
Abstract
Lingual abscesses, characterized by infectious collections of pus within the tongue parenchyma, are rare and poorly understood clinical entities. Despite their potential for severe complications, literature on lingual abscesses remains limited, consisting mainly of sporadic case reports. This comprehensive case study examines the challenges and successful management of a severe anterolateral tongue abscess in a young adult, contributing to the emerging body of knowledge on this condition. A young adult male presented with a progressively worsening painful, swollen tongue and dyspnea over 2 days. Urgent intervention was necessary to prevent potential airway compromise despite maintaining normal oxygen saturation. The patient’s medical history showed no prior oral infections, illnesses, or relevant medical conditions. Detailed clinical assessment, utilization of imaging modalities such as contrast-enhanced computed tomography scan and ultrasonography, and collaboration with a maxillofacial surgeon guided accurate diagnosis and successful treatment. This case study provides valuable insights into the diagnosis and management of anterolateral lingual abscess in a young adult. It underscores the importance of heightened clinical awareness, precise diagnostic techniques, and multidisciplinary collaboration for optimal patient outcomes. The report contributes to the limited literature and emphasizes the need for further research to establish evidence-based guidelines for lingual abscess management.
Background
Lingual abscesses, also known as acute suppurative glossitis, tongue abscess, and acute parenchymatous glossitis, are rare and present as painful infectious collections of pus within the tongue parenchyma. Because of their rarity, current knowledge regarding incidence, etiology, clinical manifestations, and treatment modalities has not been well established. 1 Very scarce information pertaining lingual abscesses has been reported in literature, which mostly consists of case reports at infrequent time intervals, with approximately 50 published over the course of 30 years. 2 Tongue abscesses are infrequently mentioned in medical textbooks, 3 and many head and neck surgeons will never encounter this type of condition. 3 Trauma, foreign objects, dental infection, or tonsillitis have all been suggested as etiological factors. 1 In addition, factors such as poor oral hygiene, heavy smoking, immunodeficiency, chemotherapy treatment, and diabetes may increase the likelihood of developing an abscess. 4 The majority of information was documented during the pre-antibiotic epoch, where findings indicated a mortality rate of 3%. 1 Furthermore, death caused by the underlying disease was usually asphyxia due to upper airway obstruction. In the contemporary therapeutic era, prompt identification, advanced investigations, and swift intervention are expected to mitigate the incidence of morbidity and mortality. Nevertheless, at present, no available data examine the clinical consequences related to morbidity and mortality among individuals with lingual abscess. 1 Lingual abscesses, such as the one described in this case report, require drainage to sequester growth and potential complications. Even minor surgical procedures to the tongue can affect functional outcomes, such as speech and swallowing, negatively affecting patient quality of life and possibly, life expectancy in itself. 5 Lingual abscesses ought to be treated with great caution, especially in infants and immunocompromised patients. The complications of a severe infection may result in life-threatening conditions presenting as airway compromise or a disseminated infection spreading to other regions of the head and neck.
Posterior third lingual abscesses are less common than anterior abscesses, but more concerning, considering that a posterior lingual abscess may potentially cause acute compromise of the airway, particularly if the patient presents with dyspnea and/or dysphagia. In addition to medical evaluation, an assessment of the patient’s underlying medical conditions must be conducted and properly managed. An evaluation of recent history of trauma is also a crucial component in the diagnosis of tongue abscesses. It should also be noted that imaging of the oral cavity and pharynx is key to the diagnosis and choice of surgical approach. Antimicrobial treatment is the core stone in treatment of tongue abscess and should be used immediately in all patients presenting with tongue abscess and should continue using antibiotics as part of postoperative workout in those patients undergoing surgical drainage of tongue abscess in addition to antibiotics treatment. Surgical debridement plays a crucial role in averting further dissemination of the infective process. 3
The current study presents a patient with a severe anterolateral tongue abscess in Ziv Medical Hospital, in the peripheral upper Galilee region in Israel. In this article, a thorough overlook over previous literature, research, and medical textbooks is discussed and summarized in relation to our patient’s conditions and clinical presentation.
