
Abstract
Epidermoid cysts are rare benign lesions that can derive from abnormally situated ectodermal tissue during embryological development or from implanted epithelium after trauma or surgery. In the oral and maxillofacial regions, epidermoid cysts usually develop in the floor of the mouth and rarely in other sites. We describe a rare case of an epidermoid cyst arising in the right maxillary sinus. A 29-year-old man with a known diagnosis of Marfan syndrome presented with progressive swelling and tenderness in the right buccal region, mimicking facial cellulitis, and refractory to medical treatment. Computed tomography scan showed a cystic lesion extending widely into the right maxillary sinus. The cyst was successfully removed with a medial maxillectomy through inferior antrostomy approach under general anesthesia. Histological examination confirmed the diagnosis of an epidermoid cyst, showing a cystic wall lined with a thin layer of keratinizing squamous epithelium and fibroma connective tissue infiltrated with inflammatory cells, with no skin appendages. There has been no evidence of recurrence during the 4 year follow-up. We also conduct a review of the English literature for the reported cases of maxillary epidermoid cyst.
Introduction
An epidermoid cyst of the maxillary sinus is a rare condition characterized by the presence of a cystic lesion within the maxillary sinus, composed of keratinized squamous epithelium and may contain pasty material. 1 Epidermoid cysts can occur in various parts of the body, but their occurrence in the maxillary sinus is considered quite uncommon.1-3 This case report highlights the clinical profile, diagnosis, management, and clinical significance of such a rare occurrence in a patient with Marfan syndrome, along with a review of the cases reported in the English literatures since 1990 to date.
Report of Case
A 29-year-old male patient with a known diagnosis of Marfan syndrome visited our otolaryngology department due to swelling on the right side of his cheek, which had been gradually increasing in size despite a 5 day course of antibiotic treatment and was accompanied by pain. During clinical examination, pronounced tender swelling in the right side cheek and upper right gingiva was observed. Endoscopic nasal examination revealed mucopurulent discharge from the right nasal common meatus. The patient had no history of sinus surgery or ophthalmic symptoms. A provisional diagnosis of right facial cellulitis was made, leading to hospitalization for further evaluation and targeted infection management.
A computed tomography (CT) scan revealed a 4 cm × 4 cm cystic lesion originating from the root of the right mandibular second premolar (Figure 1A and B). An enhancing solid component was observed at the anterior inferior portion of the lesion, fluid retention in the right maxillary sinus led to scalloping on the anterior, lateral, and posterior walls and erosion of surrounding bone.
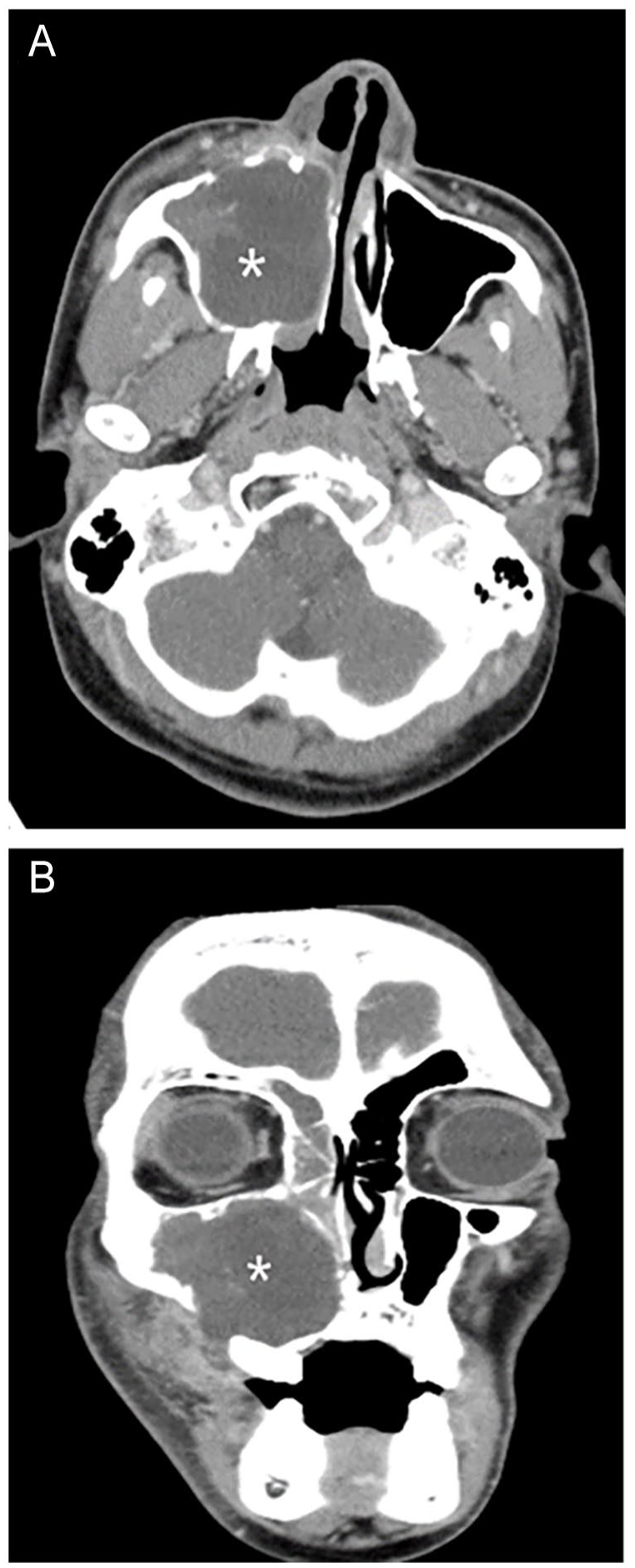
A computed tomography (CT) scan (A) at an axial section at the level of the maxillary sinus areas and (B) at a coronal section at the upper first molar region shows a well-encapsulated, hypodensity cystic mass in the right maxillary sinus (asterisk). The anterior wall of the maxillary sinus exhibited scalloping with erosion of the posterior and lateral wall.
