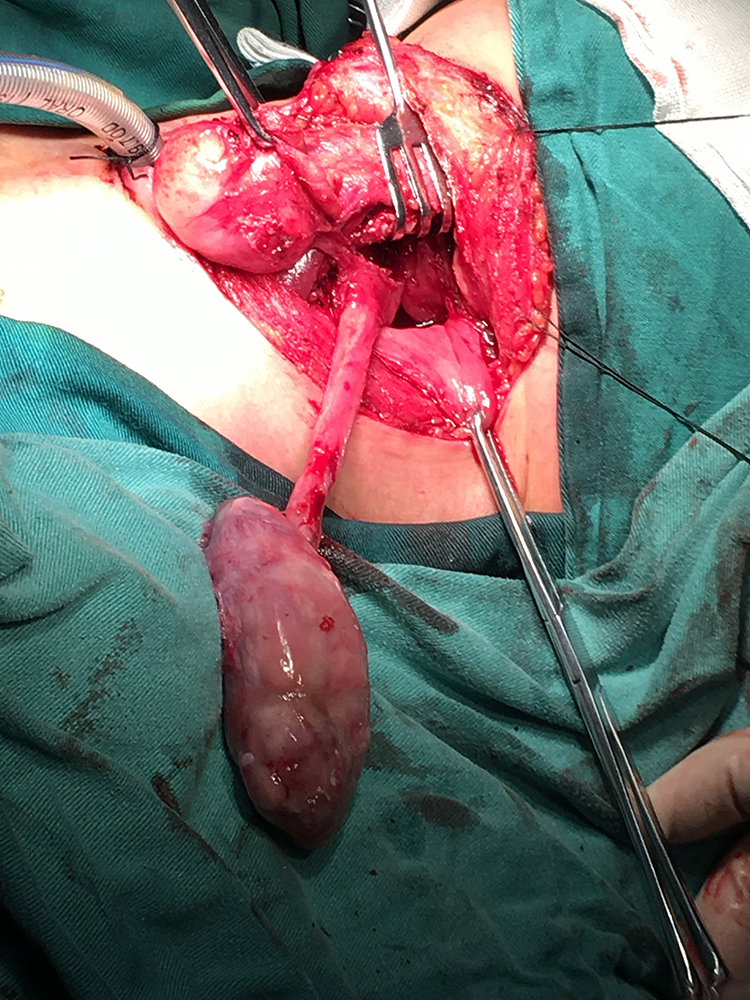
Dilating the entrance of the esophagus, following the pedicle, and pulling the esophagus mass upward.

Macroscopic findings of a surgical specimen.

Macroscopic findings of a surgical specimen.
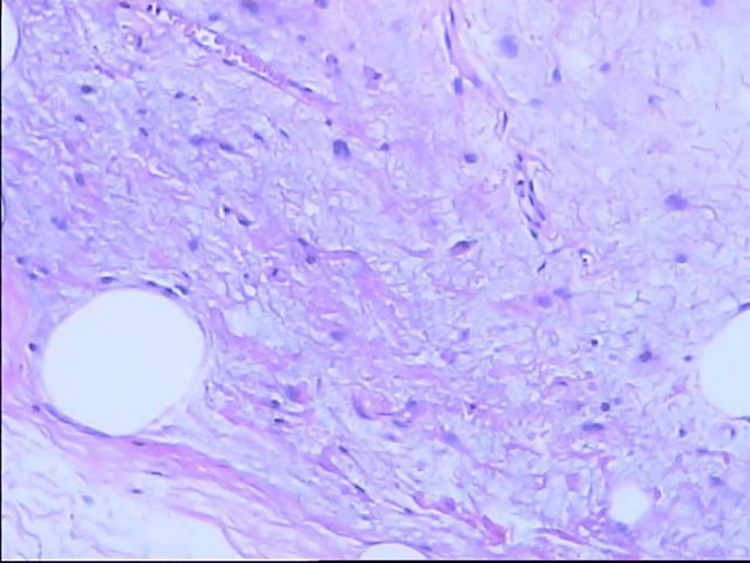
Histopathology results, revealing a lipogenic tumor, combined with immunohistochemistry results, suggesting an atypical lipomatous tumor or a highly differentiated liposarcoma.
