
Abstract
Cholesteatomas are benign growths of squamous epithelial tissue in the middle ear resulting in conductive hearing loss and/or erosion of the structures of the middle ear space. These lesions are surgically removed but require postoperative surveillance due to risk of recurrence or residual disease. Second-look surgery remains the gold standard for diagnosis and treatment of residual or recurrent cholesteatoma; however, advanced imaging modalities such as non-echoplanar diffusion weighted magnetic resonance imaging (non-EPI DWI-MRI) offer a less invasive alternative for surveillance. As surgeons become more reliant on advanced imaging, it is important to understand the limitations of the technology. We present a case of a delay in diagnosis of residual cholesteatoma due to a false-negative finding on non-EPI DWI-MRI screening in the presence of a titanium implant.
Introduction
Cholesteatoma commonly results in the loss of middle ear ossicles through erosion or surgical removal. After surgery for cholesteatoma, long-term surveillance is necessary because residual or recurrent disease often grows slowly and may not cause symptoms for years. Focal residual cholesteatoma behind an opaque cartilage graft or in the mastoid may not be clinically evident. Historically, second-look surgeries were often necessary to identify and treat residual disease. Modern surveillance protocols often include computed tomography (CT) scan or magnetic resonance imaging (MRI). Although CT is a valuable tool for imaging the temporal bone, it cannot differentiate cholesteatoma from fluid, mucosal edema, scar tissue, or cartilage grafts. MRI is better able to differentiate among these soft tissues and avoids the radiation of CT, so it has become the primary tool for surveillance for many otologists. MRI sequences commonly described for cholesteatoma identification include “non-echoplanar (non-EPI) diffusion weighted imaging (DWI), PROPELLER sequence, HASTE sequence, RESOLVE sequence, and Spin Echo.” Benefits of this shift include reduction in surgical risk and patient cost. Recent studies use negative findings on non-EPI DWI-MRI and second-look surgery as equivalent outcomes for nonrecurrence of cholesteatoma.1,2
The 2 most recent systematic reviews of adult and pediatric DWI-MRI screening for recurrent cholesteatoma reveal consistent findings of increased sensitivity using non-EPI sequencing. In the adult study, non-EPI DWI-MRI demonstrated a sensitivity of 89.7%, specificity of 94.6%, positive predictive value (PPV) of 96.5%, and negative predictive value (NPV) of 80.5%, surpassing the sensitivity of EPI DWI-MRI [71.8 (P = .02)]. Confirmatory tests for diagnosis involved second-look surgery. Results showed no discernible trend in the size of lesions missed by non-EPI DWI-MRI. 3 The authors suggest that non-EPI DWI-MRI could serve as a viable alternative to second-look surgery in centers with specific expertise. Similarly, the most recent pediatric review found that non-EPI DWI-MRI exhibited a pooled sensitivity of 89% and specificity of 93%, while the combination of EPI and non-EPI DWI-MRI showed a pooled sensitivity of 84% and specificity of 92%. There was a noted potential reduction in sensitivity for detecting lesions below 3 mm. 4 Despite these results, the authors cautioned against replacing second-look surgery in children. One author recommended delaying screening until 12 months post operation to ensure the recurrent cholesteatoma reaches a sufficient size for accurate detection. 5
A literature search shows a single study discussing the limitations of DWI-MRI in cholesteatoma surveillance after reconstruction. In the study, postoperative patients with titanium prosthesis, autologous cortical bone columella, and no reconstruction of hearing bones were compared. Non-EPI DWI-MRI was used with PROPELLER sequence. Imaging of patients with titanium prosthesis showed greater sensitivity, PPV, and NPV than imaging of patients with autologous cortical bone columella. Note that each group contained a low number of cases (9, 9, 10). 6 Authors advocate for use of DWI-MRI for postoperative screening, but second-look surgery for those with bony columella.
A review of the literature demonstrates good evidence for the precision and accuracy of non-EPI DWI-MRI as a screening tool for recurrent or residual cholesteatoma. However, there is limited evidence regarding the use of these screening tools in patients with specific types of implants and in pediatric populations.
Case Report
A 6-year-old otherwise healthy male presented to otolaryngology clinic with history of Eustachian tube dysfunction, prior myringotomy tubes, and inconsistent left ear purulent otorrhea for 2 years. Audiogram showed normal right-sided hearing and near-maximal conductive hearing loss on the left side. Microscopic examination of the left side revealed a retraction pocket containing squamous debris consistent with cholesteatoma. The parents and physician agreed on a plan for a second-stage tympanoplasty and mastoidectomy.
