
Abstract
Introduction
Sudden sensorineural hearing loss (SSNHL) is a medical condition where there is rapid and unexplained hearing loss in one or more adjacent frequency bands, with a decrease of over 20 dB within 72 hours of completing a pure-tone audiometry test. 1 Although this condition has experienced a surge in prevalence worldwide in recent years, it can manifest at any age, yet its etiology and pathophysiology remain ambiguous. 2 Sudden hearing loss can coincide with tinnitus, reduced aural acuity, and vertigo, as well as other subjective symptoms, which have a substantial impact on a patient’s work life and daily function. Patients understandably desire prompt and efficient treatment following their visit to the clinic. Although existing guidelines do recognize specific factors that affect the prognosis of sudden deafness, such as the initial visit time and the hearing loss curve’s type, research demonstrates that further factors affect treatment outcomes. Consequently, identifying clinical features and indicators linked to prognosis constitutes a crucial aspect of current research on sudden deafness, seeking to enhance patient outcomes via focused interventions.
Currently, there is a scarcity of studies that comprehensively take into consideration the clinical characteristics and laboratory indicators of patients. This study aims to fill this gap by examining the clinical data and laboratory indicators of 414 patients who were hospitalized at our institution between January 2020 and December 2022. Our aim is to identify factors that could affect the prognosis of these patients and establish a theoretical foundation for forthcoming treatments.
Materials and Methods
Study Subjects
The examined information focuses on 414 patients who were admitted to the First People’s Hospital of Zhenjiang city from January 2019 to December 2022 due to sudden deafness.
Inclusion criteria: patients must meet the diagnostic criteria outlined in the guidelines for the diagnosis and treatment of sudden deafness (referred to as the guidelines 3 ; this includes undergoing pure-tone audiometry, acoustic impedance, otoacoustic emission, and magnetic resonance imaging (MRI) or computed tomography (CT) examination of the internal auditory canal both before and after treatment. Other criteria include experiencing unilateral onset of the disease, making their first visit to the clinic, receiving no targeted treatment before the current visit, and undergoing a hematology examination on the day following admission to the hospital.
Exclusion criteria: middle ear or retrocochlear lesions, hearing loss caused by trauma or medication, and malignant tumors of other major organs are potential causes of impaired hearing. In addition, an MRI or CT scan of the internal auditory canal may suggest vestibular aqueduct, acoustic neuroma, or other conditions affecting hearing.
Materials Collection
General Information
Clinical data were collected from all participants in the study, including information such as gender, time from onset to treatment, age, affected ear, accompanying symptoms such as vertigo, tinnitus, or ear stuffiness, and the presence of comorbidities such as hypertension or diabetes mellitus. Furthermore, we documented the frequency and seriousness of hearing loss.
Laboratory Indicators
On the morning of the patient’s second day of hospitalization, a blood sample was taken to test for several markers, such as C-reactive protein, neutrophils, lymphocytes, triglycerides, total cholesterol, high-density lipoprotein (HDL), and low-density lipoprotein (LDL).
SSNHL Curve Typing and Assessment of the Degree of Hearing Loss
The study performed pure-tone audiometry tests on all participants before and after treatment. The hearing profiles of every participant were sorted in line with the regulations. 3 Four types of hearing loss were identified: a low-frequency descending type, which refers to hearing loss of at least 20 dB at 250 to 500 Hz; a high-frequency descending type, which refers to hearing loss above 2000 Hz and at least 20 dB at 4000 to 8000 Hz; a flat descending type, which refers to a mean hearing threshold of 80 dB or less at 250 to 8000 Hz; and a deaf type, which refers to a mean hearing threshold of at least 81 dB at 250 to 8000 Hz. Following the pure-tone audiometry assessments, the extent of hearing impairment was determined by categorizing it under the following classifications: mild (25-40 dB HL), moderate (40-60 dB HL), moderate severe (60-80 dB HL), and very severe (>80 dB HL).
