
Abstract
Rheumatoid nodules are extraarticular complications in rheumatoid arthritis (RA). This report details how a 63-year-old female patient with a history of lung and kidney cancer presented to the otolaryngology clinic with left submandibular region neck pain and a lesion that looked like a thyroglossal duct cyst on imaging. The patient also had accompanying joint pain. After the patient underwent a full workup including positron emission tomography and computed tomography scans, she underwent surgery to remove the suspected thyroglossal duct cyst via a Sistrunk procedure. Pathology indicated that it was a rheumatoid nodule. The patient was never diagnosed with RA until after removal of the nodule was done. The patient ended up being evaluated by rheumatology and has subsequently been treated for RA. This rare case highlights the importance of interdepartmental communication and assessment of all patient symptoms on examination.
Introduction
Rheumatoid nodules are one of the most common extraarticular manifestations (EAMs) noted in rheumatoid arthritis (RA), with approximately 7% of patients demonstrating nodules at the time of diagnosis and as many as 35% of individuals having reported experiencing rheumatoid nodules. 1 Rheumatoid nodules are superficial lesions in the deep subcutaneous tissues and are most commonly found on the olecranon, extensor surfaces of the forearm, hands, and other areas of repetitive trauma. However, they can also be found in deeper tissues such as tendon- and ligament-like structures, the periosteum, bursae, and vocal cords.1,2 In this report, we describe a female who presented with joint pains and neck pain with a lesion that looked like a thyroglossal duct cyst, which ended up being a rheumatoid nodule.
Case Report
A 63-year-old female with a past medical history of renal cell carcinoma and adenocarcinoma of the lung was referred to the otolaryngology clinic by oncology for left submandibular region neck pain for 3 months that worsened following endotracheal intubation for a lung biopsy. Her positron emission tomography (PET) scan showed a nonspecific asymmetric soft tissue within the left posterior nasopharynx with hypermetabolic activity of standardized uptake value (SUV) 4.7 and asymmetric mild hypermetabolic activity posterior to the left hyoid bone, SUV 2.3.
Physical examination revealed tenderness to the anterior aspect of the left submandibular gland without any discrete palpable neck masses or purulence from submandibular ducts. Nasal endoscopy showed a cyst in the nasopharynx that appeared as a Thornwald’s cyst.
The nasopharyngeal cyst was endoscopically biopsied and pathology revealed squamous and respiratory epithelium-lined lymphoid tissue with focal inflammation without malignancy. Flexible laryngoscopy was unremarkable. Subsequently, a computed tomography (CT) scan of the neck with contrast was ordered and the patient was seen in follow-up with otolaryngology to discuss findings.
CT scan showed a 2 cm × 1 cm × 1 cm mass within the left paraglottic fat abutting and inferior to the hyoid bone, corresponding to the hypermetabolic activity seen on the PET CT. On sagittal imaging, there appeared to be a soft tissue lesion anterior to the thyrohyoid membrane, extending through the thyrohyoid membrane and traveling behind the left hyoid bone as shown in the photographs. Given this, we felt this likely represented a thyroglossal duct tract or cyst given its anatomic relationship with the hyoid bone (Figures 1 and 2).
