
Abstract
Introduction
Parotid gland neoplasms represent 2% to 3% of all head and neck neoplasms and 70% to 85% of salivary gland neoplasms. 1 Most parotid gland tumors are benign, with only 14% to 25% being malignant.1,2 Patients usually have painful swelling that grows slowly and the differentiation between benign and malignant tumors is difficult because both usually have the same clinical picture.3,4 Alarming symptoms that could raise suspicion of malignancy include pain, rapid growth, lymph node enlargement, and signs of facial nerve involvement. 5
The diagnosis of parotid gland tumors starts with a history of the patient and a neck examination. Furthermore, fine needle aspiration is a useful tool for preoperative evaluation and sometimes diagnosis due to its sensitivity of 88% and specificity of 99%. Imaging modalities such as computed tomography scan and magnetic resonance imaging help locate the exact site of the tumor and its anatomical relationships with the surrounding tissues.6,7
Surgery is the mainstay of treatment for tumors of the parotid gland, with different surgical techniques such as partial superficial parotidectomy, superficial parotidectomy, total parotidectomy, and extracapsular dissection depending on the location of the tumor and its histological type. 8 Radiative adjuvant therapy might be needed in some malignant lesions that show high-risk characteristics, while chemotherapy is used as palliative therapy and can be administered in combination with radiation therapy or as a single treatment. 9 Facial weakness or paralysis is a major complication after parotidectomy and has therefore received the greatest attention in previous studies. The estimated incidence of facial weakness ranges from 8.5% to 65.0% for temporary and 0% to 19.6% for permanent.10,11 Variations in incidence between studies can be attributed to different factors, such as benign versus malignant lesions, the extent of the disease, the surgeon’s experience, and different sample sizes. Wound complication, such as surgical site infection, sialocele, and salivary fistula, is one of the most common complications after parotidectomy. In a previous systemic review, surgical site infection was estimated to have a pooled incidence of 2.3%, with a higher incidence in elderly patients and patients with comorbidities such as chronic obstructive pulmonary disease. 12 Furthermore, the reported incidence of sialocele and salivary fistula in the literature ranges from 5% to 39%, with limited studies on factors that might increase their incidence.12-18 Another common complication that is usually neglected by both the physician and the patient is ear numbness or loss of sensation. Patients may report difficulty shaving or answering the phone. However, vulnerability to trauma is the most troubling issue. 19 Ideally, the surgeon should aim to preserve the greater auricular nerve, but preservation of the anterior branch is challenging due to its anatomical position over the tail of the parotid gland, and therefore it may be sacrificed. In contrast, the posterior branch can usually be safely preserved. 20 Frey syndrome is considered a common complication after parotidectomy, although its previously reported incidence varies significantly due to the influence of different factors, such as surgical technique, tumor size, whether or not preventive measures were used, and the subjective definition of Frey syndrome in studies.21-23
Patients and Methods
This retrospective study was conducted at King Fahad Medical City and King Abdulaziz University Hospital, Riyadh, Saudi Arabia. A total of 173 patients diagnosed with parotid gland neoplasms who underwent parotidectomy between 2015 and 2023 with regular follow-up after surgery at either location were included in the study. The time of follow-up must be minimum of 3 months to assess complications properly. We excluded patients who did not follow-up or who had incomplete documentation. When assessing patients who underwent multiple surgeries due to tumor recurrence, we considered recurrence as a complication and limited our analysis to the initial parotid surgery.
The anonymity of the participants was ensured by assigning each participant a code for analysis only. Data collected from study participants’ medical records were divided into two categories: patient characteristics and postoperative complications. Patients’ characteristics included age, sex, diabetes, and smoking status.
For demographic variables, simple descriptive statistics were used. For the prevalence of complications, the data were scrubbed for inconsistent or missing values, and descriptive statistics of all complications were performed. To determine relationships and identify any factors related to complications, chi-square tests and correlation analyzes were performed. Correlation analyzes were used for numeric values such as age and body mass index (BMI). All data were analyzed using SPSS version 23 (IBM Corp). The study was approved by the Research Ethics Committee of King Fahad Medical City (Institutional Review Board Log Number: 23-239).