Methods of Treatment
Based on the recommendations in the guidelines, 1 the following treatments were administered:
Systemic steroids involved administering intravenous methylprednisolone 40 mg daily over 3 days. Subsequently, steroids dosage was gradually tapered over 2 days while monitoring hearing response. In cases where there was inadequate response, intradrum injection of dexamethasone 5 mg was prescribed on alternate days while hearing was evaluated on the other days.
Nutritional neurotransmission, which entailed administering a 400 mg injection of methylcobalamin once daily.
Vasodilation was managed with a daily intravenous injection of 400 mg triclabendazole in combination with 250 mL of 0.9% sodium chloride. In addition, adjuvant therapy was administered to patients meeting requirements for hyperbaric oxygen therapy. For those suffering from both hypertension and diabetes mellitus, treatment was provided to stabilize blood pressure and blood sugar levels during therapy. Patients who underwent intravenous steroid shock and demonstrated noteworthy hearing improvement after 3 days or self-reported hearing improvement during the recheck of pure-tone audiometry could decrease their hormone dosage to 20 mg and sustain medication usage. If the hearing recovery was unsatisfactory, intradural injections were considered, and hearing tests were conducted every other day. As per the guidelines, patients with various types of sudden deafness received necessary treatment based on the basic treatment. Systemic steroids were administered to patients with low-frequency hearing decline when treatment was ineffective or inefficient. Lidocaine, an ion channel blocker, was administered to patients exhibiting high-frequency decline, while bacitracin, a fibrinogen-reducing drug, was prescribed to those with full-frequency hearing loss, including flat-drop and total deafness. The treatment cycle spanned a period of 7 to 14 days for all patients. If the patient’s hearing recovery remains poor, a hearing aid may be suggested.
Criteria for Judgment of Efficacy
To evaluate treatment success, we compared the patient’s pure-tone audiometry before and after receiving treatment, following established guidelines. 1 Our grading system was based on various factors. We considered the patient cured if their hearing was restored to normal, or reached the level of the healthy ear or pre-disease level after treatment. Improvements over 30 dB were classified as having an obvious effect. An improvement ranging between 15 and 30 dB was deemed effective, while anything less than 15 dB was deemed ineffective. The patients were classified into 2 categories based on their prognosis: those with a poor prognosis (considered ineffective) and those with a good prognosis (considered effective, with an obvious effect or cured). The effective rate was calculated by dividing the total number of cases (effective + apparently effective + cured) by the total number of cases of each type and multiplying by 100%. This gave an effective rate of 100%.
Statistical Analysis
The data collected were presented in 2 forms: count data presented as n (%) and continuous variables presented as mean standard deviation ( ± s). Basic comparative statistics on the variables were performed using SPSS25.0 software. Spearman’s analysis was used to analyze the correlation between the independent variables and the treatment effect. ROC curves were plotted to determine disease prediction thresholds for the subjects’ work characteristics, and the area under the curve was used to estimate diagnostic accuracy. Univariate and multivariate binary logistic regression analyses were performed to evaluate the predictive impact of hematological parameters and various clinical variables on the prognosis of SSNHL.
Results
Clinical Characteristics and Univariate Analysis of Patients With Sudden Deafness
A study was conducted in 414 patients with sudden deafness in 1 ear. The patients ranged in age from 14 to 88 years, with a mean age of 50.10 ± 14.70 years. Of the patients, 183 (44.20%) were male and 231 (55.80%) were female. The left ear was affected in 235 cases (56.76%) and the right ear in 43.20%. Dizziness was reported in 107 cases (25.80%), ear fullness in 164 cases (39.620%), and tinnitus in 247 cases (59.66%). Hearing loss was classified as low frequency in 127 cases (30.68%), high frequency in 53 cases (12.81%), flat in 149 cases (35.99%), and total deafness in 85 cases (20.53%). The group with ineffective treatment exhibited characteristics such as older age, a longer duration from onset to treatment, a higher prevalence of concomitant tinnitus, and higher LDL levels. There were statistically significant differences between the ineffective and effective groups. However, there were no statistical differences in the side of the disease, gender, underlying diseases (such as hypertension or diabetes mellitus), or concomitant ear stuffiness or dizziness.
