
Abstract
Choanal polyps belong to a special type of nasal polyps, which are quite uncommon if originating from the nasal septum, especially those with osseous metaplasia. In this article, we report the case of a 63-year-old male patient with persistent nasal obstruction on the right side. An irregular light yellow lobulated mass with smooth surface could be visualized in the nasal cavity through nasal endoscopy, arising from the right nasal septum and extending to the nasopharynx. Computed tomography scan showed a large soft tissue shadow of the nasal meatus, with ossified structure in the center. Histopathological biopsy revealed nasopharyngeal mucositis. The patient underwent functional endoscopic sinus surgery and the polypoidal mass sent for histopathological examination proved to be choanal polyps.
Introduction
Choanal polyps belong to a special type of nasal polyps, mostly arising from the lateral wall of the nasal cavity, especially in the maxillary sinus which can extend to the oropharynx when the polyps are large. It has also been less reported that polyps can originate from the sphenoid sinus, ethmoid sinus, middle turbinate, inferior turbinate, and nasal septum. 1 Choanal polyps arising from the nasal septum are quite uncommon and those with osseous metaplasia are even rarer.
Choanal polyps have many different characteristics, but those with osseous metaplasia are quite rare. At present, the pathogenesis is still unclear, and some studies have reported that its pathology is closely related to inflammation. 2 The predominant symptom is persistent or intermittent unilateral or bilateral nasal obstruction. Other symptoms include snoring, runny nose, and anosmia. At present, surgical resection is the preferred treatment. 3 Here, we report a case of choanal polyp with osseous metaplasia arising from the nasal septum.
Case Report
The patient, a 61-year-old male, was admitted to our hospital due to right nasal obstruction for more than 3 years. The patient presented with persistent right nasal obstruction 3 years ago with no obvious inducement, accompanied by runny nose, snoring, nasal discharge stained with blood, without open-mouth breathing, dizziness, tinnitus, loss of olfaction, loss of hearing, nasal itching, or sneezing. The patient underwent computed tomography (CT) examination at a local hospital and then underwent endoscopic-guided nasopharyngeal biopsy, which was proved to be mucositis in the nasopharynx, heterogeneous cell nests in the stroma, which was likely to be tumor. Further immunohistochemistry showed that there was no evidence of tumor and reexamination was necessary.
The patient was referred to our hospital for further examination to confirm the diagnosis. The histopathological examination findings of our hospital showed that there were many glands hyperplasia, lymphocyte infiltration, tissue extrusion in the nasopharyngeal mucosa, the morphology of which was consistent with chronic inflammation of the mucosa. The patient underwent nasal endoscopy in our hospital, which showed slightly larger bilateral inferior turbinates, pale and edematous middle turbinate, mucilage-like secretions in the middle meatus, and masses in the posterior edge of the posterior choanae and the nasopharynx that were hard to touch (Figure 1). CT examination showed bilateral ethmoid sinusitis, left maxillary sinusitis, irregular soft tissue filling in the right nasal cavity, and nasopharynx (Figure 2). At last, the patient was admitted to our department, diagnosed with “nasopharyngeal lesions (which was needed to be proved further).” Physical examination showed clear bilateral tympanic membrane mark, without congestion, tympanic membrane invagination, and fluid; slightly larger bilateral inferior turbinate; pale and edematous middle turbinate; as well as hard masses with light color in the middle meatus and nasopharynx, but without deflection in the nasal septum.
