
Abstract
Introduction
Upper airway obstruction (UAO) is the most common life-threatening condition in ear, nose, and throat (ENT) patients. The most likely causes are tumor, tracheal stenosis, or severe obstructive sleep apnea.1,2
A study reported that the incidence of UAO patients who underwent emergency tracheostomy is related to male sex, obesity, and smoking.3,4 The anesthetic technique for emergency tracheostomy could range from monitored anesthesia care (MAC) to general anesthesia. The determination of the appropriate technique hinges on the prevailing conditions and the degree of patient cooperation, as well as the assessed risks associated with challenges in ventilation and intubation procedures.3,5,6 Tracheostomy may need to be operated under MAC with local anesthesia in patients with a high risk of difficult ventilation and intubation. 6 On the other hand, mild sedation can help ease anxiety in patients with low risk of a difficult airway. 3 In addition, surgical procedures that require airway sharing are quite a challenge for anesthesiologists. Communication between anesthesiologists and surgeons is much needed in these circumstances to minimize the risk of complications. 7
The incidence of complications from emergency tracheostomy included bleeding, surgical site infection, pneumothorax, subcutaneous emphysema, pulmonary edema, inability to perform tracheostomy, tube dislodgement, tube displacement, and death.2-5,8-10 Complications could occur during the intraoperative, early, and late postoperative period with an overall incidence of 5.6% to 15.6%.8-10 However, any complications affect patients physically and mentally and also increase hospital costs.
There were reports on complications of the tracheostomy procedure, mainly a surgically related complication.2-5,8-12 However, the anesthetic technique involved in the procedures was least mentioned earlier.8,13 The objective of this study is to report the incidence of early and intraoperative complications (in 7 days) of both anesthetic and surgical causes, in patients who underwent an emergency tracheostomy. The second objective was to determine factors associated with perioperative complications.
Materials and Methods
This retrospective study was approved by the Siriraj Institutional Review Board, Siriraj Hospital Faculty of Medicine, Mahidol University, Bangkok, Thailand (Si 880/2021). Inpatient anesthetic and surgical records were then examined in detail to identify patients aged 18 years or older who had undergone an emergency tracheostomy performed by ENT surgeons between January 2013 and October 2021. Exclusion criteria included intubated patients, percutaneous tracheostomy, and cases involving conversion tracheostomies from previous cricothyroidotomies or tracheostomy procedures performed to facilitate other surgical interventions. The parameters analyzed included demographic data, cause of airway obstruction, sign and symptoms, anesthetic technique, perioperative and early postoperative complications (see the Supplemental Appendix for the definition of complications), and clinical results at 7 days postoperative.
The anesthetic report of each patient was reviewed to confirm the details of an emergency tracheostomy. The anesthesia protocol included standard monitoring; pulse oximeter, an electrocardiogram, and noninvasive blood pressure were used before anesthesia was administered. The choice of anesthetic technique depended on the patient’s condition such as hemodynamic, oxygenation, and level of consciousness. If the patient had unstable hemodynamics, desaturation despite oxygen support, or a change in consciousness level, it was likely that tracheostomy would be performed under local anesthesia and MAC. During this technique, patient cooperation and ability to lie supine were crucial for the operation. Analgesia such as fentanyl can be administered to reduce pain from the procedure and help soothe patients. If the patient is stable enough without anticipated difficulties in airway management, general anesthesia with muscle relaxants is generally employed. However, in cases involving a full stomach, the need for rapid sequence induction must be carefully assessed, balancing the imperative of swift intubation against the risks associated with difficult intubation. In the event of a possible difficult airway, ENT surgeons and anesthesiologists would discuss and make a decision about the airway management steps and alternative plans. Regarding the intubation technique, the choice of awake intubation versus intubation after induction depended on the ability to provide adequate ventilation. In a difficult intubation scenario, a laryngeal mask airway was used as an adjunct device to help ventilation. Extracorporeal membrane oxygenation may play a role in higher-grade airway obstruction that cannot be ventilated and cannot be intubated. 14 Fiberoptic bronchoscopy, video laryngoscopy, conventional laryngoscopy, or direct laryngoscopy were used to manipulate intubation. After successful ventilation or intubation, the surgeons performed a tracheostomy under general anesthesia.