Preoperative CT scan revealed opacification of mastoid and middle ear with demineralization of the long process of the incus.
In the first stage, cholesteatoma debris filled the middle ear space, completely eroding the long process of the incus. The surgeon preformed an underlay tympanoplasty with temporalis facia graft. Given the extent of disease, the ossicular chain was left in discontinuity for a planned second-look procedure.
In the second stage, 11 months after initial operation, dissection of the middle ear identified and removed 2 foci of cholesteatoma from the anterior crus of the stapes and the cochlear promontory. The surgeon conducted a tragal cartilage graft tympanoplasty and ossicular chain reconstruction (OCR) using a 3.5 mm titanium Kurz Variac partial ossicular reconstructive prosthesis (PORP). A tympanostomy tube was also placed at the second-stage procedure. Postoperative course was uncomplicated. Three months after the second-stage procedure with OCR, otoendoscopy showed a well-positioned cartilage graft and early partial extrusion of the tympanostomy tube (Figure 1A). Audiogram showed marked improvement in hearing with near-complete closure of the air-bone gap.
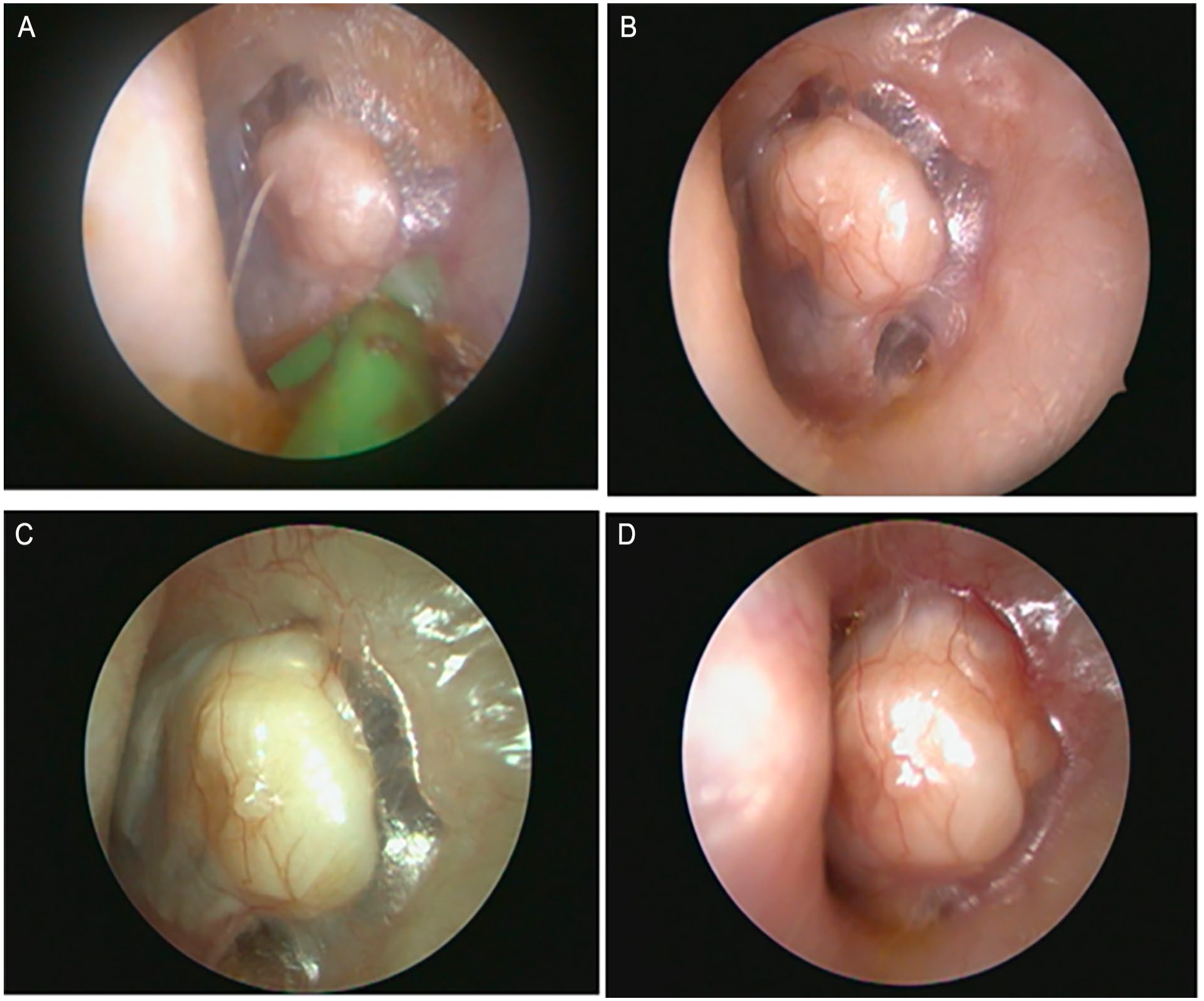
(A-D) Otoendoscopic surveillance photos 3 months, 1 year, 2 years, and 3 years after second stage with OCR. Note mass effect and increasing pallor of the tympanic membrane. MRI performed at 2 years (C); CT performed at 3 years (D). OCR, ossicular chain reconstruction; MRI, magnetic resonance imaging; CT, computed tomography.
