
Abstract
Testicular calcification is caused by calcium deposits of the testis in men with controversial and unknown etiology. Calcifications with a size >3 mm are considered as macrocalcifications. Calcifications are the result of high local calcium concentrations in many tissues. Ultrasonography is the gold standard imaging tool for testis investigation. We report a 28-year-old man who presented with left testicular pain and an inguinal hernia from 1 year ago. The ultrasonography demonstrated a hypoechoic calcified region size of 12 × 18 mm. The tumor markers were negative. After radical orchiectomy, the histopathology showed testicular calcification with benign osseous metaplasia. Calcification within a testis is found incidentally using ultrasonography since it may be misdiagnosed as a small benign or malignant mass.
Introduction
Testicular calcification is the deposition of calcium occurring in the intratesticular or extratesticular and may be diagnosed as a benign or malignant mass in men. The actual etiology, formation, and function of calcified mass in the body are unclear. 1 They are usually asymptomatic and may have been distinguished incidentally by a physician during scrotal ultrasound or routine physical examination. 2 Calcifications are categorized into three groups based on size: microlithiasis, macrocalcification (non-microlithiasis), and tumor-associated calcification, so the site, extent, and distribution of calcifications are informative on ultrasound examination. The size of macrocalcification is more than 3 mm and microcalcification is smaller than 3 mm.1,3–5 Calcification cannot be identified by patients during self-examination if it is not large enough.1,6 Differentiation between different calcifications would greatly help urologists and andrologists manage the practice and pay more attention. 7 The prevalence of testicular microlithiasis (TM) was reported to be 2.4%–5.6% in adults without symptoms, 0.6%–9% in adults with symptoms, and the prevalence of macrocalcification was reported to be 1.7%.8–10 The prevalence and genetic predisposition to calcifications are not explored fully in various ethnic populations. In addition, TM is observed in two types; classic: defined by the presence of five or more microliths on at least one ultrasound image, and limited: which is defined by the presence of fewer than five microliths on all images with a range in size from 50 to 400 μm.3,8
Approximately 5%–10% of the testicular masses are identified as benign testicular lesions after surgery. 11 The question is whether the calcified region is associated with cancer risk. Concerning that the testis is a site of a variety of testis cells, the patient with calcification within the testes is at higher risk of carcinoma in the future. 12 Many studies have reported a significant association between testicular calcification and the risk of testicular malignancy; however, some other studies did not report finding such an association and its role in the progression of cancer is still unknown.13,14 Wang et al. 15 reported a relationship between calcification with testicular cancer. De Gouveia Brazao et al. 16 reported that the prevalence of carcinoma in situ in patients with bilateral TM is significantly higher than in patients without TM. Pedersen et al.17,18 reported that TM is a risk factor for cancer as part of chromosomal abnormalities of the testis. TM with other risk factors (infertility, age, and testicular dysgenesis syndrome) are involved in the development of male reproductive cancer.5,19,20
However, ultrasonography (US) is considered the first-line option to assess the presence of calcified region and testicular mass without any side effects by urologists in the last decades, it has limitations for the evaluation of morphology and details of calcifications. 4 A testicular calcified mass may be reported on ultrasound, but the exact finding and differential diagnosis of primary benign or malignant mass are very important.6,21 These differential diagnoses in a patient include spermatic granuloma, large-cell calcifying Sertoli cell tumor, trauma, tuberculosis, filariasis, calcified Leydig cell tumor, and burned-out testicular tumor. 6 Therefore, reliable preoperative factors are important for an appropriate distinction between benign and malignant testicular lesions. Early detection of malignant or benign tumors using molecular biomarkers and US is very important in the clinic.22–24 Here, we described a case of a 28-year-old male with calcification and osseous metaplasia in the testis. Written consent was obtained from the patient.