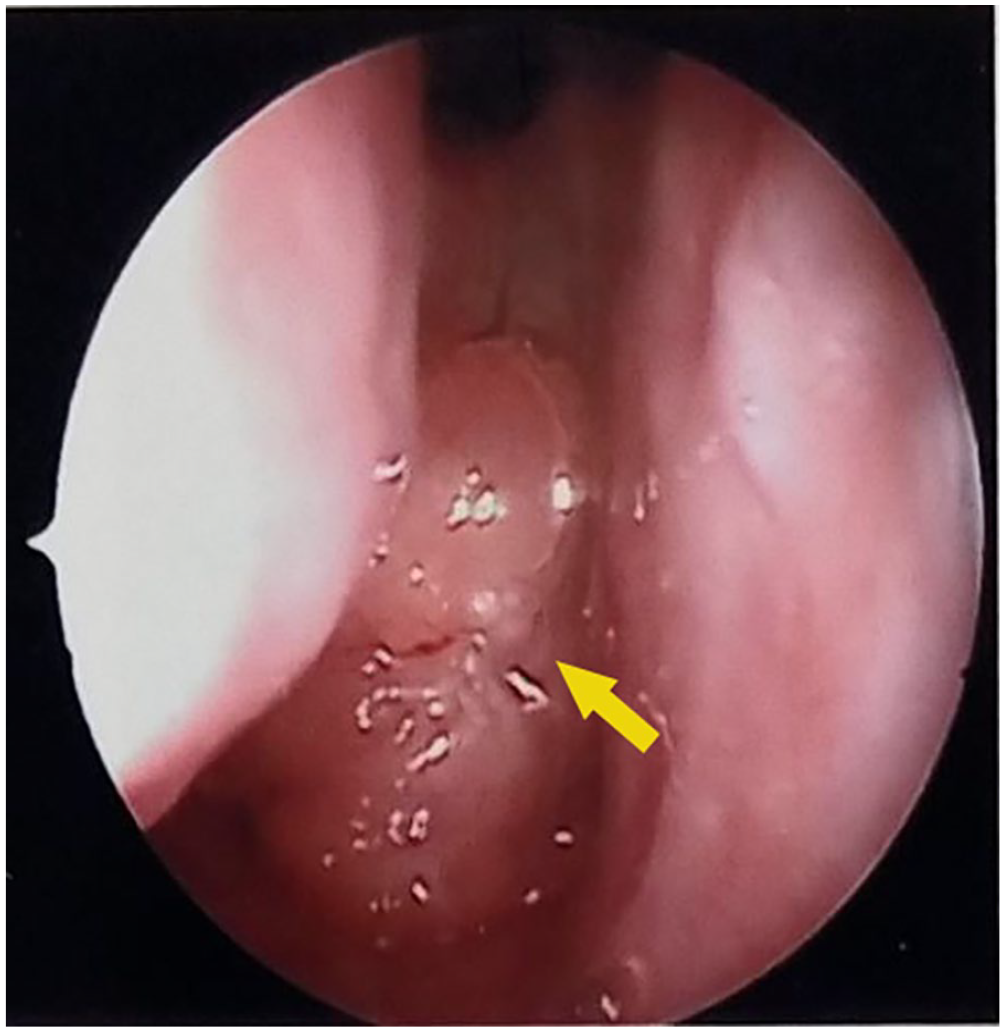
Nasal endoscopy showed that there was tumor growth at the posterior edge of the posterior nostril, nasopharynx, and the contact was hard (yellow arrow).
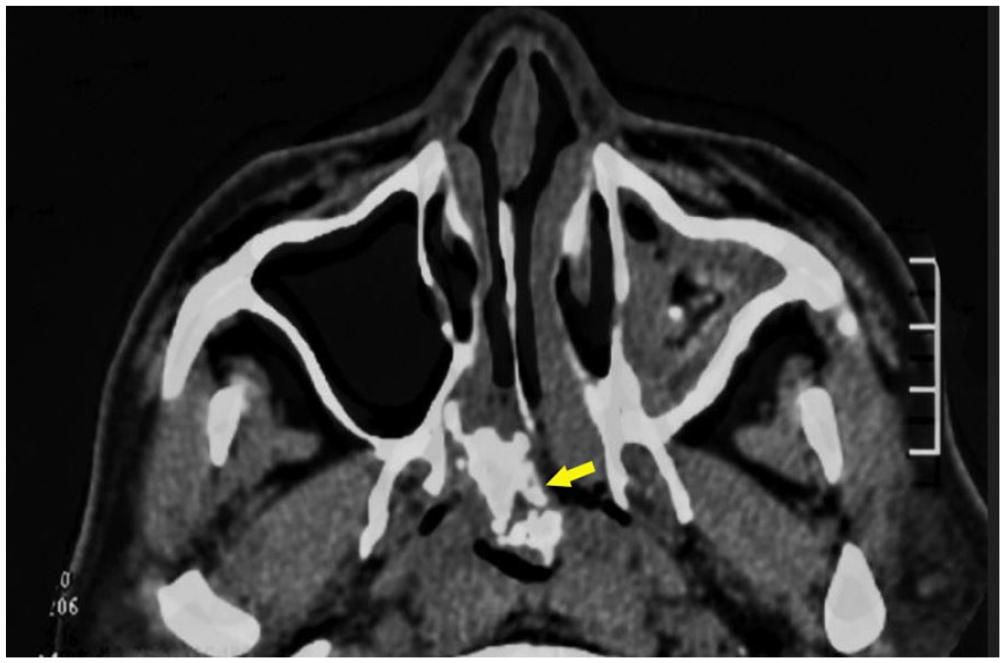
CT axial scan of soft tissue window showed that osseous trabeculae (yellow arrows) in polyps entered nasopharynx from nasal cavity through choana. CT, computed tomography.