After a thorough univariate analysis, several factors were found to influence the success rate of treating sudden deafness. These included age, duration of illness, tinnitus, hearing loss curve, degree of hearing loss and triglyceride, LDL, and HDL levels. In contrast, gender, side of the ear affected, ear stuffiness, dizziness, hypertension, and diabetes mellitus had no significant effect on the effectiveness of treatment (Table 1).
Clinical Features and Univariate Analysis.
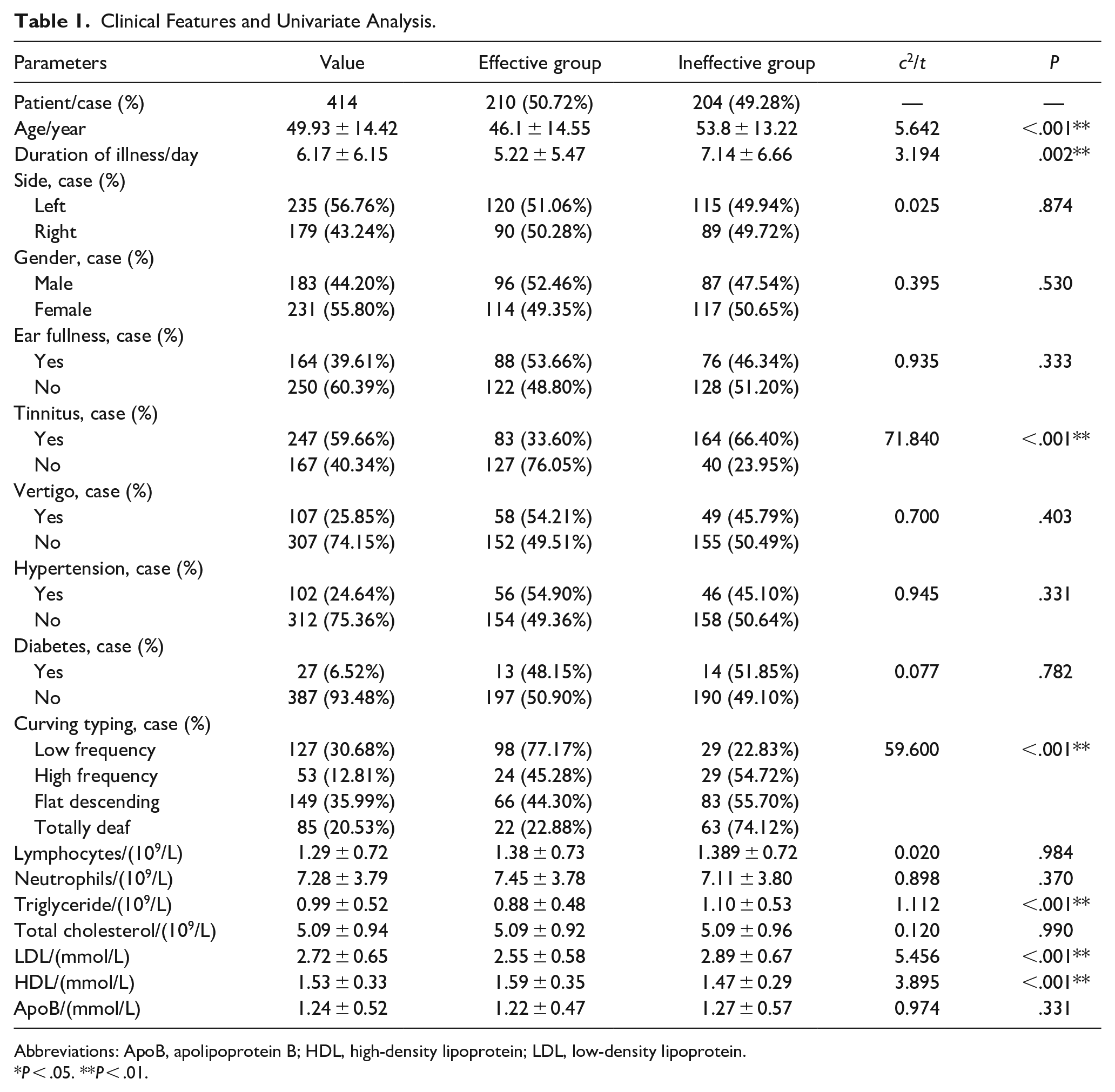
Abbreviations: ApoB, apolipoprotein B; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
P < .05. **P < .01.