Results
A total of 173 postoperative patients were involved in the study. Table 1 represents the demographic variables and their corresponding frequencies and percentages. The predominant surgical procedure performed among the patients was superficial parotidectomy, with 105 individuals undergoing this intervention. Total parotidectomy was conducted in 37 patients, while partial superficial parotid surgery was elected for 26 individuals. Notably, only 5 patients in our study sample required the more extensive radical parotidectomy. The length of the follow-up period ranged between 3 months and 7 years.
Demographic Variables.
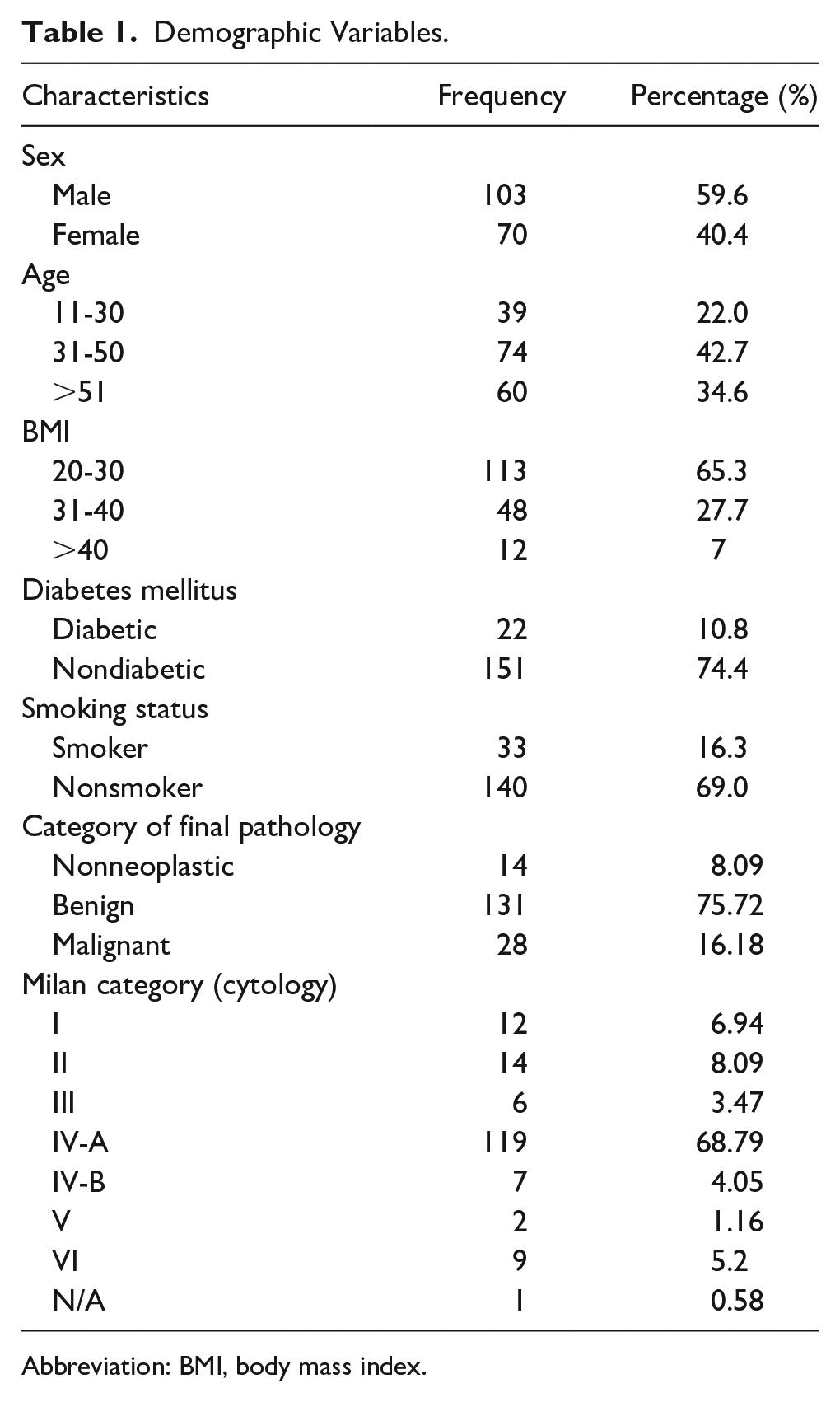
Abbreviation: BMI, body mass index.
