
Abstract
Vascular variations are prevalent among the human population. However, the occurrence of anatomical variations in the inferior thyroid artery originating directly from the brachiocephalic trunk (BCT) is exceptionally rare, as confirmed by numerous research studies. In addition, reliable departmental statistics reveal that the incidence rate of retrosternal goiter is approximately 19%. In this case study, the variation blood vessels in the neck were accidentally found and analyzed. Simultaneously, we conducted an analysis on the clinical significance of a rare anatomical variation. The study focused on a 60-year-old female patient who underwent a surgery for retrosternal goiter, during which it was discovered that the inferior thyroid artery originated from the BCT. Our report presented a unique case involving this particular combination of anatomical variations within the BCT. The anatomical variation reported in our study will effectively reduce the risk of patients and enhance our comprehension of this anatomy’s characteristics, thereby avoiding the occurrence of iatrogenic complications.
Introduction
As commonly understood, the brachiocephalic trunk (BCT) typically originates from the aortic arch, serving as its largest branch. 1 Its primary function is to supply blood to the right head, face, and upper right arm. In addition, the BCT typically follows an oblique course toward the upper right region, situated posterior to the right sternoclavicular joint, where it divides into the right common carotid artery (RCCA) and the right subclavian artery. 2 Nevertheless, the left common carotid artery and the left subclavian artery originate from the aortic arch, respectively. In the past, there have been limited reports by researchers on the variation of the anatomical position of the BCT.3,4 Especially, the case that the inferior thyroid artery originated directly from the BCT is rare. When performing thyroid tumor surgery, tracheostomy, and parathyroid surgery, we are generally surprised by the phenomenon of anatomical variation.5-7 Therefore, thorough understanding of these variations can effectively ensure the safety of surgery and reduce the risk of hemorrhage.
Case Presentation
A 60-year-old female patient with no previous history of specific diseases often felt uncomfortable in her neck over the past year. A computed tomography scan of her neck (depicted in Figure 1) revealed a significant enlargement of the retrosternal goiter, extending beyond both the sternocleidomastoid muscles and the upper mediastinum extension causing clinical symptoms of neck discomfort in patients. Furthermore, the results of ultrasound showed diffuse goiter and multiple nodules. Taking into account the patient’s clinical manifestations, we hypothesized that the patient was suffering from a retrosternal goiter and accordingly a thyroidectomy was promptly scheduled.

CT images of the appearance of retrosternal goiter. (A) Sagittal section, (B) coronal section, and (C) transverse section. CT, computed tomography.
We used tight silk thread to delicately create an arcuate incision, approximately 6 cm in length, along the dermatoglyphic direction at the superior border of sternal notch about 2 cm, until the thyroid gland was thoroughly exposed. Inspection revealed that the retrosternal extension of the goiter was situated on the right side, measuring about 8 cm in length, 6 cm in width and 4 cm in thickness. Then, silk thread was used to ligate the superior thyroid artery and middle thyroid vein, thereby completely separating the superior thyroid pole. While carefully separating the lower thyroid pole, we accidentally discovered an anatomical variation of the BCT.
More specifically, our team of surgeons meticulously exposed the inferior thyroid artery, which exhibited a diameter of approximately 0.5 cm and originated directly from the BCT. The distance between inferior thyroid artery and aortic arch was about 1.5 cm. The inferior thyroid artery originating from the BCT was approximately 2 cm long and divided into 2 branches to supply blood for the thyroid gland (middle and lower; Figure 2). We should put great emphasis on the harm caused to patient’s life and the risk of hemorrhage caused by anatomical variations due to lack of investigation of the anatomical variation preoperatively.