Analysis of the relationship between hearing loss and prognosis for different types of hearing curves showed that, except for the total deafness group, all of whom had very severe loss, there were significant differences in treatment efficacy between subgroups with different degrees of hearing loss for each type of curve, with a statistically significant difference in efficacy between the low-frequency group (c2 = 8.446, P = .038), the high frequency group (c2 = 11.275, P = .010), and the flat decline group (c2 = 7.128, P = .049) .The difference was statistically significant, and the higher the degree of hearing loss the lower the effective rate among patients with the same curve type (Table 2).
Analysis of Hearing Loss and Prognosis in Different Curve Types.
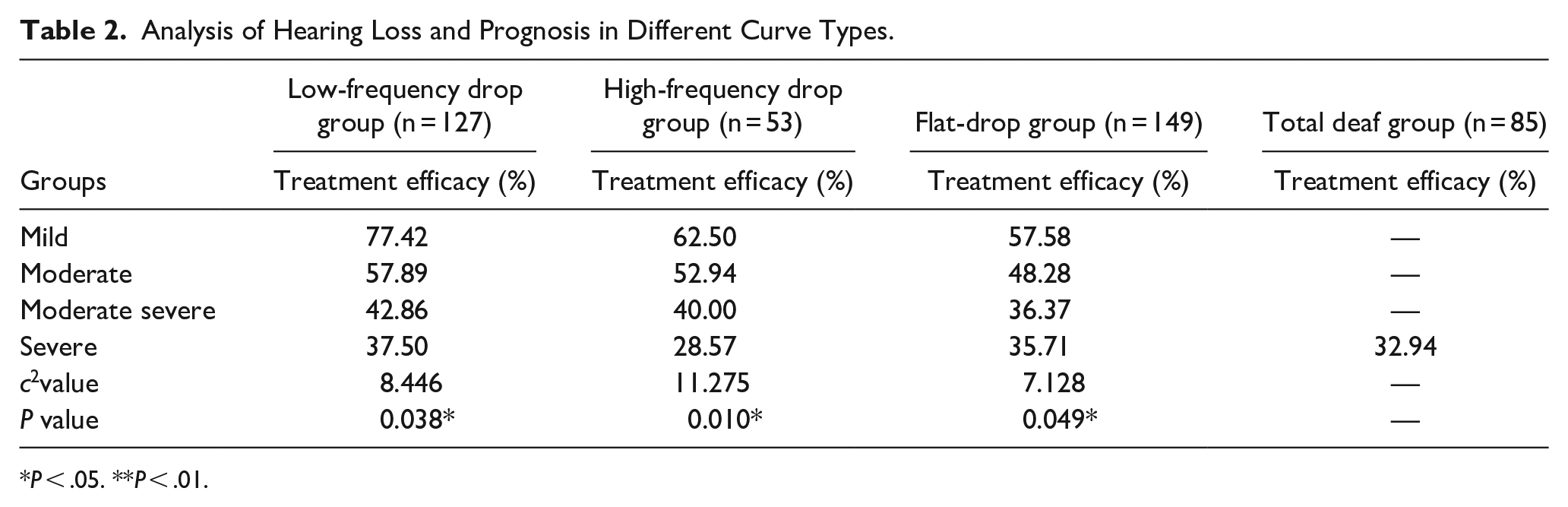
P < .05. **P < .01.
