
Abstract

Significant Statement
Fine structures of the temporal bone require accurate imaging technology to differentiate between abnormal conditions and normal microanatomy. A newly released photon-counting detector computed tomography (CT) provides better visualization of the fine structures of the temporal bone compared to the current generation energy-integrating detector CT. In this report, we show images of the temporal bone acquired with the photon-counting detector CT that highlight the benefits of this emerging technology.
Imaging Clinic
Accurate imaging of intricate structures of the temporal bone are required to distinguish abnormal conditions from normal microanatomy. To meet this need, otologists have relied on multidetector computed tomography (MDCT), which utilizes an energy-integrating detector (EID) to acquire high-resolution images. However, despite some improvements in this technology, certain limitations of EID-MDCT still hinder progress in reducing the radiation dose and achieving higher spatial resolution. To overcome these limitations, photon-counting detector CT (PCD-CT) has been developed. In Japan, the first commercial PCD-CT (NAEOTOM Alpha; Siemens Healthcare) received approval in January 2022. Our hospital has recently started to use PCD-CT in regular clinical practice. In this report, we present a case that demonstrates the exceptional quality of imaging achieved with the PCD-CT platform.
The patient was a 49-year-old woman with a middle ear cholesteatoma of the right ear who underwent tympanoplasty. An initial CT image prior to surgery was obtained with a conventional EID-MDCT scanner (SOMATOM Force; Siemens Healthcare), while a follow-up CT image after surgery was acquired with the PCD-CT scanner. The acquisition parameters were as follows: for EID-MDCT: 120 kV, 64 mm × 0.6 mm (slice thickness reconstructed to 0.6 mm), pitch 0.85, quality reference mAs (quality ref. mAs) 320, and 1 second rotation time; for PCD-CT: 120 kV, 120 mm × 0.2 mm, pitch 0.85, IQ level 150, and 0.5 second rotation time. The image matrix was 512 × 512 for EID-MDCT and 1024 × 1024 for PCD-CT, and image data were reconstructed using a high-resolution kernel. CT images of the temporal bone of the unaffected side were compared between the two CT scanners. Fine details of small structures in the middle ear and inner ear were well visualized, with clear boundaries (Figures 1–3).
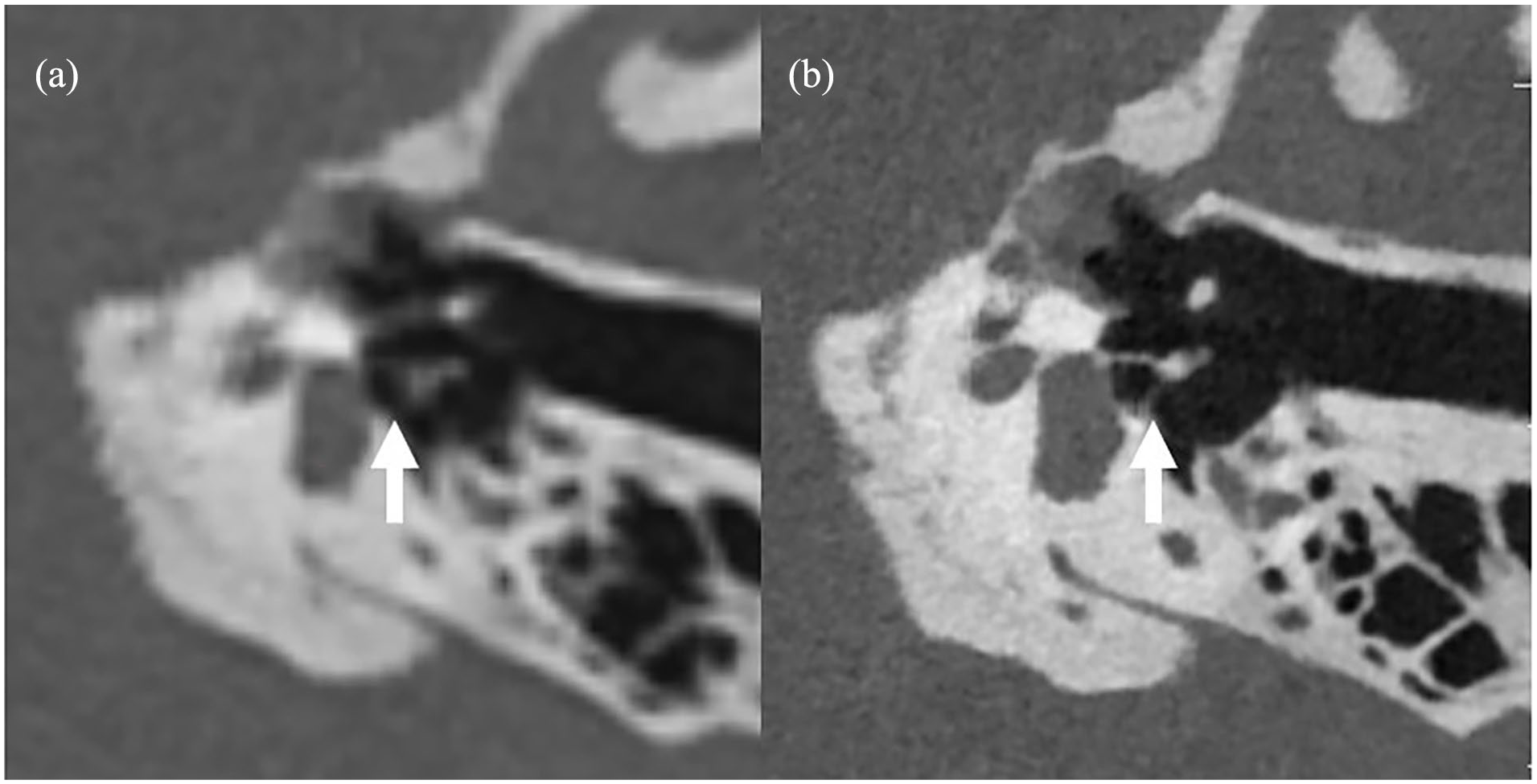
(a) EID-MDCT and (b) PCD-CT images reformatted in the axial stapes plane, showing the crus of the stapes (arrows). Note the anterior and posterior crus of the stapes are better visualized on the PCD-CT image. EID, energy-integrating detector; MDCT, multidetector computed tomography; PCD-CT, photon-counting detector computed tomography.