Case report
The patient was a 28-year-old man who was referred to the hospital with a presenting complaint of testicular pain and a suspicious solid mass in his left testis from 1 year ago. The patient had no history of cryptorchidism, testicular trauma, hydrocele, infection, fever, and family history of testicular tumor. There were no changes to the scrotal skin or solid palpable mass over this period. The patient had normal urination, scrotal skin, and regular size of both testes.
During his physical examination, a left inguinal hernia was detected. The urologist ordered an ultrasound to further characterize his testicular pathology. US of the scrotum was performed and revealed a grade I varicocele in the pampiniform plexus vein of the left testis, a hypoechoic mass (12 × 18 mm) with calcified septa without evidence of differentiation into other cells or peripheral malignancy in the left testis. The size of the right testis was reported at 52 × 24 mm and 60 × 24 mm for the left testis. Also, the size and shape of the epididymis and echo of the testes’ parenchyma were normal (Figure 1).
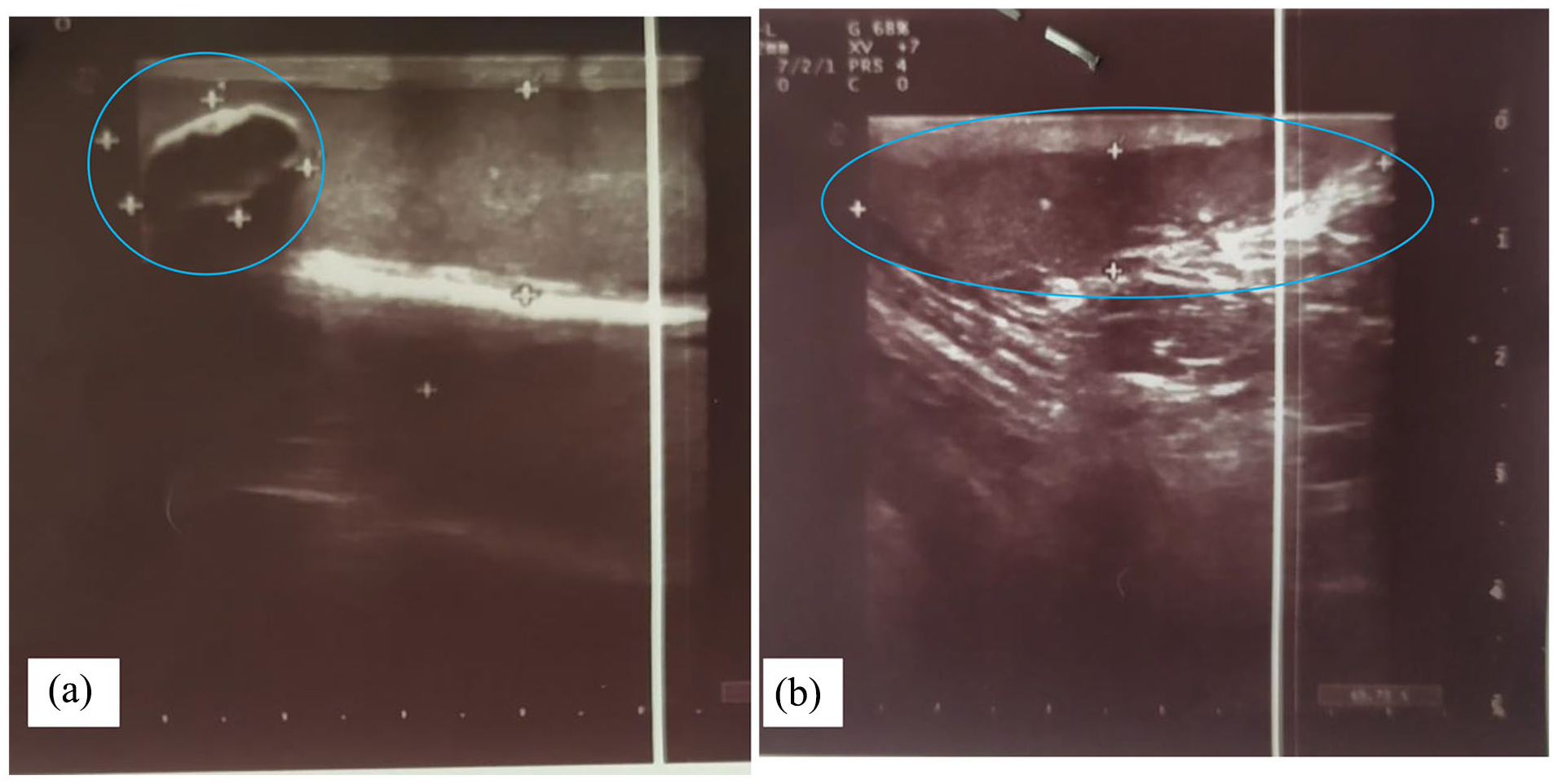
Ultrasound images showed the area of hypoechoic calcified mass (a) and inguinal hernia (b) in the left testis.