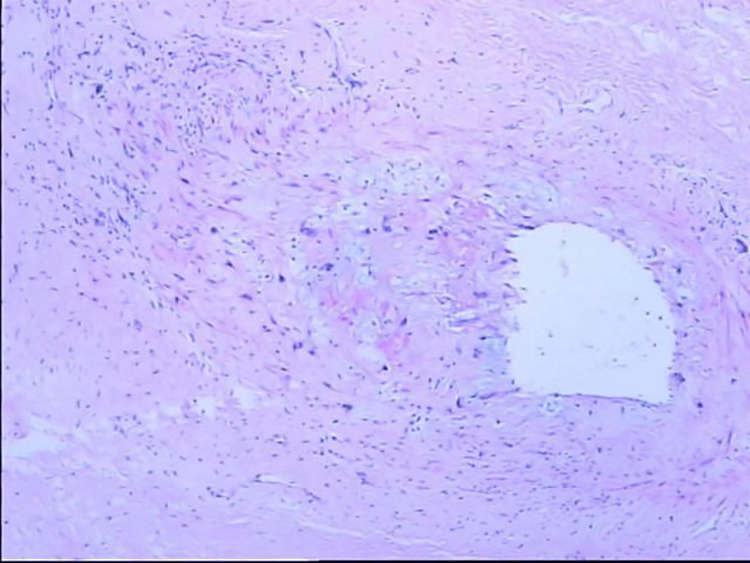
Histopathology results, revealing a lipogenic tumor, combined with immunohistochemistry results, suggesting an atypical lipomatous tumor or a highly differentiated liposarcoma.
The gastric tube was removed 3 weeks postoperatively. The patient did not have dysphagia, choking cough, or hoarseness and showed good movement of bilateral vocal cords. No abnormalities were detected after oral feeding. Currently, at 10 months postoperatively, the hypopharyngeal tumor has not recurred. The patient provided informed consent for publication of this case and the associated images.
Discussion
Liposarcoma is a soft tissue sarcoma with adipocyte differentiation and a predilection for men aged 40 to 60 years. 1 It is mainly found in the deep soft tissues, particularly of the thighs, and retroperitoneum of the limbs as painless, slow-growing tumors. Despite being the most common mesenchymal tumor in adults, it is extremely rare in the hypopharynx or esophagus. 10
Although there are different classification systems, the most widely accepted system for liposarcoma is the one developed by the World Health Organization. According to that system, liposarcoma is divided into 4 subgroups: well-differentiated, pleomorphic, myxoid, and dedifferentiated. Well-differentiated liposarcoma account for approximately 30% to 40% of all liposarcomas, second only to dedifferentiated liposarcoma. 11
Well-differentiated liposarcoma is common in the head and neck, particularly the esophagus. To date, there has been no reported case of hypopharyngeal liposarcoma invading the esophagus. Therefore, there is no previous experience or treatment protocol for it.
Hypopharyngeal and esophageal liposarcomas have similar pathological characteristics. 12 Similar to esophageal liposarcoma, hypopharyngeal liposarcoma is usually a slow-growing tumor. In the early stage of tumor growth, patients experience no typical symptoms until the tumor is enlarged and compresses the surrounding tissues and organs. The main clinical manifestations are progressive dysphagia, nausea, vomiting, foreign body sensation in the throat, odynophagia, dyspnea, and asphyxia. The symptoms of esophageal and hypopharyngeal liposarcomas are similar. In the present case, foreign body sensation in the throat for over 6 months and progressive dysphagia for over 2 months were the main manifestations. The patient had undergone endoscopic laser surgery for hypopharyngeal lipoma 2 years before, and the postoperative pathology had shown lipoma. The patient had not been followed-up regularly because of resolution of dysphagia and foreign body sensation. At first, both the patient and doctor thought that the hypopharyngeal lipoma recurred, without considering that the tumor had invaded the esophagus. Because the symptoms and signs of hypopharyngeal lipoma are similar to those of hypopharyngeal and esophageal liposarcomas, we had initially suspected the recurrence of hypopharyngeal lipoma in this case and therefore planned to perform endoscopic resection of the tumor again. However, chest CT performed preoperatively helped prevent the misdiagnosis.