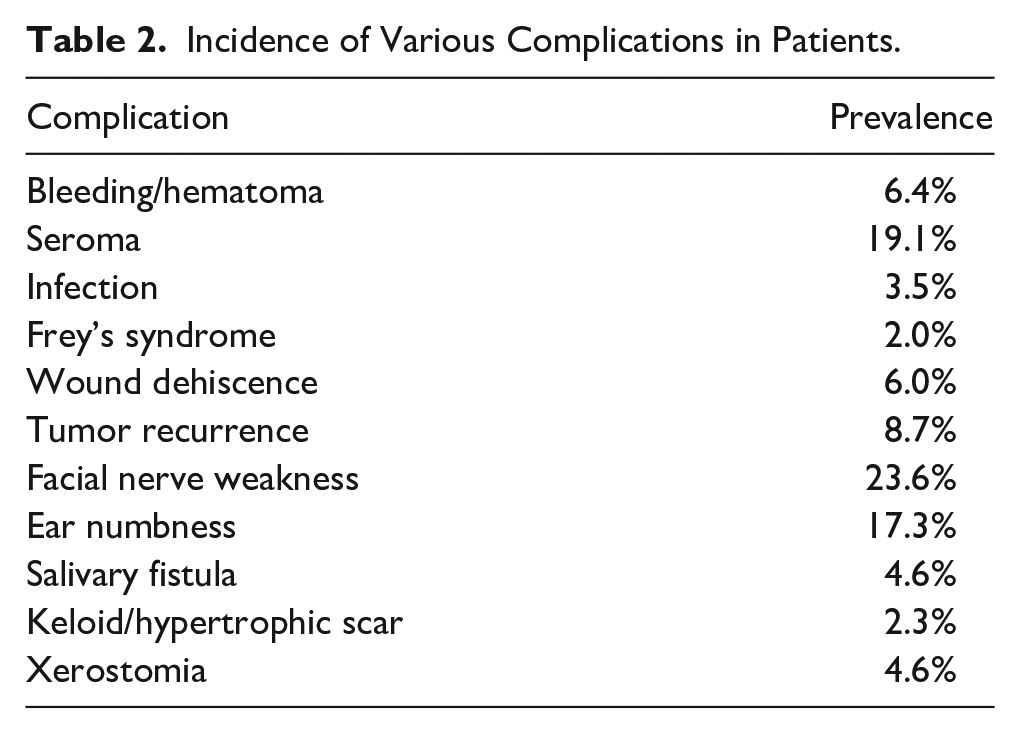
Table 2 presents the incidence of various complications in patients undergoing parotidectomy. The incidence rates indicate the approximate percentage of patients who experienced each complication. Facial nerve weakness was observed in 41 patients (23.6%), but most of them were grade 2 (n = 26, 15.0%), and the most common nerve involved was the marginal mandibular nerve (n = 26/41). Out of all facial nerve weakness cases, 26 (63.4%) of them completely recovered on follow-up.
Incidence of Various Complications in Patients.
Associations of Various Factors With Complications
Table 3 highlights the relationship between various variables and complications. Regarding smoking, no statistically significant association was found between smoking and any of the complications, except for a potential association with xerostomia. More invasive type of surgery showed a significant association with surgical site infection, indicating that the specific surgical procedure performed may influence the probability of experiencing these complications. Moreover, an unexpected correlation was noted between a more invasive type of surgery and tumor recurrence, likely to be attributed to the characteristics of the illness rather than the operation itself.
Association of Different Factors With Complications.