After the tracheostomy was performed, the patient was ventilated through the tracheostomy tube with end-tidal CO2 monitoring to ensure definite airway access. Complications during intraoperative, immediate postoperative, and also outcomes at 7 days postoperatively were recorded. Complete recovery was defined as the ability to breathe normally through a tracheostomy in the postoperative period without ventilatory support or leading to unplanned intensive care unit (ICU) admission. For unstable hemodynamics, we defined as hypotension or hypertension that needed medication.
Sample Size Calculation and Statistical Analysis
The sample size was calculated using nQuery under the assumption of a 15.6% incidence of complications in patients undergoing an emergency tracheostomy. 10 Therefore, 250 patients were needed to achieve a 95% confidence interval (CI) with a 4.5% error margin. Statistical analyses were performed using IBM SPSS Statistics (version 29; IBM Corp). The demographic data of the participants, the cause of airway obstruction, sign and symptoms, anesthetic technique, perioperative and early postoperative complications, and clinical evolution were analyzed using descriptive statistics. Categorical data were compared using the Chi-square test or Fisher’s exact test, and the results are given as number and percentage. Continuous data were compared using the 2-sample T test for normally distributed data (results shown as mean ± standard deviation) and using the Mann-Whitney U test for nonnormally distributed data (results shown as median and range; minimum, maximum). The variables evaluated