Surgical intervention was carried out under general anesthesia with orotracheal intubation. A right maxillary bulging lesion with a significant amount of keratinaceous debris was observed within and was subsequently cleared (Figure 2A and B). A medial maxillectomy through inferior antrostomy approach was performed, along with the removal of polypoid mucosa. The lesion was totally excised. The surgical site was packed with Nasopore Forte Plus (Polyganics, Groningen, Netherlands) and later removed 2 days post operation after which the patient was discharged in a stable condition.
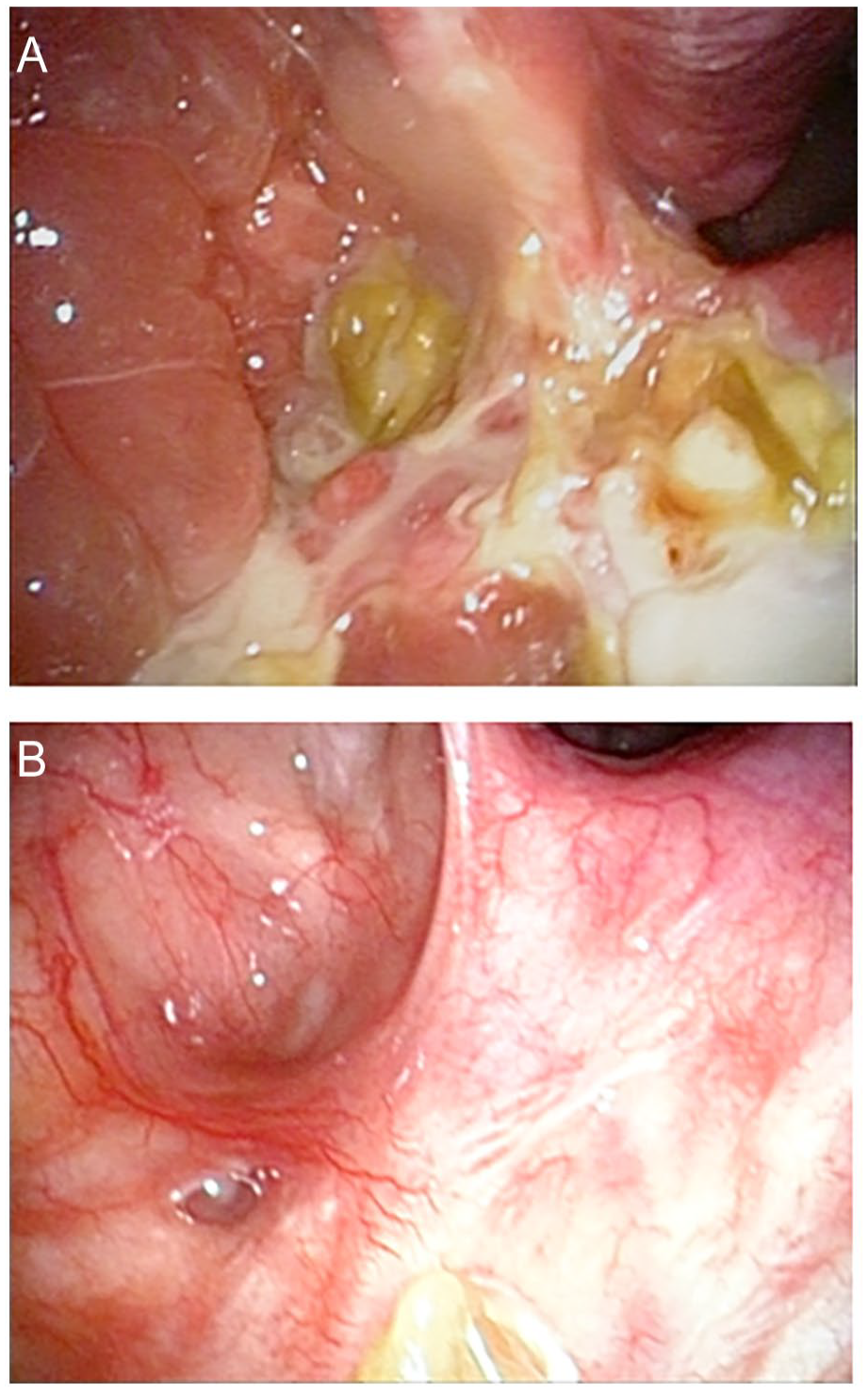
(A) Intraoperative view of the mass lesion eroding the right medial wall of the maxillary sinus with purulent material and keratinaceous debris present. (B) Four years postoperation fibroscope.
On gross examination, the lesion measured 3 cm in diameter and was grayish-pale, edematous, and mixed with pasty substance. Histopathology revealed a cystic space lined by a thin layer of keratinizing squamous epithelium supported by dense fibrovascular connective tissue (Figure 3A and B). No skin appendages were presented in the cystic wall. In addition, stromal edema, congestion, and infiltration by chronic inflammatory cells were observed. No cells suggested the presence of malignancy. Based on the clinical and histopathological findings, the lesion was diagnosed as an epidermoid cyst of the right maxillary sinus.