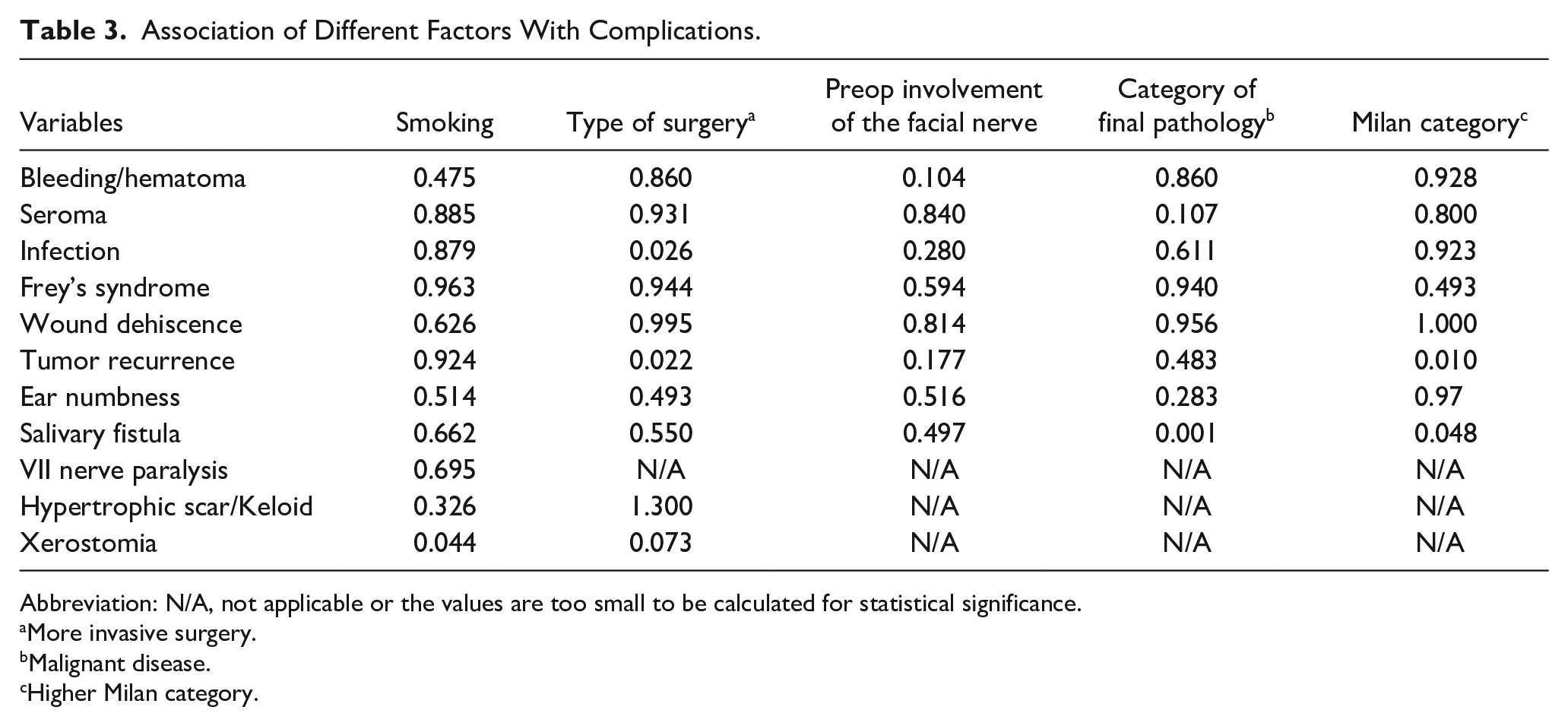
Abbreviation: N/A, not applicable or the values are too small to be calculated for statistical significance.
More invasive surgery.
Malignant disease.
Higher Milan category.
No significant associations were found between preoperative facial nerve involvement and any of the complications. The category of final pathology (nonneoplastic, benign, or malignant) did not show significant associations with most of the complications. However, there was a notable association between malignant disease on the final pathology and salivary fistula, suggesting that the pathological characteristics of the tumor may influence the occurrence of this complication. The Milan category was associated with tumor recurrence and salivary fistula.
Association of BMI and Age With Complications
Correlation analyses were performed to evaluate the associations of BMI and age with complications. The correlation analysis between age and complications showed no significant associations. Similarly, no significant correlations were found between BMI and complications. These results suggest that age and BMI do not have a strong linear relationship with the occurrence of the listed complications (Table 4).
Correlation Analysis.