with a P < .10 in the univariate analysis were entered into the multivariate analysis to identify independent factors related to unstable hemodynamics. The results of the univariate and multivariate analyses are presented as crude and adjusted odds ratios (ORs), respectively, and their respective 95% CIs. A P < .05 was considered statistically significant for all tests.
Results
Between January 2013 and December 2021, there were 255 cases of emergency tracheostomy. Two cases were excluded due to incomplete data. A total of 253 patients who underwent an emergency tracheostomy were included in the final analysis.
Demographic and anesthetic data are demonstrated in Table 1. Malignancy was the leading cause of UAO that requires an emergency tracheostomy with male predominate. Hypertension was the most associated comorbid disease. Supraglottic malignancy was found to be the leading cause of emergency tracheostomy in 108 patients (42.6%), followed by bilateral paralysis of the vocal cord in 30 patients (11.9%), and glottis malignancy with bilateral paralysis of the vocal cord in 27 patients (10.7%), respectively. The other causes of emergency tracheostomy, such as subglottic stenosis, transglottic malignancy, thyroid mass, esophageal cancer, lymphoma, and corrosive ingestion, were summed up in 67 patients (26.5%). There were 57 patients (22.5%) with a history of radiation therapy at the neck and 202 patients (79.8%) who had a lesion at the neck. Most patients had no contact bleeding at the lesion (238 patients, 94.1%). The prevalence of patients with a history of smoking and alcohol use were 