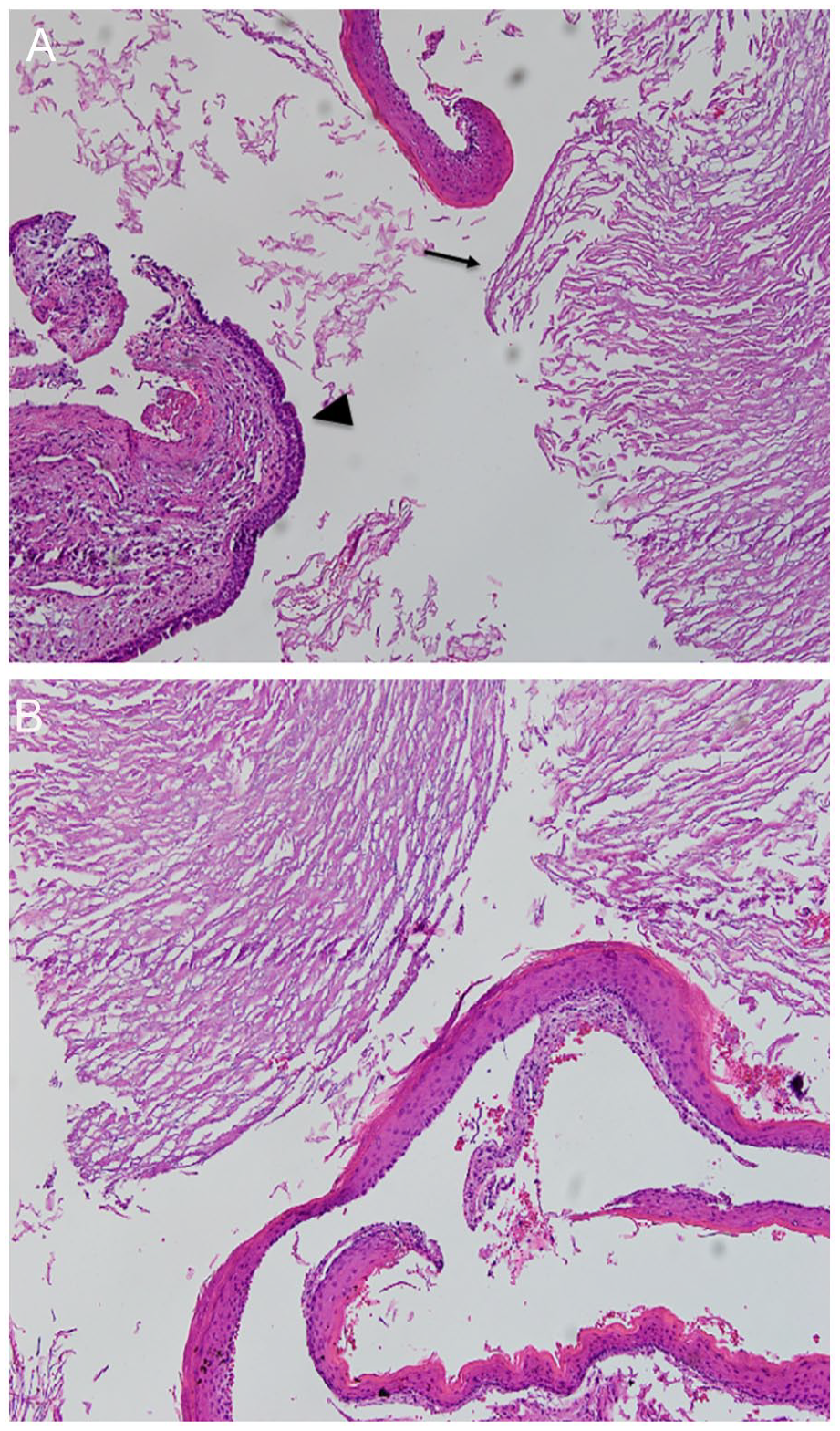
(A) Histopathologic examination. Epithelium exhibits both respiratory (arrow head) and squamous epithelial cell (arrow). Epidermoid cyst with lamellated keratin flakes and respiratory epithelium supported by dense fibrovascular connective tissue without any dermal appendage. No cell suggested the presence of a malignancy (hematoxylin and eosin, ×100). (B) Lamellar sheets of keratin materials on squamous epithelium with connective tissue (hematoxylin and eosin, ×200).
The postoperative course was uneventful. In the 5 years follow-up, the patient stayed symptom-free. Physical and endoscopic assessments conducted showed no disease recurrences.
Discussion
Epidermoid cyst can develop from abnormal epithelial components of ectoderm tissue during embryological life or from implanted epithelium after trauma or surgery.2,4 Other terms used to describe this pathology include keratocyst, epidermoid tumor, and cholesteatoma.5-7 Factors rendering individuals more susceptible to epidermoid cysts include puberty, specific rare genetic disorders, and skin injuries. 8 Most epidermal cysts are congenital.2,9 Our case involved a congenital epidermal cyst, with no history of prior trauma or surgical intervention. The association between an epidermoid cyst originating from the maxillary sinus and Marfan syndrome is unreported in existing literature. The patient in this case had a known diagnosis of Marfan syndrome, a genetic disorder affecting connective tissues, which prompts our consideration of potential links between Marfan syndrome and the development of this uncommon sinus pathology. Skin changes are documented in the Marfan syndrome in the studies previously,10,11 which include joint hypermobility and skin joint hypermobility. Previously Gosalia et al 12 has published a case report of a patient with Marfan syndrome who developed epithelial inclusion cyst in conjunctiva.