Spearman’s Rank Correlation Analysis
In the first analysis, the significant factors were compared with the efficacy level. The results showed a negative correlation between hearing threshold of at least 81 dB at 250 to 8000 Hz, LDL and triglyceride levels, and prognosis (r < 0, P < .001). Conversely, HDL levels were positively correlated with prognosis (r > 0, P < .001; Table 3).
Correlation Analysis of Influence Factors and Level of Effectiveness.

Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein.
P < .05. **P < .01.
We investigated the prognostic role of age, duration of disease from the onset to the first visit, and LDL level in sudden deafness. We evaluated the receiver operating characteristic (ROC) curve of the participants. ROC curve was presented in Figure 1. The results indicate that age had an area under the ROC curve of 0.647 [95% confidence interval (CI) 0.594-0.699], duration of disease had an area under the ROC curve of 0.585 (95% CI 0.530-0.640), and LDL level had an area under the ROC curve of 0.651 (95% CI 0.598-0.704; Table 4).
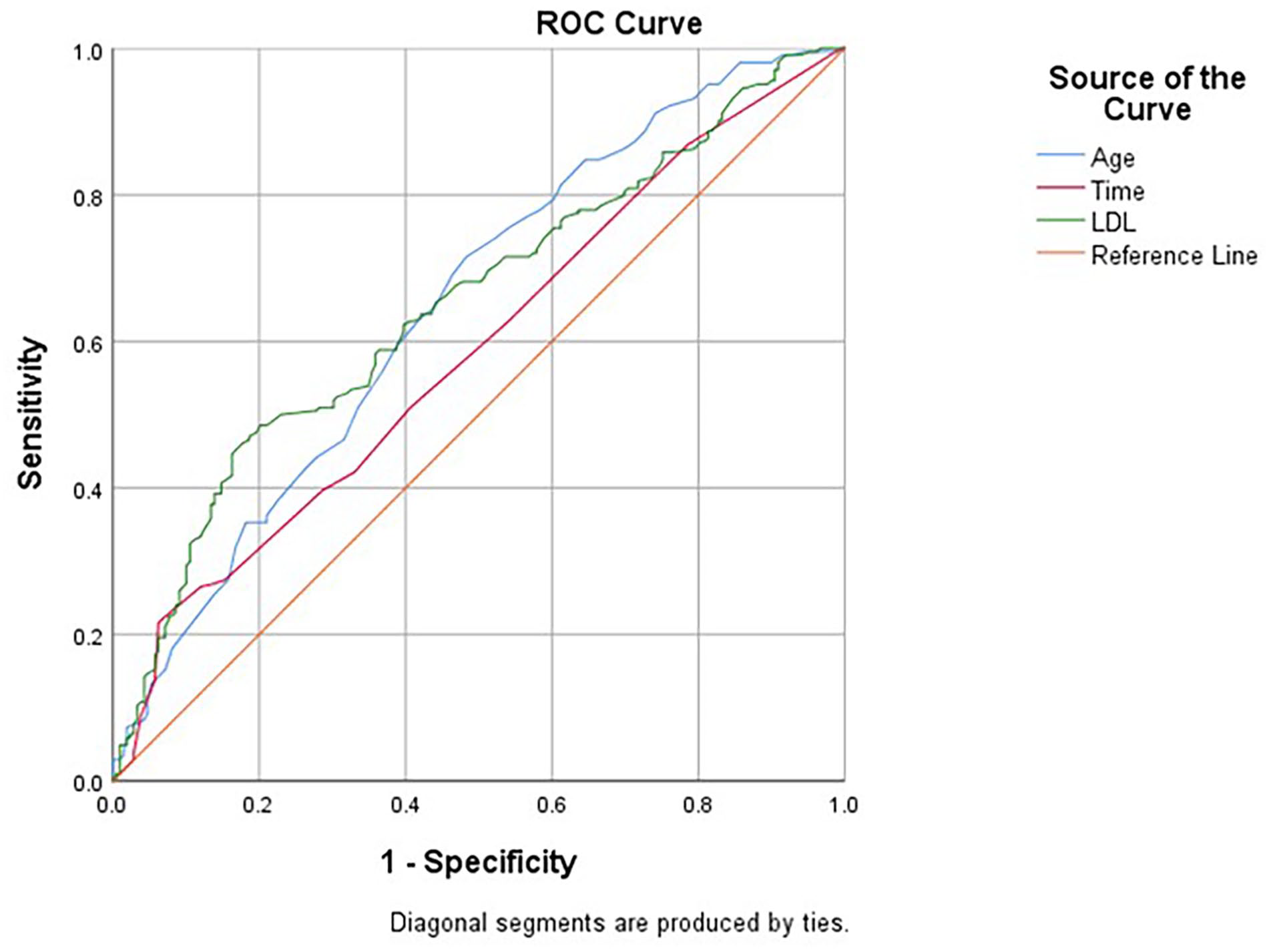
ROC curves for LDL, age, and time to treatment. ROC, receiver operating characteristic; LDL, low-density lipoprotein.
Comparison of the Predictive Value of the Diagnosis of Sudden Deafness.
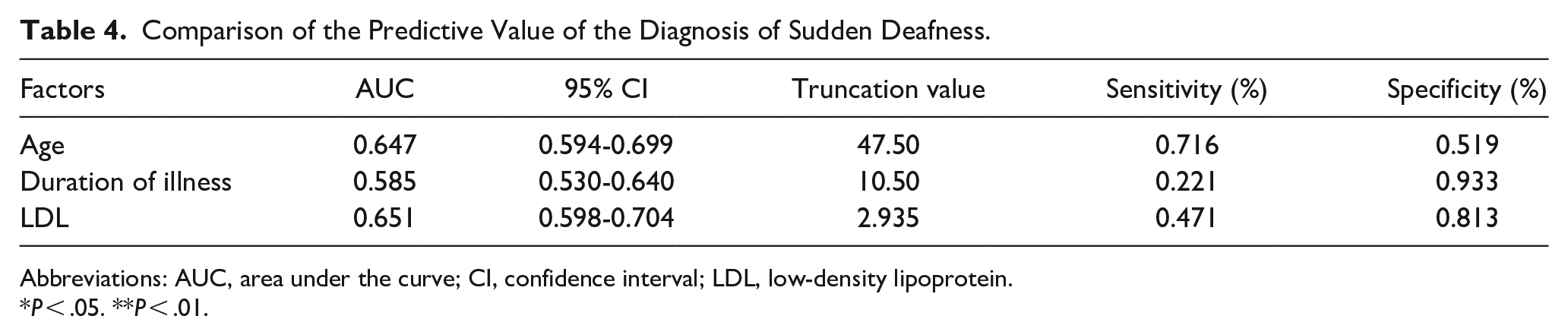
Abbreviations: AUC, area under the curve; CI, confidence interval; LDL, low-density lipoprotein.
P < .05. **P < .01.
Multivariate Logistic Analysis
The multivariate regression analysis took into account the statistically significant factors identified in the univariate analysis. The study revealed independent risk factors that influence the effectiveness of sudden deafness treatment, such as age over 47 years, disease duration of more than 10 days, presence of tinnitus, sudden deafness curve, and LDL level above 2.93 mmol/L (Table 5).
Multivariate Analysis Affecting the Prognosis of Patients With Sudden Deafness.