Blood analyses of alpha-feto-protein (2.06 ng/ml, reference range up to 7) as tumor markers and beta subunit of human chorionic gonadotropin (0.78 mIU/ml, reference range less than 3.0) and lactate dehydrogenase (380 U/L, reference range <480) levels of the patient were within normal limits. Moreover, the results of the biochemical tests, urine analysis, and complete blood count were normal. After a thorough discussion with other colleagues, clinical examination, US findings, and the possibility of malignancy, the patient was admitted to the surgery unit. The operation was performed under sterile conditions and general anesthesia. Radical orchiectomy and herniorrhaphy were performed, the hernial sac was repaired, and the operation was ended by closing the fascia and layers of skin repaired with silk1 and nylon 2/0 properly.
After orchiectomy, the labeled specimen was sent to the pathology department. Macroscopic examination of the orchidectomy revealed a testis of 7.5 × 5 × 4 cm and a spermatic cord of 9 cm in length and 2 cm in diameter. There is a creamy colored well-circumscribed firm mass, measuring 1.5 × 1 × 1 cm in the superior testis located 4 cm from the mediastinum. Cut sections of the lesion showed a cystic lesion containing white-colored amorphous materials (Figure 2). Microscopic evaluation of testicular mass showed an encapsulated intratesticular lesion with calcification, ossification, some macrophages, eosinophilic amorphous material, and a few foreign body-type giant cells. There was no evidence of necrosis, hematoma, or teratoma. There are focal areas of seminiferous tubule atrophy and mild chronic inflammatory cell infiltration at the periphery of lesions (Figure 3). The rest of the testicular tissue showed normal architecture and spermatogenesis. The spermatic cord and epididymis are unremarkable. In the end, it has been diagnosed as a benign mass with calcification and osseous metaplasia in the left testis. Also, the patient was followed up for 10 months and the physical examination, abdominal ultrasound findings, and hormonal profile of the patient were assessed to be within normal limits. Written informed consent was obtained from the patient for publication of the case report. This case study was approved by the Committee for Ethical Consent of Urmia University of Medical Sciences under the number IR.UMSU.REC.1401.373.

Gross appearance of the left testicle demonstrating a testicular mass (cystic lesion) composed of bone and calcified tissue.

Microscopic appearance of the left testicle composed of osseous metaplasia and seminiferous tubules: hematoxylin–eosin (H & E) stain and original magnification 20×.
Discussion
Calcifications are the result of high local calcium concentrations in many tissues. 25 Testicular calcification and microlithiasis are discovered during the investigation of testicular signs and symptoms. 26 Intratesticular calcifications are located in the parenchyma of the testis; some are not large enough to detect. 2 Hiramatsu reported that there was no significant correlation between the number of calcifications and sperm motility, while there was a negative correlation between the number of calcifications and sperm concentration. The European Academy of Andrology reported that sperm concentration and vitality correlated negatively with the number of calcifications.4,27,28 Testis surgery to preserve fertility is recommended. The frequency of calcifications is related to environmental factors and genetic background.