After conducting relevant preoperative examinations and assessment, the patient underwent functional endoscopic sinus surgery (FESS) under general anesthesia and the left maxillary sinus, ethmoid sinus, and right sphenoid sinus were exposed to remove the masses. It was found that masses in the nasopharynx were arising from the right nasal septum, and the posterior choanae was completely blocked. The part of the mass was cut out by forceps and sent for rapid frozen pathological examination during the operation, which showed that no malignant tissue was found. Then, the remaining mass was completely removed block by block because it was large. Through exploration, it was found that the mass was arising from the end of the right nasal septum, with bone destruction near the ostium of sphenoid sinus. Therefore, part of the sphenoid ethmoidal plate was resected and the ostium of sphenoid sinus was enlarged. Part of the mucosa of posterior nasal septum was removed. The left maxillary sinus and ethmoid sinus were exposed to clear lesions. After the operation, the patient was treated with routine standard management and discharged according to doctor’s advice. The postoperative pathological report showed that mature trabecular bone tissue and new bone tissue are covered by respiratory polypoid mucous membrane without eosinophils infiltration (Figure 3).
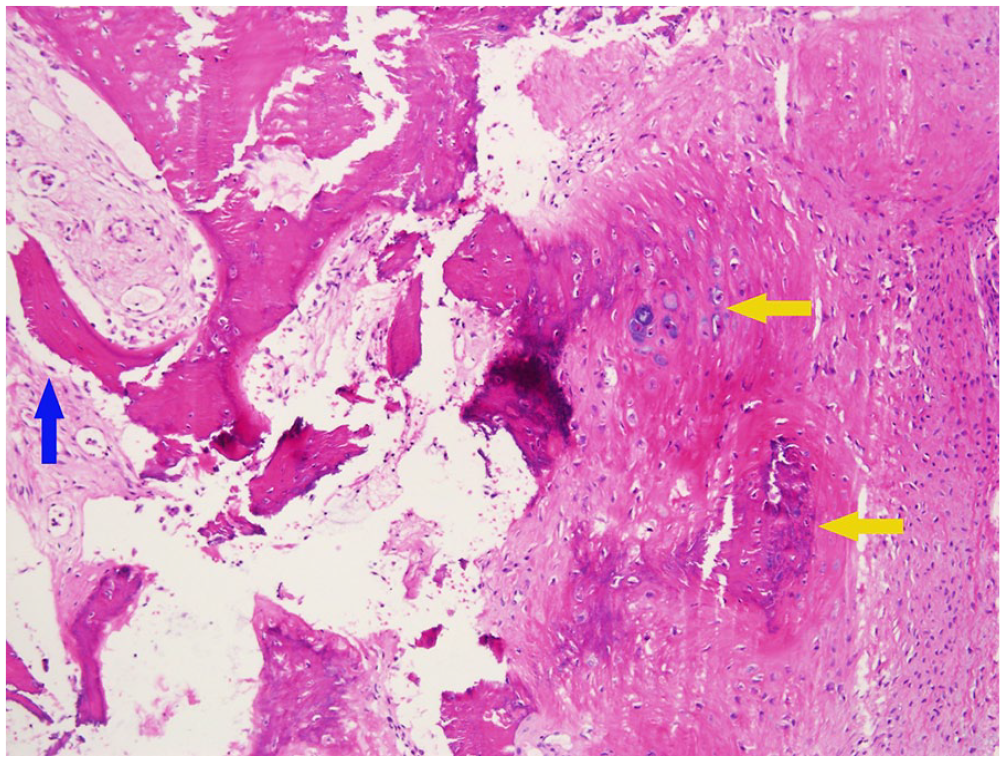
Histopathology (hematoxylin and eosin, original magnification, ×10) revealed that mature trabecular bone tissue (blue arrow) and new bone tissue (yellow arrow) were covered by respiratory polypoid mucous membrane without eosinophils infiltration.