The patient returned for regular office visits including endoscopic photo-documentation of the tympanic membrane (Figure 1B). Two years after the second-stage procedure with OCR, serial examination raised concern for an enlarging area of pallor adjacent to the cartilage graft (Figure 1C). A screening non-EPI DWI-MRI with RESOLVE sequence showed no restricted diffusion and no evidence of cholesteatoma (Figure 2A). Concurrent T1 MRI showed the implant correctly positioned in the middle ear with possible soft tissue changes (Figure 2B). In the context of a negative non-EPI DWI-MRI, regrowth of residual cholesteatoma was not definite. An audiogram showed slight interval worsening of hearing at high frequencies, but hearing remained acceptable and nonlimiting, and the patient remained asymptomatic. After an informed discussion, the parents and senior author chose to continue observation.
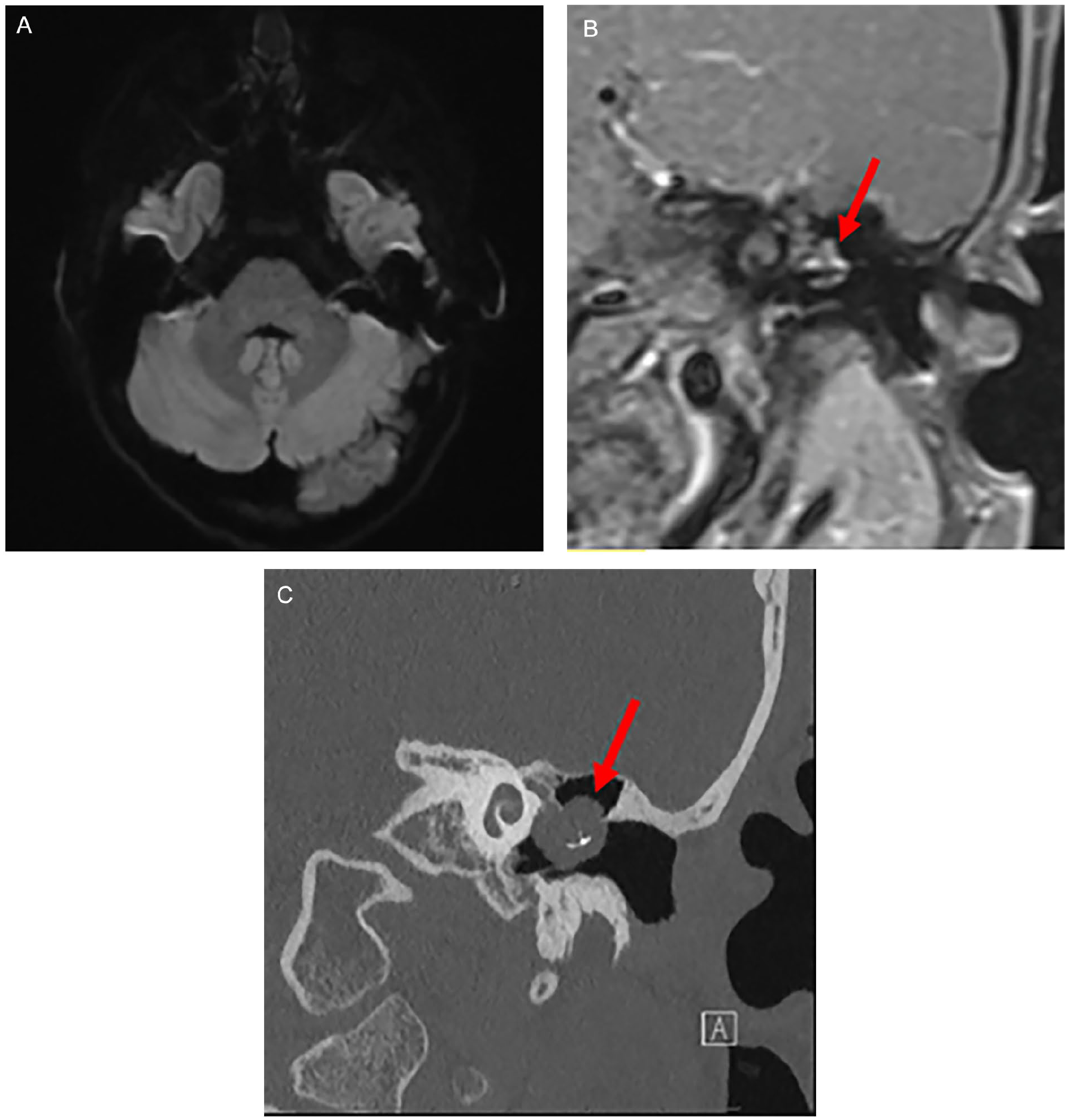
(A) Coronal non-EPI DWI-MRI with RESOLVE sequence 2 years after second stage with OCR shows no restricted diffusion. Because of the titanium imbedded within the cholesteatoma, this mass did not exhibit signal characteristic of cholesteatoma on the DWI RESOLVE sequence. (B) Coronal MRI T1 FS Thin w/ contrast 2 years after second stage with OCR shows the presence of the bright mass (now known to be cholesteatoma) which measures 7.5 mm in diameter and encases the prosthesis (appears as dark, upside-down “T”). (C) Coronal CT of left middle ear taken 3 years after second stage with OCR shows the mass which measures 1.0 cm in diameter with titanium implant encased within cholesteatoma. MRI, magnetic resonance imaging; EPI, echoplanar imaging; DWI, diffusion weighted imaging; T1 FS Thin, T1 weighted fat supressed image; OCR, ossicular chain reconstruction; CT, computed tomography.
Three years after the second-stage procedure with OCR, the previously noted peripheral pallor further increased in size to become an obvious white mass bulging beneath the cartilage graft (Figure 1D). CT imaging showed a 1.0 cm round, soft tissue mass encasing the prosthesis (Figure 2C).
Surgical exposure revealed a large cholesteatoma filling middle ear with encasement and displacement of the PORP and erosion of the stapes suprastructure. The surgeon resected the cholesteatoma and reconstructed with a total ossicular reconstructive prosthesis. The patient had an uneventful postoperative course and remains in regular follow-up with ongoing otoendoscopic and radiographic surveillance.