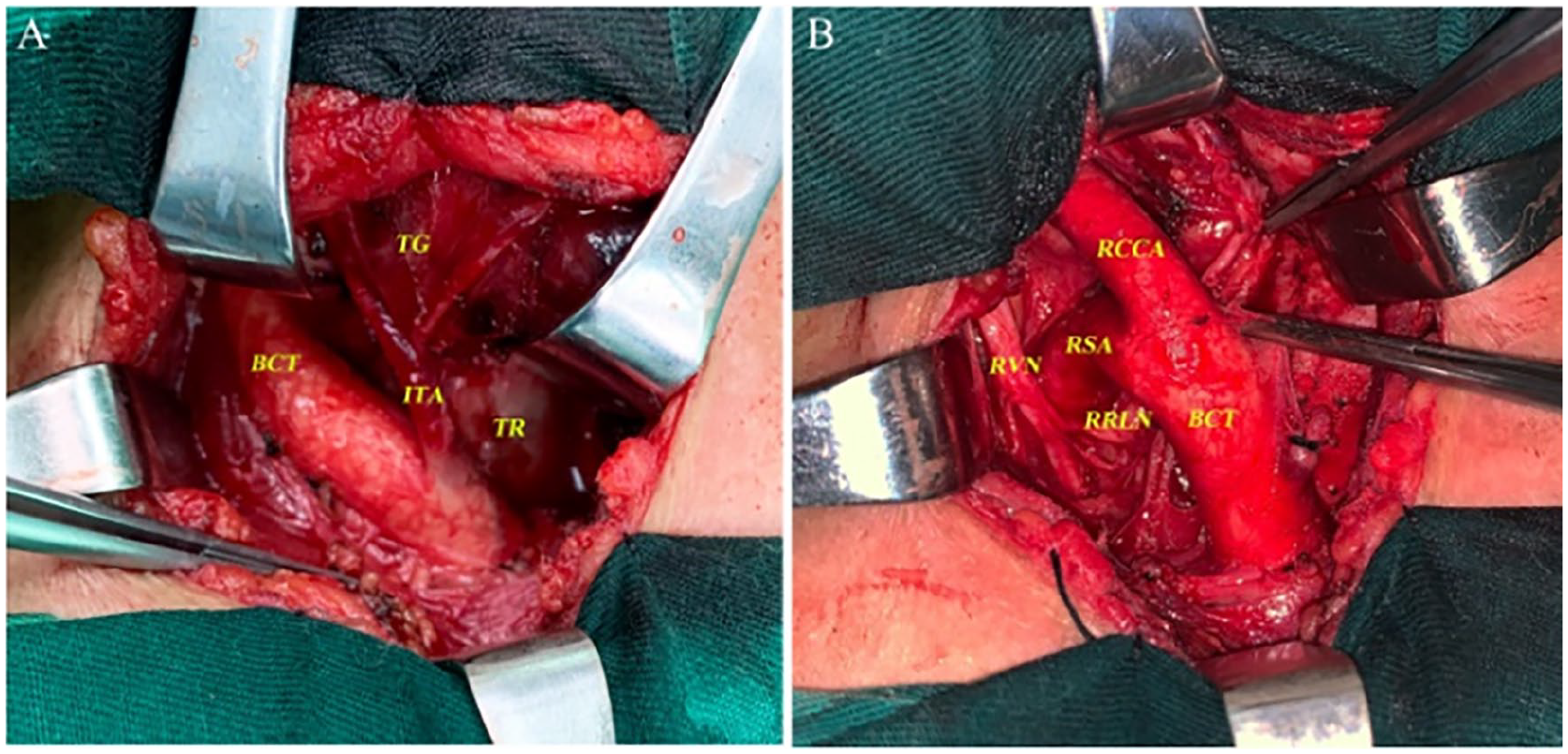
Intraoperative images showed that the ITA arose from the BCT (A and B). ITA, inferior thyroid artery; BCT, brachiocephalic trunk; TG, thyroid gland; TR, trachea; RVN, right vague nerve; RSA, right subclavian artery; RRLN, right recurrent laryngeal nerve; RCCA, right common carotid artery.
The surgeon successfully excised the retrosternal goiter (weight: 150 g), and the intraoperative blood loss was about 20 mL (Figure 3A). Moreover, the postoperative conscious patient had clear pronunciation without any adverse complications. Two days after surgery, the patient’s drainage tube was removed. Meanwhile, the pathology of the resected samples showed that the diagnosis of nodular goiter included local calcification, but no malignant component was found in the tissues or lymph nodes (Figure 3B). The patient has been approved to leave the hospital on the third day after surgery, as her blood routine, parathyroid hormone, and calcium levels were within normal range.