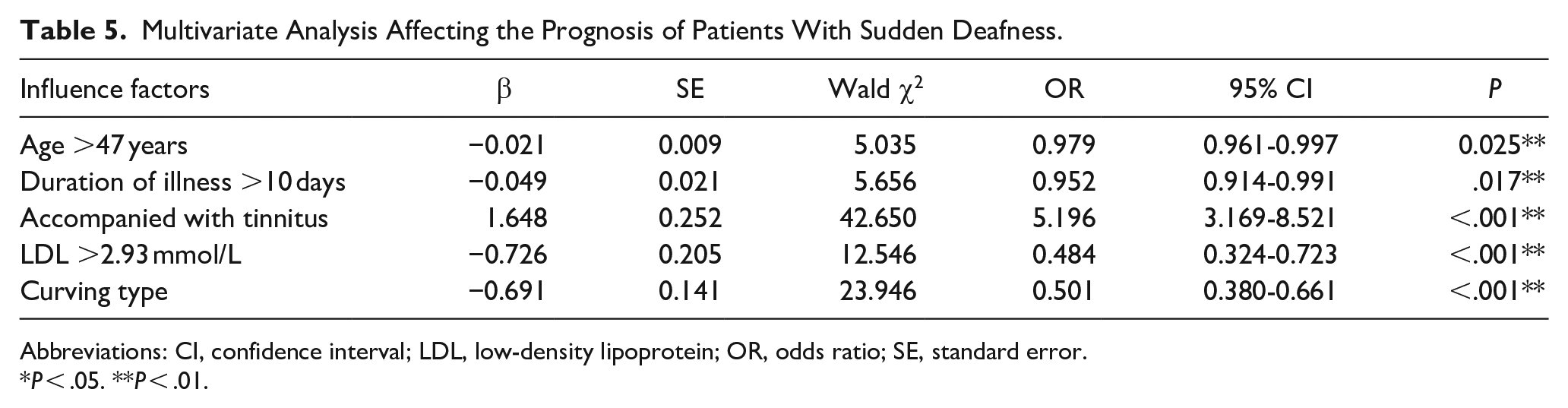
Abbreviations: CI, confidence interval; LDL, low-density lipoprotein; OR, odds ratio; SE, standard error.
P < .05. **P < .01.
Discussion
SSNHL is a common condition in ENT medicine. Its causes are not fully understood and many studies have been conducted to identify factors that influence its prognosis. 4 One area of research has focused on identifying circulating biomarkers of SSNHL, but results have been inconsistent and of low quality. 5 This study aims to comprehensively investigate the clinical features and hematological indicators associated with the prognosis of SSNHL. This information may help guide treatment decisions for patients with sudden deafness.
The study included 414 patients who experienced sudden deafness in 1 ear and sought treatment at the Jiangsu University Affiliated People’s Hospital. The results showed that 50.72% of cases responded positively to treatment, which is in line with the results of previous studies (32%-70%).6,7 Further examination of clinical factors showed that patient age, time from symptom onset to medical intervention, type of sudden hearing loss, degree of hearing loss, and presence of tinnitus were important determinants of patient prognosis.
Sudden deafness can affect people of all ages, as shown in a recent study involving participants aged 14 to 88 years. Interestingly, the study found that patients over the age of 47 years had a less favorable prognosis (t = 5.642, P = .025). This is consistent with previous research suggesting that people over the age of 60 years tend to have lower hearing recovery rates. 8 Various factors affect the prognosis of older patients with sudden deafness, including the increased possibility of having systemic diseases. The function of the inner ear naturally deteriorates with age, which further hinders the recovery process. Moreover, animal experiments have been conducted in this domain. Studies conducted on animals have demonstrated that a substantial number of auditory neurons in the aging ear become detached from their hair cells, resulting in a pathological explanation for this phenomenon. 9 However, research conducted by Zhang and Young 10 has shown that the treatment outcome for elderly patients older than 65 years is not significantly different from that of nonelderly patients aged between 55 and 64 years. The results imply that the aging process has no impact on the outcome of this disease. SSNHL is identified by an abrupt loss of hearing, which may deteriorate gradually. Seeking early consultation, preferably within 1 week of SSNHL onset, has been linked to improved hearing recovery.