The authors have attained written informed consent from the patient and guardian for the aforementioned case and associated images to be published.
Discussion
While the gold standard for screening of recurrent and residual cholesteatomas remains second-look surgery, recent literature demonstrates that the use of non-EPI DWI-MRI as an equivalent screening tool. However, there exists limited research on the NPV of non-EPI DWI-MRI in the context of different ossicular chain prosthesis materials.
Our case demonstrates that, although titanium is an MRI compatible material, the presence of titanium within or near cholesteatoma may reduce the NPV of MRI as a screening tool. This case points to the need for research evaluating different MRI sequences in the context of different ossicular chain prosthesis materials.
It is important for surgeons and neuroradiologists to be aware that a negative result should be interpreted with caution if the patient has a titanium prosthesis. With currently available imaging, second-look surgery may be indicated under these conditions, even in the presence of a negative result on MRI. While this patient had both a staged second-look procedure and an MRI, photographic documentation of progression of pallor over years ultimately informed diagnosis and decision-making. This case highlights the importance of regular office surveillance, potential limitations of non-EPI DWI-MRI, and the utility of photo-documentation with otoendoscopy for postoperative cholesteatoma screening. Additional research in both adults and children is necessary to better inform screening for recurrent cholesteatomas in the context of ossicular chain prosthesis.
Footnotes
Data Availability
No new data were generated or analyzed during this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Dartmouth Hitchcock Institutional Review Board (DH-IRB) has reviewed and approved this research. DH-IRB has determined that this case report is not research involving human subjects as defined by Department of Health and Human Services and Food and Drug Administration regulations (March 7, 2023).
Informed Consent
The authors have attained written informed consent from the patient and guardian for the aforementioned case and associated images to be published.