Case Presentation
A male in his late 20s presented with a painful, swollen tongue and dyspnea with progressive deterioration over the course of 2 days despite maintaining normal oxygen saturation. The patient denied trauma, chills, sore throat, dysphagia, or vomiting. He did not report prior oral infections or recent illnesses. He had no prior medical or surgical history, was not on any regular medications, and had no known allergies. He reported only heavy cannabis use and no history of tobacco smoking or other drug use.
On physical examination, the patient was awake and alert, speaking coherently but in a labored manner, and looked fatigued. On admission, his pulse rate was 120 bpm (tachycardic), blood pressure was normal (120/80 mmHg), he was febrile (38.5°C), and oxygen saturation was 98% (normal value 90%-100%).
On oral examination, the patient displayed signs indicative of poor oral hygiene, including the presence of plaque and tartar. In addition, signs of gingivitis were observed. These findings were noted despite the dental examination revealing no significant decay or infections. During the examination, it was noted that the patient did not exhibit a “hot potato voice,” a symptom often associated with oral infections but absent in this case.
Head and neck examination revealed a tender mass in the anterolateral right region of the tongue (Figure 1). The tongue was not erythematous, and no external lesions were visible. All teeth present without evidence of any tooth decay and no dental infections or any dental abnormalities were evident. The oropharynx was otherwise unremarkable with normal-appearing tonsils. Head and neck lymph nodes were not enlarged or tender. The remaining of the physical examination was unremarkable.

Physical examination of the tongue. Lateral part of tongue.
Visual inspection using a fiber optic camera revealed no signs of trauma or bleeding; airway and trachea were clear with no signs of discharge. Optimal visualization of the vocal cord and the epiglottis were evident. To complete our investigation, we did a neck ultrasound to check for masses and lymph node abnormalities, which yielded unremarkable and normal findings. Doppler ultrasound (Figure 2) was conducted to evaluate the mass in the anterolateral right region of the tongue, which revealed a tongue abscess that appeared as a hypoechoic lesion surrounded by a hyperechoic ring. The use of contrast-enhanced computed tomography (CT) scan (Figures 3 and 4) has been demonstrated to significantly enhance the diagnostic accuracy, particularly in the detection of tongue base and deep space infections. 1 The contrast-enhanced oro-buccal CT scan revealed the hypodense collection with surrounded enhanced capsule, presenting as an abscess confined at the anterolateral area of tongue.
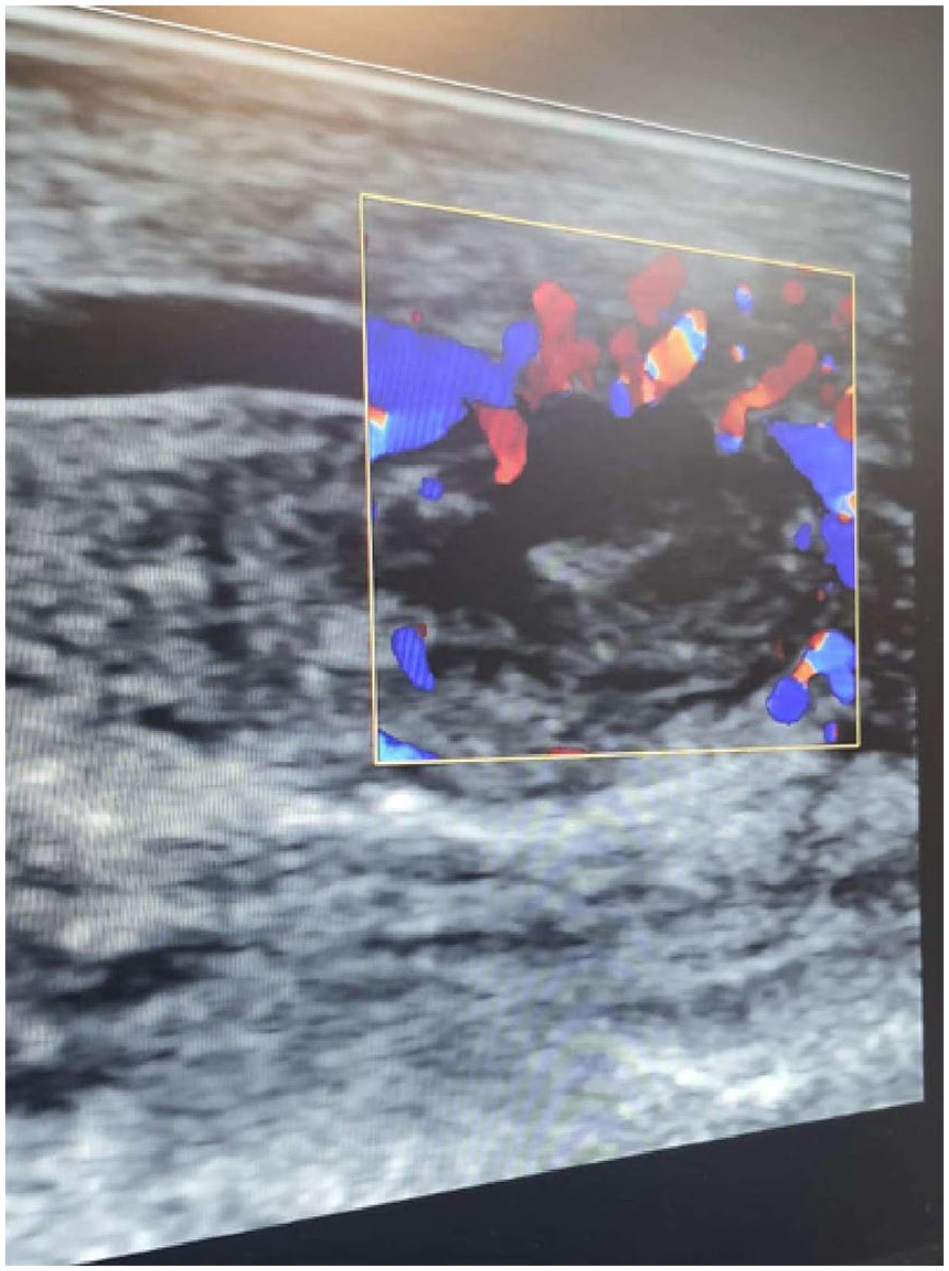
Doppler ultrasound of the tongue.
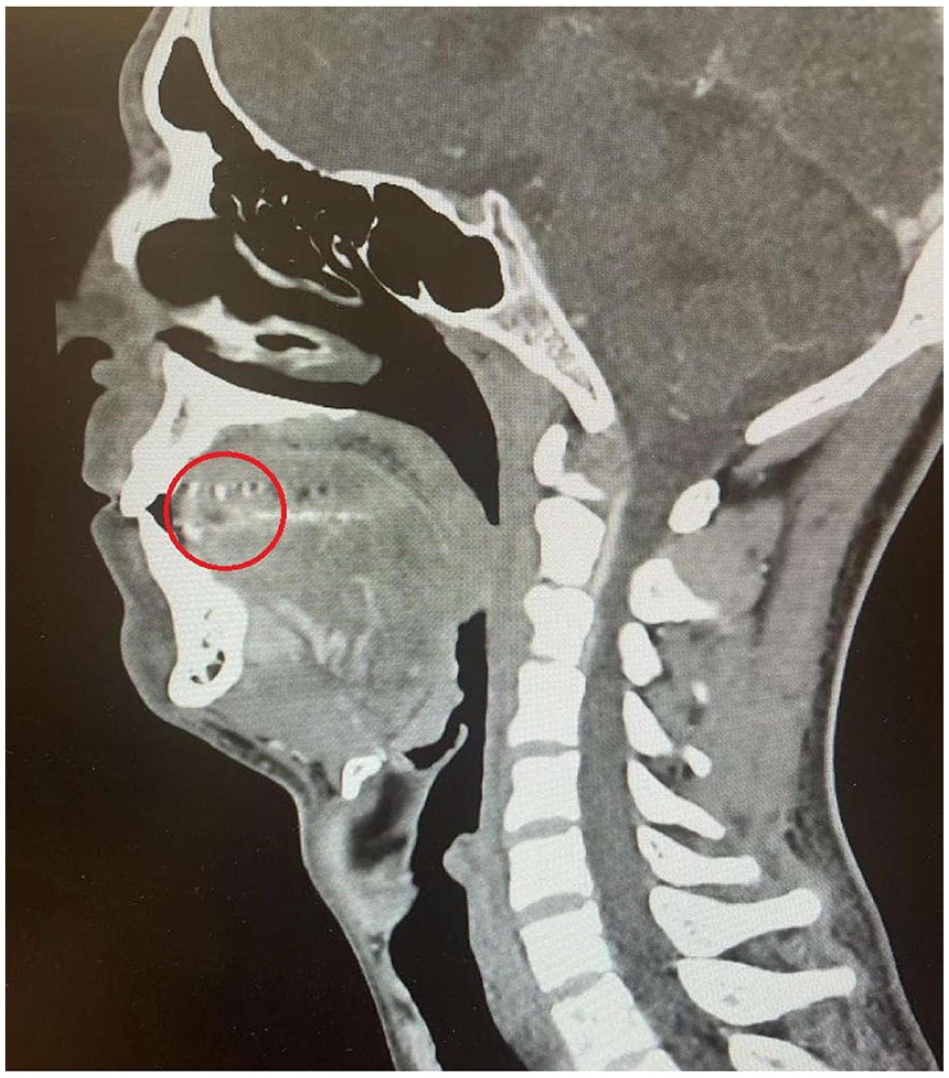
Computed tomography scan with contrast of the head and neck. Sagittal view.