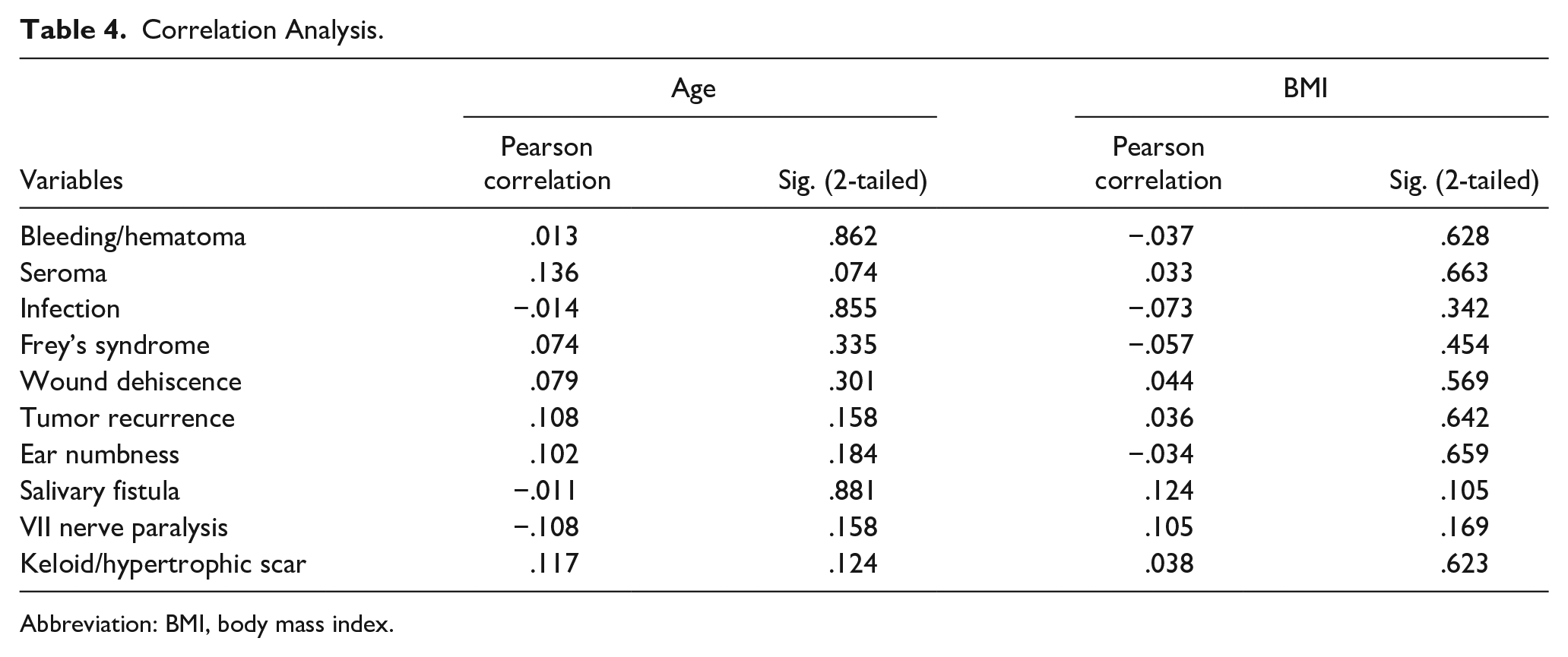
Abbreviation: BMI, body mass index.
Discussion
The purpose of the present study was to investigate various factors associated with postoperative complications following parotidectomy. Our findings showed that facial weakness was the most common complication followed by seroma and ear numbness, in line with previous studies that showed facial weakness with an incidence ranging from 9.2% to 66 %.24,25 Seroma formation is a common occurrence after surgery and can be due to the accumulation of fluid at the surgical site. However, the incidence of seroma was much higher in the present study compared to previous studies. A study by Coniglio et al 26 reported that seroma incidence was 9.5% in patients who underwent drainless parotidectomy and 3.8% in drained patients. Similarly, another study by Nielsen et al 27 reported that 5.8% of the patients developed seroma after undergoing parotidectomy. Our findings also contrasted with those of Ruohoalho et al, 28 who observed that 6.1% of patients developed seroma after surgery. In the present study, we did not differentiate between drained and drainless approaches in parotidectomy. Some authors suggest that drainage avoids complications like seromas and hematomas.17,29 However, even after drainage, almost 2.4% developed hematomas and 4.2% had seroma complications in previous studies.17,29 In addition, drainage can also increase the risk of infection and salivary fistula, as it exposes the underlying tissues to pathogens.17,28,30
In our study, Frey syndrome was observed in 2% of the patients. Our findings are consistent with those of Ruohoalho et al, 28 who reported that 3% of their patients developed Frey syndrome after parotidectomy. However, a much higher incidence of Frey syndrome has also been reported in the literature. A study that included 372 patients reported that 23.5% of patients developed Frey syndrome 1 year after parotidectomy. 31 Furthermore, they revealed that almost half of these patients were symptomatic. 31 However, our findings are supported by a large study that involved 610 surgical cases. In another study, only 4% of the patients developed Frey syndrome. 21 Some studies have also tried to identify various predictors of Frey syndrome after parotidectomy. A study by Lee et al 23 reported that tumor size is a significant predictor of the development of Frey syndrome, while the type of resection, previous treatment, or pathology of the disease were not found to be significant predictors.