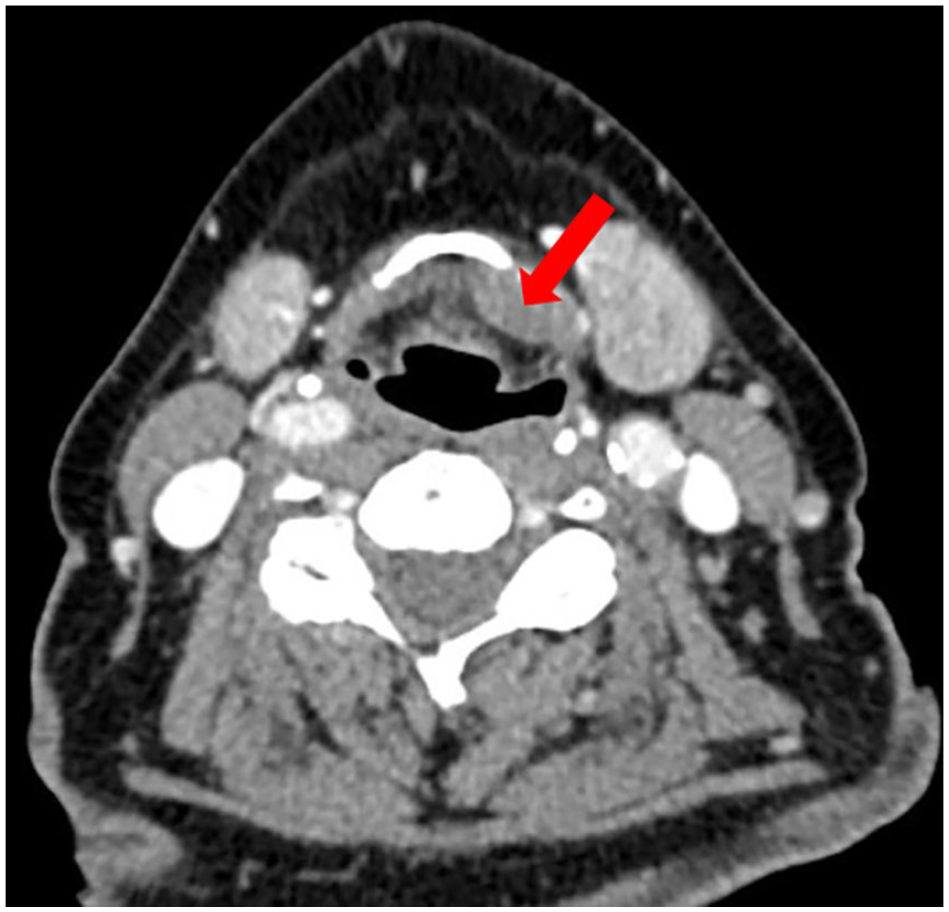
Axial CT of the neck showing a 2 cm × 1 cm soft tissue mass (shown with arrow) attached to the left side of the hyoid bone. CT, computed tomography.
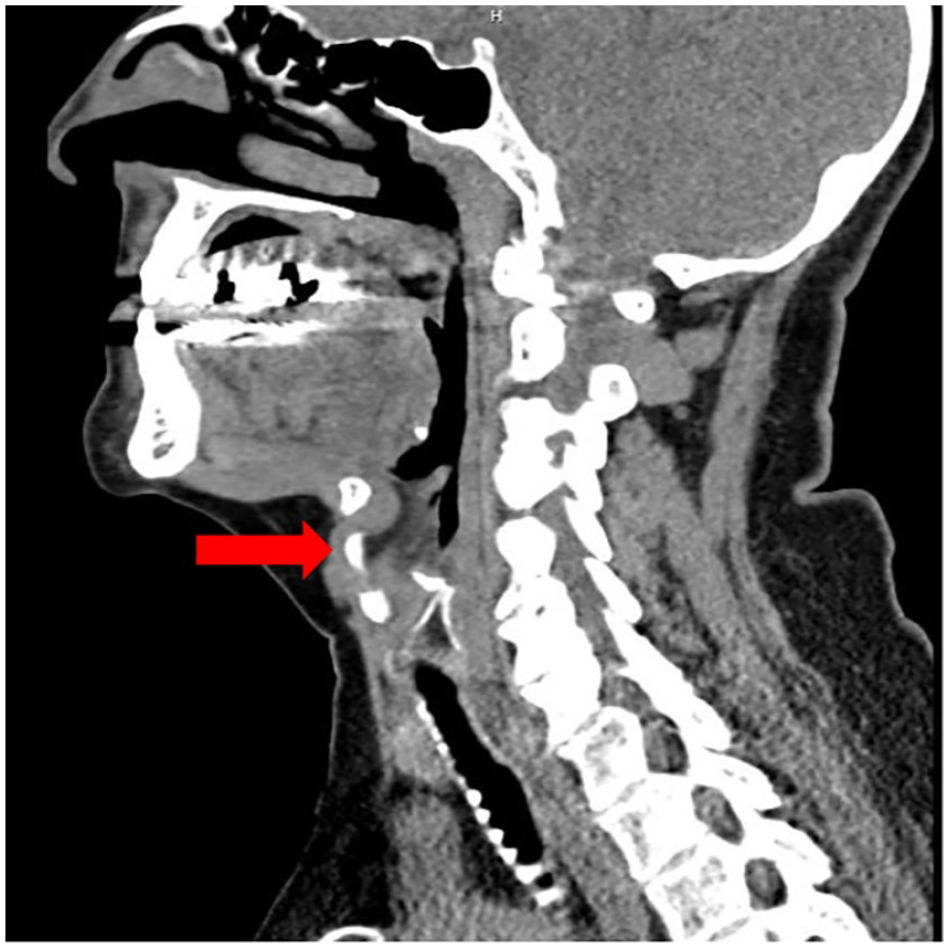
Sagittal CT of the neck showing a soft tissue mass (shown with arrow) anterior to the thyrohyoid membrane and tracking through thyrohyoid membrane into the prelaryngeal area. CT, computed tomography.