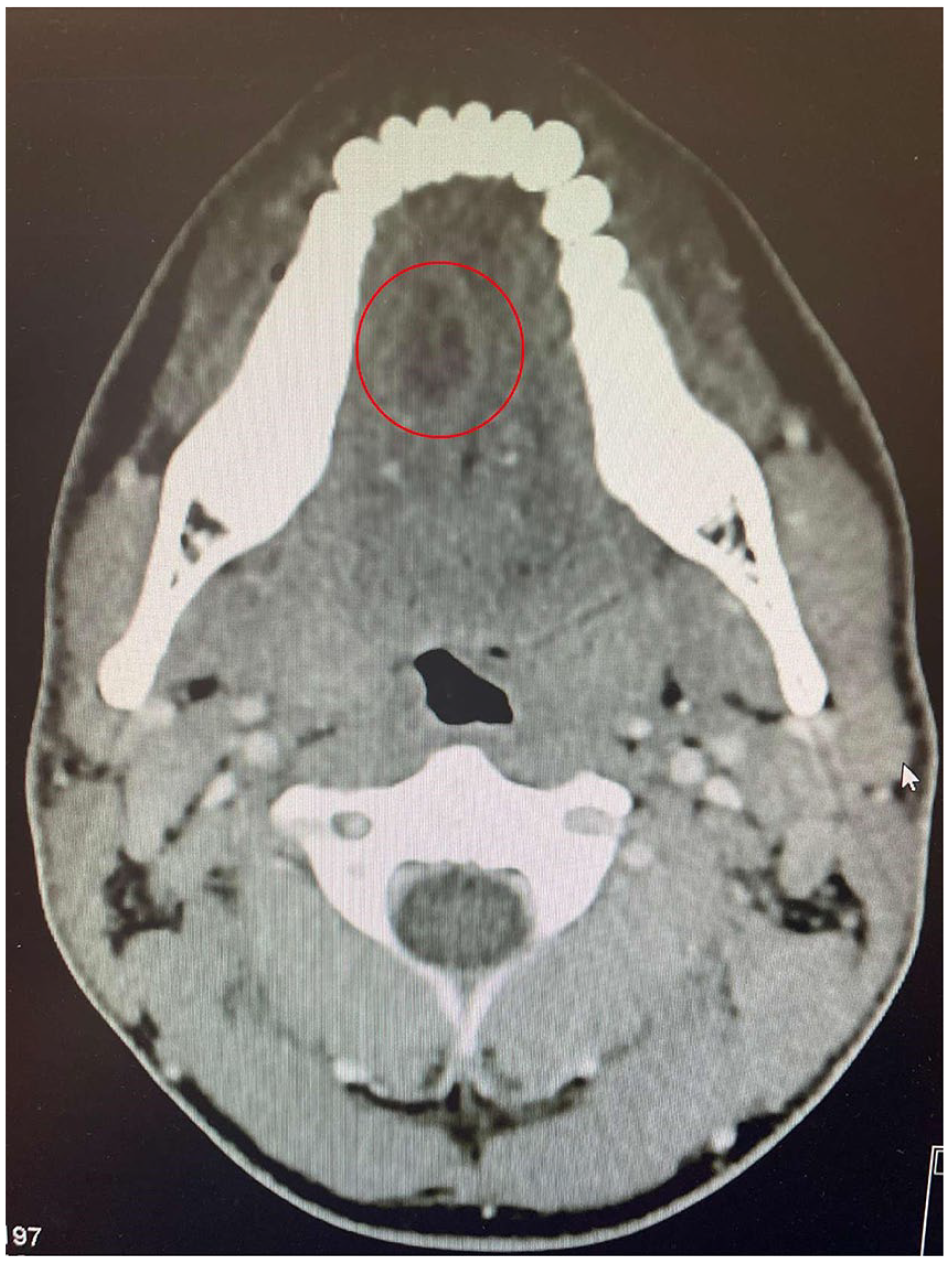
Computed tomography scan with contrast of the head and neck. Axial view.