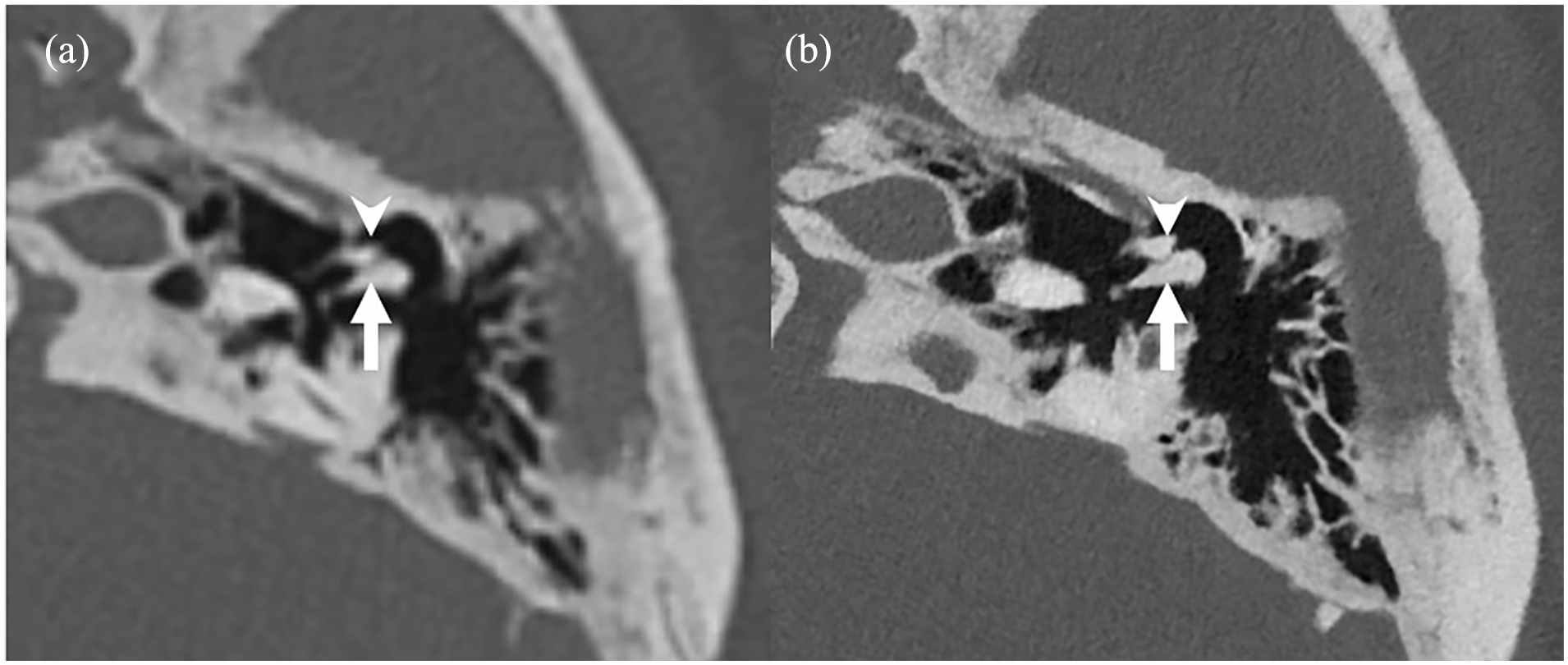
(a) EID-MDCT and (b) PCD-CT images reformatted in a plane parallel to the long process of the incus, showing the incus and malleus. The incus (arrows) and malleus (arrowheads) are better visualized with clear boundaries on the PCD-CT image. EID, energy-integrating detector; MDCT, multidetector computed tomography; PCD-CT, photon-counting detector computed tomography.
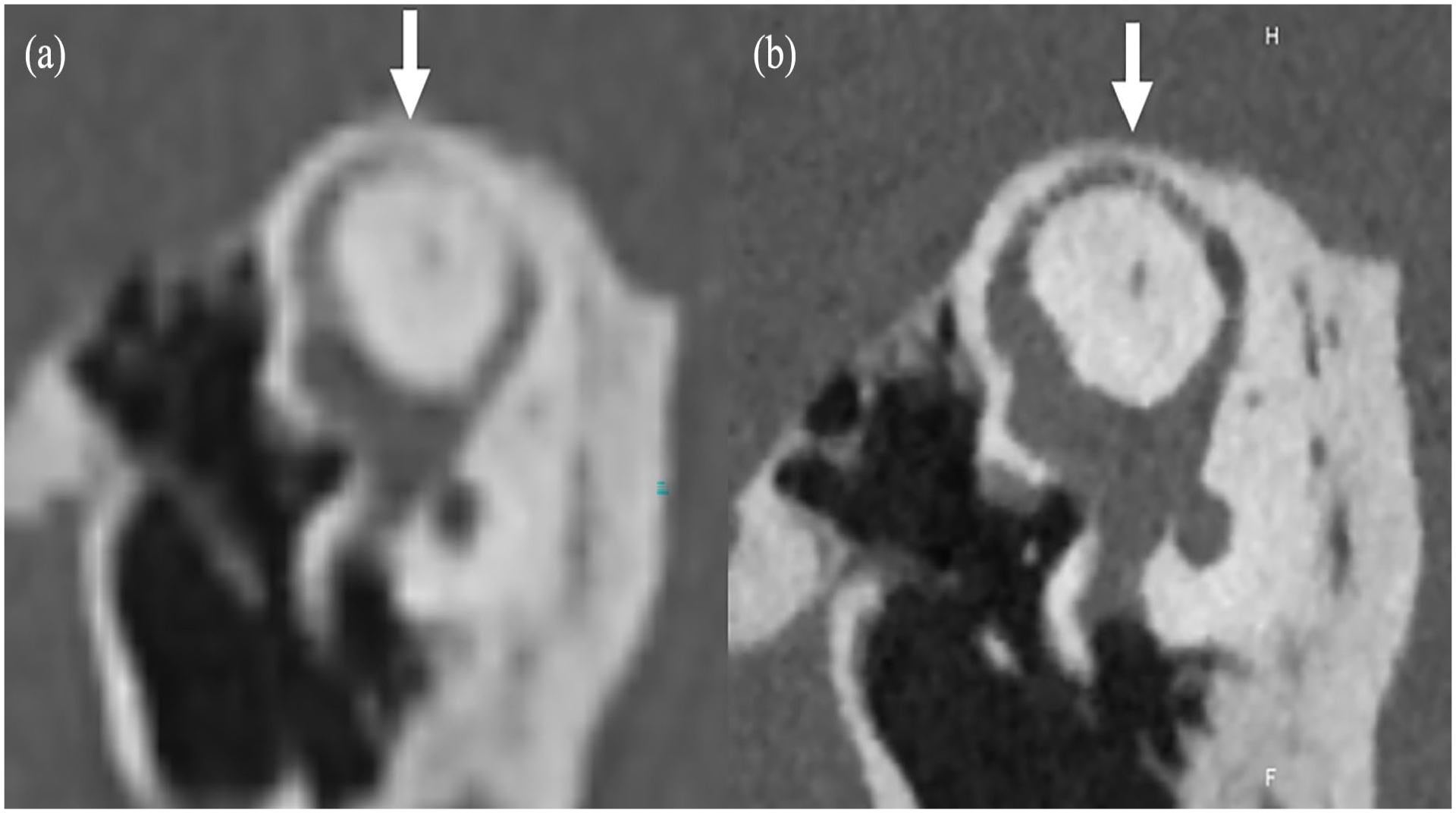
(a) EID-MDCT and (b) PCD-CT images reformatted according to the Pöschl plane, showing the superior semicircular canal. The bony layer covering the superior semicircular canal (arrows) is better visualized on the PCD-CT image. EID, energy-integrating detector; MDCT, multidetector computed tomography; PCD-CT, photon-counting detector computed tomography.
A technical description of the mechanism of CT may help otologists understand how CT produces high-resolution images. In EID-MDCT, the absorbed energy of photons is converted to light by a scintillator, which is then converted to an electrical signal by a photodiode. The output of an EID is influenced by the total energy of the incident photons. Photons with higher energy generate more light and therefore have a greater impact on the output electrical signal of the EID. As described above, EID-MDCT does not directly convert the incident photons to a signal, whereas PCD-CT directly measures each photon and its energy. PCD-CT utilizes a semiconductor material to convert each incoming photon directly into an electric signal, which is promptly detected and processed for accurate determination of the number of photons received. When a photon strikes the detector, it generates a charge cloud, and the size of this cloud corresponds to the energy of the incoming photon. By measuring these energy levels, advanced reconstruction technology can produce higher quality images and spectral information.
The reconstructed thickness of PCD-CT is 0.2 mm, which is 3 times thinner than that of EID-MDCT, 1 and PCD-CT provides a higher imaging quality of fine structures in the temporal bone compared to that acquired with EID-MDCT. 2 For instance, detecting subtle anomalies of the ossicular chain or minute dislocations of the ossicles that can cause conductive hearing loss is likely to be more accurate using PCD-CT. 3 Moreover, it should be possible to distinguish true dehiscence of the superior semicircular canal from false-positive cases. 4 These characteristics of PCD-CT suggest that it will be beneficial for both otologists and radiologists in diagnosis of conditions of the temporal bone region.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.