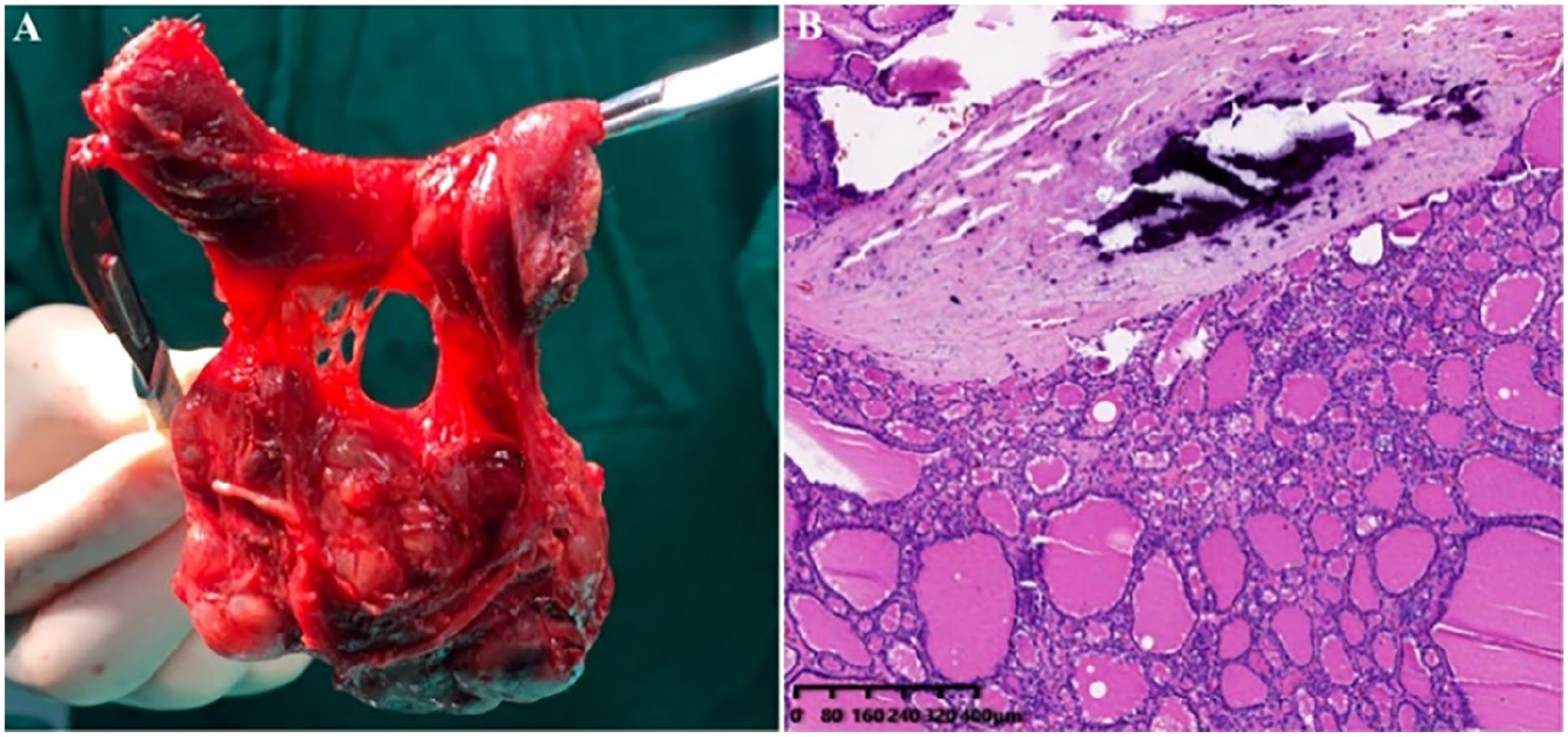
Macroscopic appearance of the retrosternal goiter after removal (A). Its microscopic morphology was analyzed (B).
Discussion
Vascular variation has become more and more popular worldwide due to its high occurrence. Many scientists have shown that most of the inferior thyroid arteries originate from the thyrocervical trunk and subclavian, but few originate from the BCT, aortic arch, common carotid artery, or other parts. 8 Thus, the inferior thyroid artery directly originating from the BCT we reported in this article is very rare and worth learning and presenting.
A severe hemorrhage risk during operation can be caused by the anatomical variation BCT, which could even endanger people’s lives. 9 Meanwhile, it also has important clinical value for thyroid surgery. 7 If surgeons are not familiar with the anatomical variations of important neck vessels, it is easy to cause accidental arterial hemorrhage and recurrent laryngeal nerve injury.
Globally, there have been reports of relevant articles related to anatomical variation.10,11 Lovasova et al 4 discovered a rare vascular variation during the dissection of an adult female cadaver. The middle thyroid artery and aberrant accessory inferior thyroid artery were observed to originate from the RCCA, while the thyroid artery originated from the BCT. In this case, we discovered an anatomical variation of the inferior thyroid artery that originated from the BCT. The vascular variation from the BCT may be attributed to the continuous extension and transformation of the artery during embryonic development, and then the degenerated and fused vascular can replace the blood supply of thyroid blood.
In addition, the change of hemodynamics also has certain influence on the incidence of retrosternal goiter. In our case, the surgeons observed that the contralateral thyroid artery was normal, and its blood vessel size was obviously smaller than that of the affected thyroid artery. Concurrently, the affected thyroid artery exhibited significant enlargement and thickening. We analyzed that the inferior thyroid artery originating from the BCT possessed high blood volume and high arterial pressure, thereby promoting and potentially inducing the occurrence of retrosternal goiter.
Conclusions
Senior surgeons may encounter the anatomical variation of BCT in neck-related surgery, and this surprising discovery can pose serious risks. Specifically, serious surgical complications may lead to massive hemorrhage and even life-threatening outcomes. Therefore, we unanimously believe that surgeons possessing robust medical theoretical foundation and superior surgical skills can provide safety and reliability for the health of patients.
Footnotes
Data Availability
All data generated or analyzed during this study are included in this published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case was obtained from the ethical committee of Guangdong Second Provincial General Hospital.
Informed Consent
Written informed consent was obtained from the patient for the publication of this case report.