66.9% (170 patients) and 56.7% (144 patients), respectively. There were 108 patients (42.7%) who were unable to lie supine and 121 patients (47.8%) who needed oxygen support before being transferred to the operating room with a mean oxygen saturation of 98.0% ± 2.0%.
Demographic Data of the Study Population and Anesthetic Details.
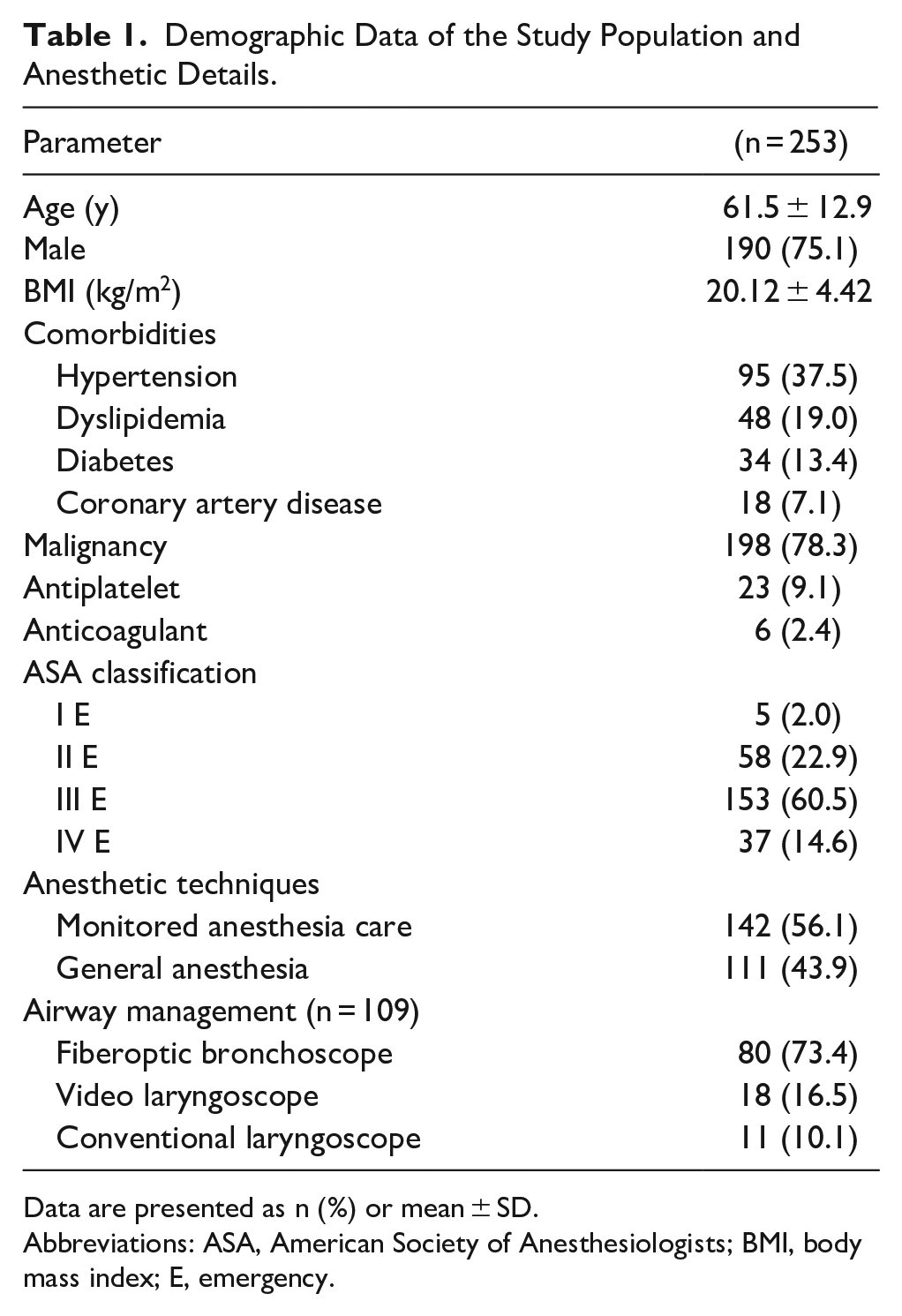
Data are presented as n (%) or mean ± SD.
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; E, emergency.
The perioperative complications and outcomes are shown in Table 2. In total, 131 patients (51.8%) had intraoperative complications. There was no intraoperative death. Two patients, their underlying conditions progressed and need end-of-life care at home 7 days postoperatively. Another patient developed left-sided heart failure with volume overload on which ventilatory support was required.
Perioperative Complications and Outcomes.
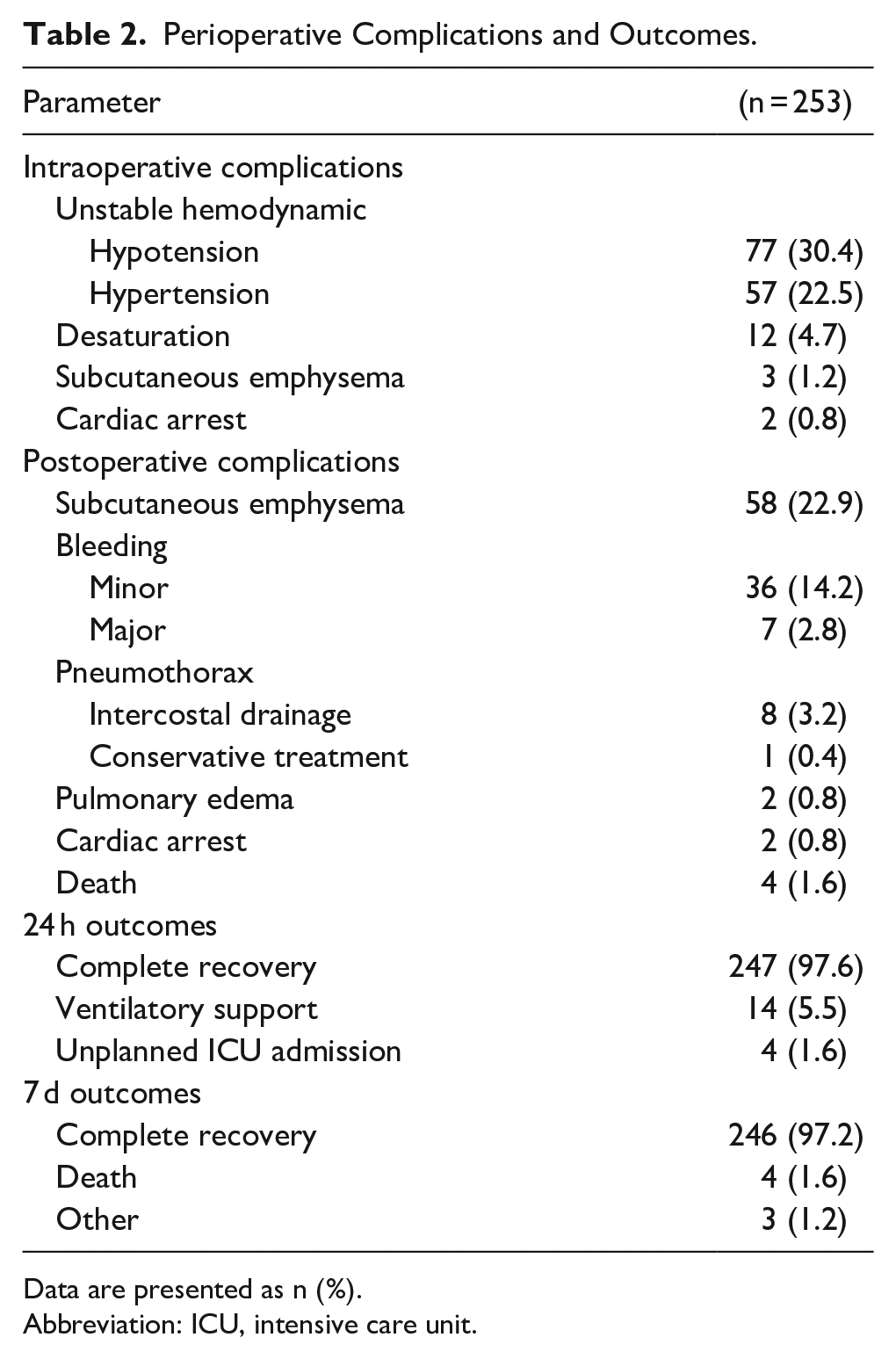
Data are presented as n (%).
Abbreviation: ICU, intensive care unit.
Unstable hemodynamics was found in 52.9% of the patients. Risk factors that had a P value <.1 were the American Society of Anesthesiologists classification, hypertension as a comorbid disease, the MAC technique, and intraoperative fentanyl less than 1 µg/kg/hour (Table 3).
Multivariate analysis revealed that MAC (adjusted OR = 1.80; 95% CI: 1.08-3.00) and hypertensive patients (adjusted OR = 1.70, 95% CI: 1.01-2.86) were associated with unstable intraoperative hemodynamics (Table 3).
Univariate and Multivariate Analysis of Factors Associated With Intraoperative Unstable Hemodynamics.