Options were discussed with the patient. We discussed with our interventional radiology colleagues to see if they could perform an ultrasound-guided biopsy of this mass but they did not feel comfortable with this. Given this, the patient elected to proceed with surgery to resect the mass and to rule out malignancy particularly given her history. She underwent mass excision via a Sistrunk approach which is typically performed for thyroglossal duct cysts. Intraoperatively, a firm 2.5 cm × 1.5 cm cystic-appearing mass started anterior to the thyrohyoid membrane with a tract under the hyoid bone primarily to the left side. The lesion was firmly adherent to the posterior aspect of the hyoid bone and the central portion of the hyoid bone was resected with the lesion in a standard Sistrunk manner. There was no visible tract extending superiorly or posteriorly to the hyoid bone toward the tongue base. On postoperative day 1, she had some worsening swallowing so she was given a dose of intravenous dexamethasone. Interestingly, the patient immediately felt improvement in her joint pains and swallowing after the dexamethasone injection. Pathological analysis of the neck mass revealed a necrobiotic palisaded granulomatous inflammation representing a rheumatoid nodule (Figure 3).
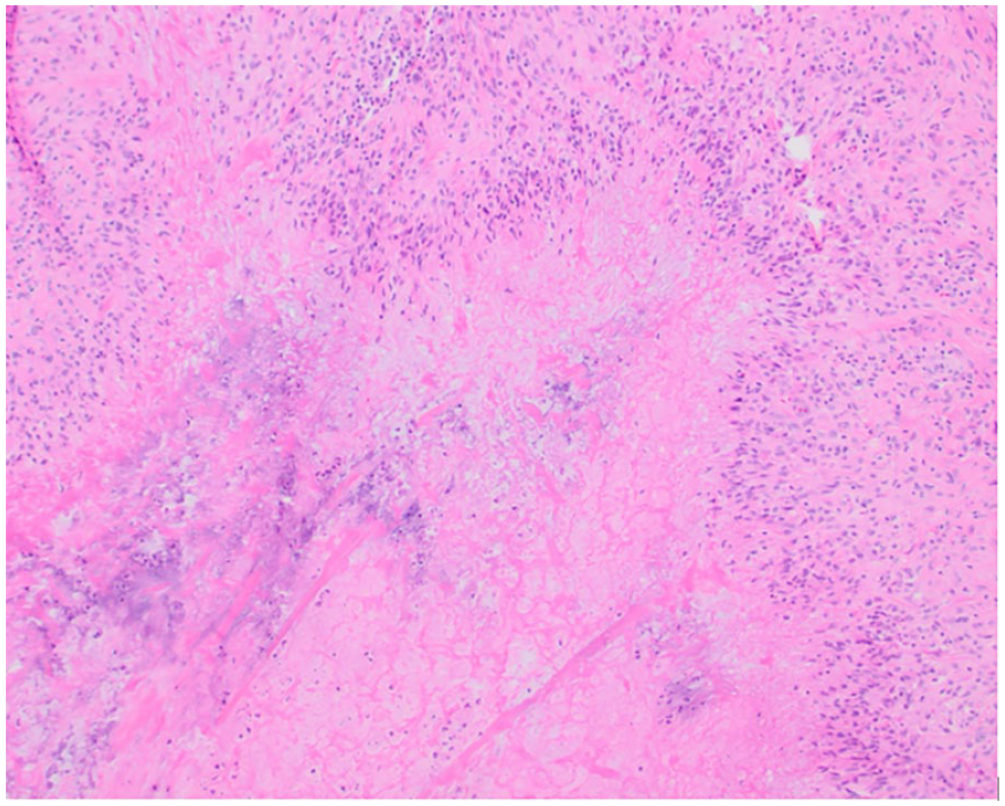
H&E stain under 100× magnification revealing granulomatous inflammation surrounding central necrosis with palisading histiocytes adjacent to necrotic debris with scattered neutrophils overall consistent with necrobiotic palisaded granulomatous inflammation. H&E, hematoxylin and eosin.