In our study, ear numbness was the third most common complication (17.3%). A study by Al-Mazrou 32 found that 14% of their patients developed ear numbness. Similarly, an incidence of 20% was reported in another study. 33 In a different study, only 1 in 8 patients developed ear numbness. 34 Although ear numbness can be attributed to surgical manipulation of the auriculotemporal nerve during the procedure, 35 it is important for clinicians to inform patients about the potential for sensory disturbances and provide appropriate counseling to manage this complication.
Studies that focused on the association between various variables and complications provide information on potential risk factors that might contribute to the development of postoperative problems. Smoking, al-though not showing significant associations with most complications, showed a potential link with xerostomia. These findings are also supported by previous studies. For example, a study reported that 39% of smokers and 12% of smokers developed xerostomia. 36 Furthermore, that study found a significant association between the 2 variables. 36
More invasive types of surgery (partial < superficial < total) emerged as a significant factor that influenced surgical site infection. Furthermore, the study revealed an inconsistent link with tumor recurrence, perhaps due to the use of invasive surgical procedures for aggressive diseases, which acts as a confounding factor. Two previous studies have shown no significant increase in recurrence rates between partial and complete superficial parotidectomy.37,38 Other factors, such as final pathology, demonstrated an interesting association with salivary fistula, hinting at the interplay between tumor characteristics and complications. However, a previous study by Britt et al 39 found no association between tumor pathology and salivary fistula. Similarly, higher Milan category showed a significant association with tumor recurrence indicating that disease severity might play a role in shaping postoperative outcomes.
Conclusion
The present study sheds light on various factors associated with postoperative complications in patients who underwent parotidectomy. In this study, seroma was identified as the most common complication followed by ear numbness and tumor recurrence. Although some complications showed significant associations with certain variables, others did not show strong connections. Smoking did not show statistically significant associations with most complications, except for a possible link to xerostomia. More invasive type surgery demonstrated a significant association with surgical site infection. Preoperative involvement of the facial nerve did not show significant associations with complications. However, malignant disease of final pathology showed a notable association with salivary fistula and recurrence, suggesting that tumor characteristics may contribute to the appearance of this complication. A correlation analysis revealed that neither age nor BMI exhibited significant linear relationships with the occurrence of complications. The study highlights the importance of understanding patient-specific characteristics, surgical techniques, and tumor pathology in predicting and managing complications. Healthcare professionals should consider these findings and tailor their approach to minimize the occurrence of complications. More research and larger-scale studies may help validate these associations and provide even more comprehensive insights.
Footnotes
Acknowledgements
No further acknowledgments to be declared.
Authors’ Note
This article has not been previously published and is not under consideration in the same or substantially similar form in any other peer reviewed media.
Author Contributions
All authors have an essential contribution to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in King Fahad Medical city in Riyadh, Saudi Arabia, and was approved by the Ethics Committee Institutional Review Board Log Number: 23-239 on May 10, 2023, with an exemption from informed consent. No specific consent is needed for statistical analyses of aggregated deidentified data. For this study, the raw data were first extracted from HIS, and patients’ identities, including names, screening IDs, patient IDs, and mobile phone numbers, were de-identified.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because no personal or identifiable information/images submitted in this article.
Data Availability
Data in this article were obtained from King Fahad Medical City Registry in Riyadh, Saudi Arabia