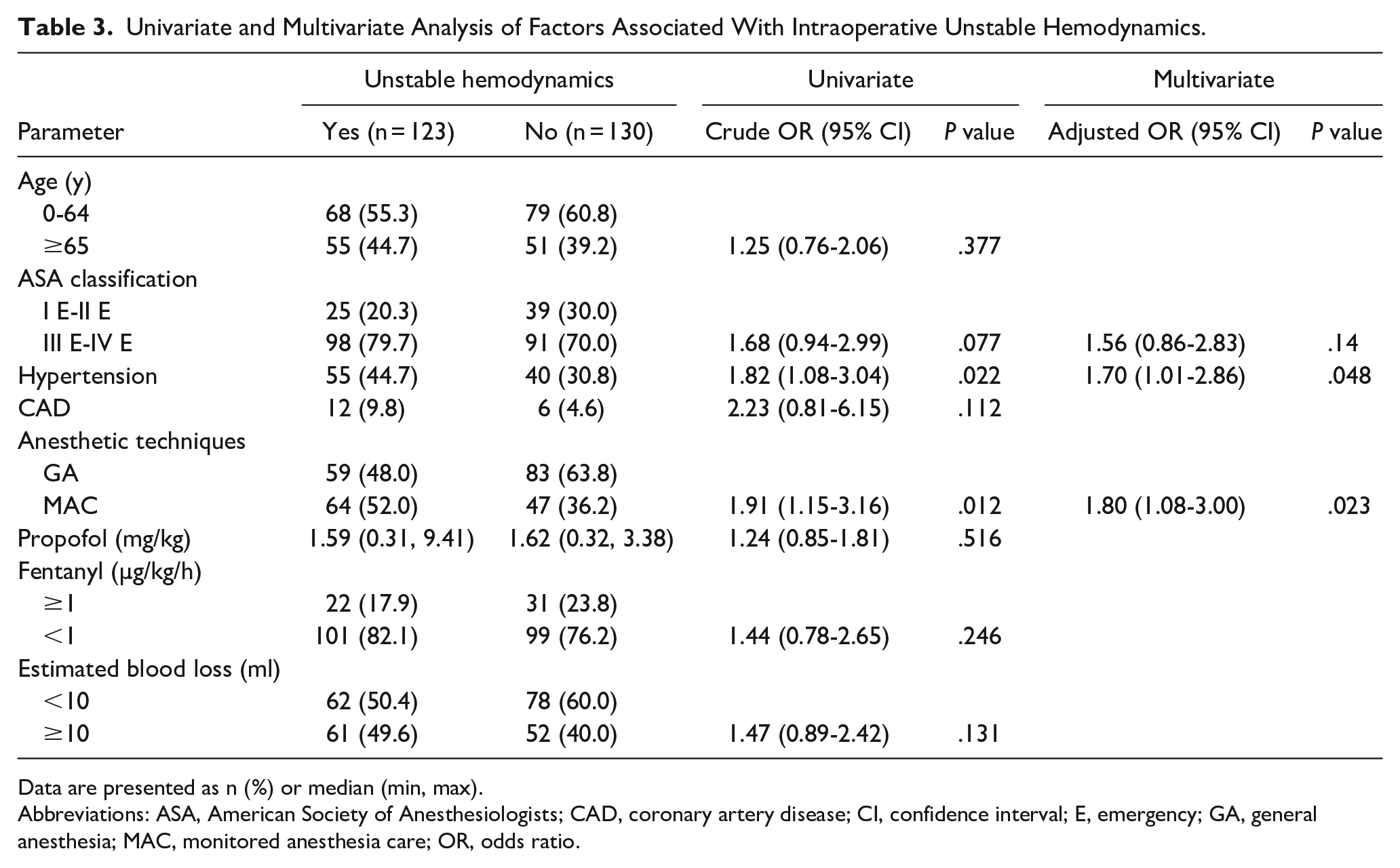
Data are presented as n (%) or median (min, max).
Abbreviations: ASA, American Society of Anesthesiologists; CAD, coronary artery disease; CI, confidence interval; E, emergency; GA, general anesthesia; MAC, monitored anesthesia care; OR, odds ratio.
Discussion
This study revealed that the incidence of intraoperative and early postoperative complications (within 7 days) after emergent tracheostomy was 51.8% and 46.7%, respectively. Cardiovascular instability, particularly hypertension and hypotension that require treatment, represented the majority of the complications observed (52.9%). The prognostic assessment revealed that monitoring anesthesia care, as an anesthetic technique, and the presence of underlying hypertension were identified as significant factors influencing unstable intraoperative hemodynamics.
Tracheostomy can be scheduled as elective or emergency surgery. Elective tracheostomy performed mainly in critically ill patients or with a prolonged ventilatory dependence, which is associated with fewer perioperative complications. The emergency tracheostomy is usually faced with UAO.