Spermatic granulomas, phleboliths, SLC34A2 gene mutation, and vascular calcification have been identified as risk factors for intratesticular calcification. 8 Moreover, individuals with a history of inflammatory disease of the epididymis are at a greater risk of extratesticular calcification.6,29 Extratesticular calcifications are more frequent than intratesticular calcifications. 6 Furthermore, some genetic disorders, genetic factors, less physical activity, some diseases, the lungs, and the central nervous system are involved in the development of calcification and tumors.9,10 Previous studies mentioned that intra-TM is associated with confirmed testicular cancer based on ultrasound evidence. 17 Fattahi et al. 30 reported a large-cell calcifying Sertoli cell tumor. They mentioned that these tumors are mostly benign and have a good prognosis after surgery.
The current study described a testicular mass with calcification and osseous metaplasia in a young patient. Nevertheless, until now only a few studies have reported calcification with osseous metaplasia. 31 Diagnosis of a calcified mass was made based on ultrasound findings, including a hypoechoic mass in the testicular parenchyma, while the tumor markers were normal. The main reason for calcifications is not reported fully in various ethnic populations. There was no evidence of dermoid cysts, teratoma, burnt-out malignant germ cell tumors, mucine, and scar tissue in the testicular parenchyma. Due to the different sizes of the calcification and the difficulty of distinguishing it from malignancy, radical orchidectomy is often carried out. 32 Preoperative diagnosis is not sufficient to detect malignancy. 33 Benign tumors often are diagnosed as germ cell tumors in patients who are candidates for orchiectomy. However, sparing surgery of the testis based on intraoperative frozen section examination is highly recommended to preserve testicular parenchyma. Furthermore, previous studies reported that US is the first tool for calcification, microlithiasis, and metaplasia diagnosis. 21 Several societies and colleges updated and published more accurate guidelines and recommendations, reference ranges on the appropriate use of US and color-Doppler ultrasound in the evaluation of testicular volume (three maximum diameters), testicular homogeneity/inhomogeneity (grade 1–3), testicular echogenicity (three-point Likert scale), calcifications and microlithiasis (different size and number), testicular vascularization (qualitative and quantitative assessment), and testicular masses.3,4 Miller et al. 29 mentioned that the use of US was very important in malignancy detection. Based on the ultrasound findings, a diagnosis of an intratesticular calcified mass can be made, but details of calcification and metaplasia cannot be identified.
Conclusion
Some appearance of intratesticular-calcified mass could be reported with benign or malignant types. Due to the difficulty of assessing and the short period of follow-up or prognosis, few cases of calcified mass can be recognized in different populations. If a mass is suspected, several biopsies of surrounding testicular parenchyma for molecular genetics or pathology and serum tumor biomarkers for cancer screening will be useful in the surgical approach to correctly discriminate benign from malignant lesions. Molecular pathology and serum biomarkers such as mRNA, microRNA, and small molecules with a longer period of follow-up can be a feasible diagnostic option and clinical information relevant to patients. We proposed an network interdisciplinary between specialists with radiologists, oncologists, pathologists, urologists, and molecular pathologists or genetics which can contribute to the reliable diagnosis and reduction of medical errors in the clinic.
Footnotes
Acknowledgements
We thank the staff of the surgery, Urmia, Imam Khomeini Hospital for specimen processing.
Authors’ contributions
M.P. Participated in the collection of clinical data, evaluation of patient specimens, and interpretation of results. M.N. and A.G. Participated in the evaluation of patient specimens and original draft preparation. F.M. Prepared the full manuscript, writing, and editing of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This case study approved by the Committee for Ethical Consent of Urmia University of medical sciences under the number IR.UMSU.REC.1401.373.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.