Airway was secured via oral endotracheal intubation and the abscess was promptly drained via surgical incision following CT scan visualization. Our readiness for potentially more invasive intubation techniques, such as a tracheotomy, was also an integral part of our preparedness, although it was not required in this case.
Ultrasonography-guided needle aspiration aided diagnosis and symptom relief. Surgical intervention under general anesthesia ensured complete abscess removal with saline and 2% hydrogen peroxide wash (Figure 5).

Intraoperative view of the anterolateral part of the tongue with the drained abscess.
Antibiotics intravenous (IV) Zinacef (cefuroxime) 750 mg thrice daily, IV clindamycin 600 mg thrice daily for 1 week, oral Augmentin 875 mg twice daily, and clindamycin 300 mg thrice daily for 10 days. Swelling mitigated with IV dexamethasone 8 mg twice daily for 1 week. Pathological examination confirmed acute and chronic inflammation with abscess formation.
The patient reported significant improvement 1 day postsurgery after abscess drainage. During the hospital stay, IV antibiotics and IV steroids led to marked clinical and laboratory improvement. Bacteriological analysis revealed a polymicrobial infection, specifically including organisms typically found in the oral cavity and oropharynx, such as Streptococcus spp., Staphylococcus spp., and various anaerobic bacteria. 1 This supported the continuation of the appropriate antibiotic regimen.
Three days post surgery, the patient resumed normal eating and was discharged with oral antibiotics, instructed to seek emergency care for symptom exacerbation. One week later, follow-up at ENT department and maxillofacial surgeon consultation ensured symptom alleviation and ruled out recurrence or complications.
Discussion
Our case report highlights the challenges and management of a severe lingual abscess in a young adult. Lingual abscesses, though rare, can present as painful infectious collections of pus within the tongue parenchyma. Due to their rarity, established management guidelines remain scarce, leading to limited literature and case reports. Prompt diagnosis and intervention are crucial to prevent complications, including airway obstruction and systemic infection.
Our patient’s presentation demonstrated a painful, swollen tongue with dyspnea, requiring swift action to secure the airway. This was achieved using oral endotracheal intubation, ensuring airway patency and safety during the management of the lingual abscess. Imaging modalities, including contrast-enhanced CT scan and ultrasonography, aided in accurate diagnosis and surgical planning. Surgical incision and drainage, guided by ultrasonography, along with appropriate antibiotics and steroids, resulted in significant improvement and successful resolution of the abscess.
The most probable cause of the tongue abscess in our patient was attributed to poor oral hygiene and heavy cannabis use. Collaboration with a maxillofacial surgeon was essential to address underlying factors and optimize the treatment plan. However, it should be noted that lingual abscesses can have various etiologies, including trauma, dental infections, immunodeficiency, and diabetes.
Despite the paucity of data on lingual abscesses, this case underscores the importance of early diagnosis, thorough investigation, and multidisciplinary management to achieve favorable outcomes.
In conclusion, our case report contributes to the growing body of literature on lingual abscesses and highlights the need for heightened awareness among healthcare professionals. The cornerstone of treatment includes the protection of the airway, prompt administration of appropriate antibiotics and steroids, surgical excision of the abscess, and subsequent pathological review. Our patient’s successful outcome, with significant improvement and minimal complications, aligns with the proposed optimal treatment strategy. Although the medical literature on this subject remains limited. Future research should focus on larger-scale studies to provide evidence-based guidelines for the management of lingual abscesses, improving patient care and prognosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from the patient for the publication of this case report and accompanying images.