Discussion
Nasal polyp is a kind of common disease in otorhinolaryngology, but choanal polyps are relatively uncommon in clinic, especially those arising from nasal septum are quite rare. It has been found that choanal polyps with osseous metaplasia can originate from ethmoid sinus, middle meatus, middle turbinate, and inferior turbinate. Rare literature reported that choanal polyps can also originate from nasal septum and lateral wall of the nasopharynx. 4 The predominant symptoms presented are nasal obstruction, snoring, and other discomfort, and there is a certain recurrence rate after surgery. Previous studies reported the choanal polyps arising from nasal septum but did not mention the polyp accompanied with osseous metaplasia.5-7 The nasal polyp with osseous metaplasia is a quite rare disease. Mucosal polyps with osseous metaplasia in other parts of the body, such as stomach, 8 rectum,9-11 and colon, 12 have also been reported.
At present, the mechanism of osseous metaplasia is not clear. It has been reported that mucosal polyp mesenchymal cells differentiate into osteoblast progenitors and then mature into osteoblasts under the influence of bone morphogenetic proteins (BMPs) and transforming growth factor-β1. 13 It has also been reported that mesenchymal cells in mucosal polyps differentiate into osteoblasts when the secretion of local alkaline phosphatase increases. 14 The effect of BMP may be related to the upregulation of type 1 collagen and osteonectin.15,16
In the CT examination of nasal sinuses, nasal polyps often present with even soft tissue masses with smooth edges and no bone destruction, while nasal polyps with osseous metaplasia manifest with multiple high-density shadows in the center of the polyps. When there is high-density shadow in CT examination, it should be differentiated from nasal calculus, inverted papilloma, osteosarcoma, fibrosis, and other diseases, because they can all have similar results in CT. 17
In the present case, the polyp ossification is obvious, which may be related to the long course of disease and calcium deposition. The CT findings of the sinuses are dumbbell shaped with clear linear trabeculae, which are easily differentiated from nasal calculus, fungal sinusitis, and inverted papilloma. The biopsy reports of the nasopharynx in other hospital showed that mucositis of the nasopharynx and the polyp biopsy failed because it is accompanied with osseous metaplasia with hard texture, and it is hard to get the central part of the mass.
At present, FESS is still the first choice for the treatment of polyps with osseous metaplasia. If the mass is large, it can be removed block by block or through the mouth. The final pathological specimen of this case confirmed that mature bone trabecular tissue was covered by polypoid mucosa of respiratory tract.
Conclusion
Although osseous metaplasia in choanal polyp is quite uncommon in clinic, we also need to be aware of the existence of this kind of disease and be able to differentiate it from other diseases. Large osseous metaplasia in polyps may make it more difficult for the surgery and use longer time to resect the mass, thus increasing the possibility of postoperative complications. Therefore, adequate preoperative preparation is conducive to the smooth completion of the operation, the selection of the optimal surgical plan, and the improvement of the patient’s prognosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Clinical Medical Research Center of Shaanxi Provincial (No. 2021LCZX-15) and Natural Science Basic Research Program of Shaanxi Provincial (No. 2018JQ8074).