Computed tomography and magnetic resonance imaging (MRI) are essential for accurate assessments of the size, location, and extent of a tumor as well as its relationship with peripheral nerves and blood vessels. Simultaneously, they can assist in the detection of distant metastasis. Liposarcoma often presents as fat-density masses with regular outlines. On MRI, well-differentiated liposarcoma shows an increased fat signal intensity, similar to other benign tumors, particularly lipomas. Therefore, the diagnosis of liposarcoma, particularly well-differentiated liposarcoma, is challenging. Histological examination is the only method to distinguish these tumors. According to the literature, the diagnoses of hypopharyngeal and esophageal liposarcomas are mainly based on barium swallow and endoscopy. The barium swallowing examination often shows smoothly marginated filling defects and tension-free esophageal widening. Endoscopic examination can reveal the location, texture, shape, and size of a tumor directly. For tumors with a pedicle, the length of the pedicle and its relationships with the esophagus and hypopharynx can be clearly detected by endoscopy. Therefore, endoscopy has great significance for designing a surgical strategy.
The standard treatment for well-differentiated liposarcoma is surgery.13,14 Considering that differentiated liposarcoma usually does not metastasize, lymph node dissection is not recommended. 15 Because of the complexity of the head and neck structures, complete tumor resection for preserving pharyngolaryngeal function is difficult. In some studies, local recurrence was as high as 80% because of incomplete resection. 13 Therefore, radiotherapy is necessary for patients without complete resection. To date, there has not been reliable evidence to support chemotherapy for liposarcoma of the head and neck. 14
Preoperatively, gastroscopy should be performed to evaluate the relationship between the root of the tumor and the esophagus. Due to obstruction of the glottis by a large tumor, the present patient developed mild dyspnea. At that time, performing gastroscopy directly would have posed a high risk of suffocation, regardless of the type of anesthesia. Therefore, a tracheotomy was made to ensure safety before the gastroscopic examination. Anesthesia was also induced by intubation through the tracheotomy. Patients need to wear tracheal tubes for airway safety. Thus, a preoperative tracheotomy has been proven to be necessary.
There are 2 surgical methods for hypopharyngeal liposarcoma: lateral pharyngotomy and endoscopic surgery. Endoscopic surgery has the advantages of less trauma and quick recovery but the disadvantage of difficulty in removing the tumor completely. Since the patient had undergone endoscopic resection of hypopharyngeal lipoma 2 years before, we suspected local tumor recurrence. Lateral pharyngotomy could be used to identify the tumor boundary and remove the tumor completely, with disadvantages of severe trauma and long postoperative recovery time.
In the strict preoperative evaluation in this case, we found hypopharyngeal and esophageal masses, connected by a pedicle. The pedicle originated from the left pyriform fossa, partially adhered to the esophageal entrance, and was completely dissociated from the esophagus. Simultaneously, the esophageal mass was free from the esophagus. Therefore, we made a bold attempt by exposing the hypopharyngeal mass using lateral pharyngotomy and then expanding the esophageal entrance. The esophageal mass along with the pedicle could then be removed from the esophagus by resecting the root of the pedicle attached to the esophageal entrance retrogradely. The operation went well, and tumors were completely removed. The patient did not receive radiotherapy or chemotherapy postoperatively. Four months postoperatively, the patient did not show abnormal respiration or swallowing or the prior sense of obstruction. Laryngoscopy revealed a smooth bilateral pyriform fossa and no new mass. At present, we are continuing to follow-up the patient.
In conclusion, hypopharyngeal liposarcoma invading the esophagus is an extremely rare tumor. Dysphagia and foreign body sensation are the most common initial manifestations. Since the esophageal entrance has its own tension and is not easily exposed by endoscopy, endoscopic surgery often faces a great challenge in dealing with such cross-border tumors. Because liposarcoma is pedunculated and well-differentiated, complete resection with a clear margin can effectively prevent recurrence. Lateral pharyngotomy is a good option. Due to a high incidence of recurrence, a long-term postoperative follow-up after treatment is critical to improve the prognosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.