In a previous study, the overall surgical complication related to tracheostomy was 27.6% 15 compared to 51.8% in our study, which included surgical and anesthetic-related complications. Ruohoalho et al demonstrated 22% complications in which accidental decannulation (3.9%) and local bleeding (3.1%) play an important role in surgical complications, and for medical complications, pneumonia (4.7%) was the most common complication without mention of unstable hemodynamics. 16 Compared to our study, hypotension (30.4%) and hypertension (22.5%) were the main complications found and combined into unstable hemodynamics (52.9%). In patients who have hypertension as a comorbid disease, intraoperative unstable hemodynamics was significantly related to lower performance status and hypertension itself, which affected the response of the renin-angiotensin-aldosterone system and increased activation of the sympathetic nervous system, making it prone to have unstable perioperative hemodynamics. 17 This study also found that monitoring anesthesia care as an anesthetic technique and intraoperative low-dose fentanyl (lower than 1 µg/kg/hour) was significantly related to unstable hemodynamics. Pan et al compared the use of fentanyl and remifentanil with propofol. The result shows that the fentanyl and propofol group showed more fluctuation in hemodynamics than the remifentanil and propofol group. 17 However, they did not specify the type of surgery that may affect hemodynamics. According to practice, if the patient had severe comorbid diseases or life-threatening conditions, it was likely that a tracheostomy would be performed under MAC. Patients may suffer from pain and discomfort during the tracheostomy and may face unstable hemodynamics intraoperatively.
Subcutaneous emphysema (22.9%) was the most common postoperative complication, followed by minor bleeding (14.2%) despite only 11.5% use of antiplatelets and anticoagulations.
Some studies have indicated that awake tracheostomy procedures yield a higher incidence of subcutaneous emphysema compared to those conducted under general anesthesia. 13 This discrepancy may be attributed to the complexity in awake tracheostomies, driven by the increased acuity of patients’ needs and the procedural challenges. However, our study contradicts this trend, revealing a higher occurrence of subcutaneous emphysema in cases conducted under general anesthesia compared to those performed under local anesthesia with MAC. This discrepancy might be attributed to the surgical team’s experience, as evidenced by the observed phenomenon of tight tissue closure around the tracheostomy tube. In addition, minor bleeding in our study is likely associated with the varying experience levels among surgeons, given that over half of the participating surgeons were residents with comparatively less experience compared to the otolaryngology (ENT) staff. However, bleeding has been reported to be among the most common complications in many previous studies, as has infection and decannulation. 18