Epidermoid cysts may exhibit diverse clinical presentations, typically manifesting as small, painless subcutaneous nodules, often characterized by a central pore. In cases of infection or inflammation, additional symptoms may include skin redness, tenderness, warmth, and the discharge of grayish-white, malodorous material. 13 As demonstrated in our case, the initial presentation of the disease can be facial swelling with pain, mimicking acute facial cellulitis. In the maxillary sinus, epidermoid cysts may lead to various symptoms such as nasal obstruction, recurrent sinusitis, infraorbital nerve dysfunction, disruption of normal sinus wall profiles, and facial deformities. However, these clinical signs are nonspecific for epidermoid cysts and can also be observed in other benign and malignant sinus tumors.14,15 Distinguishing an epidermoid cyst from other maxillary sinus conditions can be challenging, and occasionally biopsy may be required for definite diagnosis.1,16 Using immunohistochemical study including markers of proliferation, cytokeratin, and apoptosis-related factors to compare epidermoid cyst, odontogenic keratocyst, and orthokeratinized odontogenic cyst. Koizumi 17 indicated that epidermoid cyst had the lowest cellular activity (mean Ki-67 labeling index = 5.7%) in the 3 cysts and it was comparatively maturated lesion. Epidermoid cyst is biologically nonneoplastic but can erode bone and expand into adjacent areas. Malignancy change for epidermoid cyst had been reported but is extremely rare.1,18 Recent investigations on bony erosions highlighted the role of cytokines like TNFα. They act directly on the bone and indirectly by stimulating the release of proteolytic enzymes. Overexpression of epidermal growth factor receptor and transforming growth factor has also been detected, indicating that the dysregulation of these genes is associated with the initiation and progression of epidermoid cyst. 19
Surgical intervention, specifically medial maxillectomy through inferior anstrostomy approach, was performed in this case, underscoring the importance of complete cyst removal to mitigate the risk of residual epithelial tissue following incomplete excision. After complete excision, vigilant long-term follow-up is essential, as recurrence rates of epidermoid cysts in other sites have been reported.18,20 In our case, a 5 year follow-up yielded no evidence of recurrence or additional lesions, suggesting a favorable outcome.