The patient was then evaluated by rheumatology for pain in her hands, wrists, elbows, and knees, which had been present for the previous 10 months. The patient expressed that since taking dexamethasone she had had significant relief in pain from her joints for several days after surgery. She had multiple laboratory studies completed which were consistent with RA and she was subsequently treated for this condition. Complete blood count with automated differential, comprehensive metabolic panel, connective tissue disease cascade, C-reactive protein, and cyclic citrullinated peptide antibody laboratory studies were ordered to rule out connective tissue disease. She recovered well from surgery and did not have any complications. Of interesting note, the left submandibular gland pain she had before surgery completely resolved after surgery.
Discussion
The most important finding of this case report is the identification of a rheumatoid nodule rather than a thyroglossal duct cyst. This holds significant clinical implications, as understanding and recognizing such deviations in presentation are crucial when determining medical intervention. This unexpected finding emphasizes the importance of maintaining a broad differential and obtaining an appropriate review of systems with each patient.
Rheumatoid nodules are most commonly found on the olecranon, extensor surfaces of the forearm, hands, and other areas of repetitive trauma.1,2 However, RA can also extend its impact to the larynx, ears, and nose, leading to otorhinolaryngological symptoms. 3 Rheumatoid nodules can also mimic head and neck malignancies, especially in patients who have an oncological history. 4 Rheumatoid nodules can also present in the subepiglottic region, mimicking a thyroglossal duct cyst as initially thought in our patient.
As the thyroid anlage descends from the foramen cecum at the base of the tongue to the pretracheal inferior midline neck, the thyroglossal duct develops. 5 Persistence of the duct may give rise to a clinical cyst, although the duct usually involutes. Thyroglossal duct remnant cysts (TGDCs) are clinically one of the most common neck lesions with a bimodal age distribution in the first and fifth decades of life, with approximately 2.2/100,000 in the population at risk per year. 5 Males tend to predominate in the pediatric population whereas females predominate in the adult population. 5 The cyst wall is smooth and demarcated and is usually solitary, unilocular, round, or oval-shaped with a vertical long axis. 6 The recommended procedure for removal of a TGDC is the Sistrunk procedure, ensuring removal of the full length of the duct remnants, including the cylinder of tissue at the base of the tongue and the midportion of the hyoid bone. 5
RA is a chronic inflammatory joint disease that can cause musculoskeletal deficits, decline in physical function, quality of life, and cumulative comorbid risk.3,7 RA is pathologically heterogeneous with the presence of autoantibodies against citrullinated peptides and autoantibodies against immunoglobulin G [IgG; rheumatoid factor (RF)].3,7 The presence of autoantibodies is associated with more severe symptoms, joint damage, and increased mortality. 7 Rheumatoid nodules are characterized histopathologically by a pattern of necrobiotic granuloma with a central red area due to fibrin. 8 The pathogenesis of rheumatoid nodules is unclear, with the most widely accepted explanation being they are mediated by immune complexes. 8 Fibrin deposits are secondary to complement activation due to aggregation of IgM-RF on the endothelial surface of the cell after vascular injury, causing an immune complex formation. 8
Rheumatoid nodules within the thyrohyoid membrane are rare, and the presentation of these nodules, especially to the hyoid bone, is not often seen, which makes this case presentation unique. 9 This stresses the importance of keeping a robust differential diagnosis when evaluating neck masses. Better overall control of RA disease activity is associated with a decreased incidence and impact of EAMs, such as rheumatoid nodules. 10 Treatment of rheumatoid nodules is an area of research that needs more data. Some studies have shown that injection of glucocorticoids can reduce the size of rheumatoid nodules but is seldom used today due to the risk of infection, recurrence of nodules, and persistent drainage. 1 Furthermore, there have been documented cases of patients developing laryngeal rheumatoid nodules during methotrexate therapy, a widely employed treatment for RA.11,12 An interruption to methotrexate medication leads to a decrease in the size of the rheumatoid nodules.13-15 Current data is unclear and there is little support to suggest that treating rheumatoid nodules helps with symptoms. 1
In the future, individuals similar to our patient may potentially avoid surgical interventions by maintaining a comprehensive list of potential diagnoses and recognizing the distinctive presentation of rheumatoid nodules in this manner.
Footnotes
Acknowledgements
The authors are particularly grateful for the patient allowing us to present this interesting case.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Patient consent for publication was obtained.