Preoperative, intraoperative, and postoperative protocols or checklists must be implemented to ensure safe practice and help reduce unwanted outcomes. According to our practice, we also develop a guideline for UAO as shown in Figure 1 to provide a manipulation system and to facilitate the healthcare provider who must face these types of patients. Before initiating anesthetic care for the patient with UAO, ensure that an airway risk assessment is performed. Conduct an airway examination to further identify physical characteristics that may indicate the potential of difficult airways along with the search for life-threatening conditions such as congestive heart failure and uncontrolled systemic disease. Choose whether to perform a tracheostomy under MAC or general anesthesia. If ventilation can be controlled, the patient was put to sleep and intubated. If the intubation fails, then an alternative approach to intubation is required in not more than 3 attempts. We must consider invasive airway access or awaken patients if repeated failure.
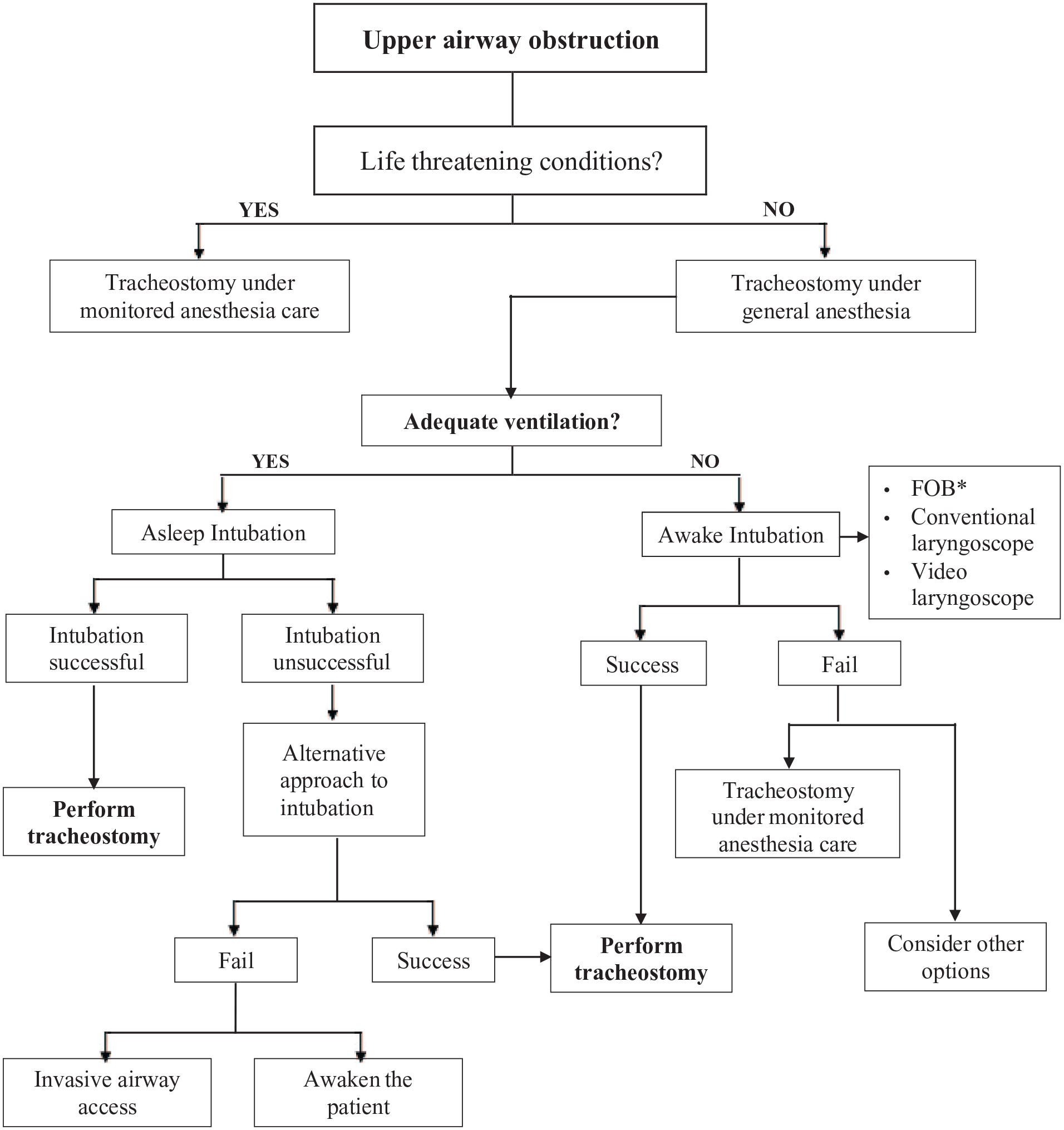
Upper airway obstruction guideline.
In general, mortality associated with tracheostomy complications was relatively low. In exemption of a very high-risk patient such as a patient with respiratory failure scheduled for tracheostomy who has severe comorbidities, for example, pulmonary hypertension, low ejection fraction, mortality could be as high as 39%. 19 Compared to our study, life-threatening complications such as cardiac arrest occurred only in 0.8% of the patients with no intraoperative mortality. More than 95% complete immediate recovery and 7 days after surgery, the rest need ventilatory support and admission to an unplanned ICU. Few patients die or need end-of-life care at home 7 days after surgery due to progressive underlying conditions.
Limitations
There are limitations in our study due to its retrospective design, and the data reviewed in the medical records, in some cases, were limited. This study included only emergency tracheostomy in the surgical ENT unit in the operating room. Emergency tracheostomy is also performed in other departments and outside the operating room. This study was conducted in a single university hospital. More studies should be multicenter and cover all emergency tracheostomy performed in the hospital.
Conclusions
The overall rate of intraoperative complications for emergency tracheostomy was 51.8%. Patients with hypertensive disorder and the use of the monitor anesthesia care technique were a significant risk factor for unstable hemodynamics intraoperatively. It is important for the surgeon and anesthesiologist to identify these factors and intensively discuss the choice of anesthesia and surgical technique to prepare, prevent, or manage unwanted outcomes.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241238620 – Supplemental material for Emergency Tracheostomy: Complications, Anesthetic Techniques, and Outcomes
Supplemental material, sj-docx-1-ear-10.1177_01455613241238620 for Emergency Tracheostomy: Complications, Anesthetic Techniques, and Outcomes by Ekanong Sutthipongkiat, Saowapark Chumpathong, Lapatrada Boonmak, Sriwimon Panyamee, Khanittha Vorasanon and Peerachatra Mangmeesri in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
The authors gratefully acknowledge Rinrada Preedachitkun for her assistance with statistical analysis and Associate Professor Arunotai Siriussawakul for the professional editing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.