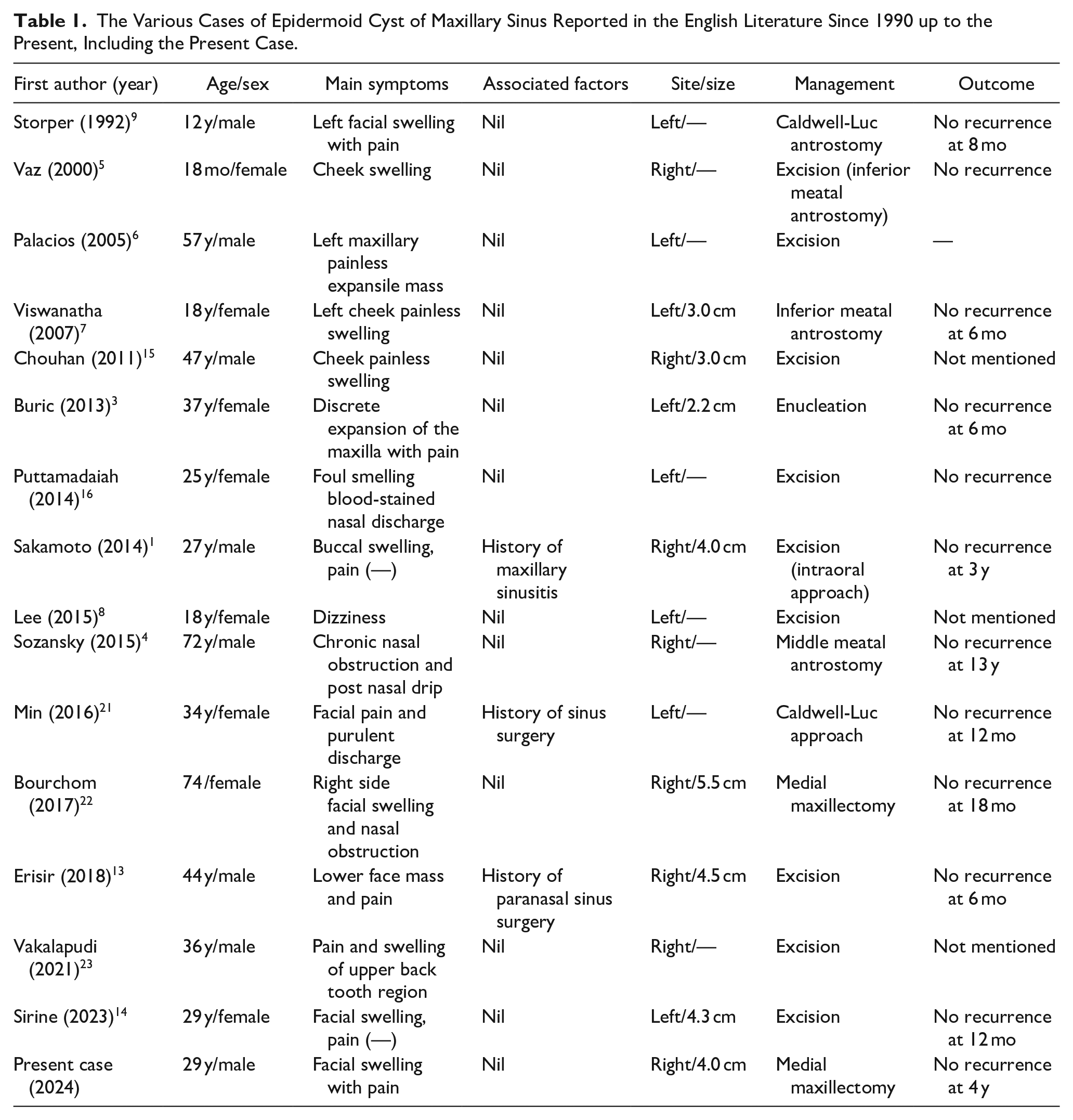
Standard treatment of this entity is by complete excision of the cyst. The appropriate surgical treatment is a Caldwell-Luc type procedure and the removal of the cyst from the antrum. However, the literature is not always clear as to the surgical approach used in the treatment of maxillary sinus epidermoid cyst. 21 A summary of 16 cases of epidermoid cysts in the maxillary sinus reported in the English literature since 1990, including the present case, is listed in Table 1. The median age of the patients was 32 years (range 12-74 years old). Eight patients (50%) were male. The lesions were equally distributed between the right (8 patients) and left (8 patients) sides of the maxillary sinus. The most frequent presentation was cheek and buccal swelling with or without pain. No cases of recurrence have been reported.
The Various Cases of Epidermoid Cyst of Maxillary Sinus Reported in the English Literature Since 1990 up to the Present, Including the Present Case.
Conclusion
This case presents an infrequent occurrence of an epidermoid cyst within the maxillary sinus, coexisting with Marfan syndrome. The potential relationship between epidermoid cyst and Marfan syndrome remains to be elucidated. Despite the rarity of epidermal cysts in the head and neck region, particularly in the maxillary sinus, they should be included in the differential diagnosis of tumors in this anatomical region. Complete surgical excision remains the preferred treatment modality.
Footnotes
Acknowledgements
None.
Data Availability
The data that support the findings of this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study received approval from the Institutional Review Board at Cheng Hsin General Hospital, Taipei, Taiwan.
Informed Consent
This study involved a retrospective analysis of medical records, and all data were fully anonymized prior to access. The Institutional Review Board committee waived the requirement for informed consent.