Delayed treatment has been linked to a worsened prognosis. 11 Studies have indicated that putting off treatment for sudden hearing loss can lead to a less favorable outcome. 11 Several studies have found that the probability of recovery rises with decreased illness duration.12,13 Our investigation confirms this finding, as we observed that seeking medical care within 10 days of symptom onset led to more positive treatment outcomes.
Regarding the correlation between the type of hearing curve decline and prognosis, Byl 14 suggested in 1984 that the hearing curve of patients is significantly associated with the prognosis of sudden deafness. Our analysis reveals that patients with diverse types of hearing curves exhibit various levels of treatment effectiveness, which is statistically significant (t = 59.600, P < .001). Patients with low-frequency hearing decline have the highest treatment effectiveness rate at 77.17%, whereas those with high-frequency decline have an effective treatment rate of 45.28%. The flat type of decline presents the second-worst treatment effect at 44.30%, while the total deafness type has the worst treatment effect, with an effective rate of only 22.88%. These findings align with prior research. 15 Cochlear apex lesions which result in hearing loss at low and medium frequencies have better blood supply, thereby leading to a superior ability to restore hearing function.
On the contrary, in cases of high-frequency hearing loss, hair cells located at the base of the cochlea experience greater sensitivity, thereby making the restoration of high-frequency hearing function more difficult. 16 High-frequency hearing thresholds decline more rapidly than low-frequency hearing thresholds with age, 17 leading to a negative feedback loop between the loss of high-frequency hearing and poor restoration that further affects the treatment effect. In addition, we conducted an analysis of the degree of hearing loss and prognosis of patients with each hearing curve type separately and found that the prognosis of patients exhibiting more severe hearing loss was worse within the same curve type.
The association between lipid levels and the prognosis of sudden deafness remains uncertain, with inconsistent findings across studies. Nevertheless, research on SSNHL biomarkers has yielded prognostic indicators. The study of Silky et al 18 found a negative correlation between average LDL levels and prognosis, which is supported by the results of this study. Elevated levels of LDL in the bloodstream pose a risk factor for the development of atherosclerosis. 18 This affliction can cause an increase in blood viscosity, microvascular inflammatory response, ischemia, and even thrombosis. As atherosclerosis disproportionately impairs the supplying vessels to the inner ear, it can likely obstruct blood supply. 19 Notably, there is no established threshold value for LDL that may directly affect SSNHL prognosis. Our analysis has revealed that an LDL level greater than 2.93 mmol/L is an autonomous risk element for sudden deafness prognosis. One factor that can potentially worsen the prognosis of SSNHL is hyperlipidemia, which may represent a basis for early clinic intervention. To enhance the prognosis of SSNHL, certain experts advise the reduction of LDL levels through blood purification.20,21 However, there is no definitive guidance on whether to administer lipid-lowering therapy to patients, and this study merely demonstrates that dyslipidemia is a potential prognostic risk factor. Further research is needed to establish whether targeted lipid-lowering therapy is crucial for such patients.
Tinnitus is the perception of sound in the ear or brain, which patients report even in the absence of external sound or electric stimulation in the surrounding environment. 22 The prevalence of tinnitus varies among studies due to the absence of transparent diagnostic criteria. About 80% of sudden deafness patients have reported experiencing tinnitus. 4 However, the study uncovered a 59.66% incidence of tinnitus with a significantly lower treatment efficiency (33.60%) among patients with tinnitus compared to those without (76.05%), as evidenced by statistical significance (t = 71.840, P < .001). The lower incidence observed in this study compared to earlier reports may stem from the age of the enrolled patients, considering that tinnitus incidence rises with age and is more prevalent among those older than 40 years. The average age of patients with tinnitus who participated in this study was 43.64 ± 14.35 years, which is below the mean age reported in other studies with a high prevalence of tinnitus. 23 However, the study’s limitations prevented the ability to conduct a multicenter clinical study which could have affected the results. Tinnitus is a subjective sensation and lacks clear diagnostic criteria. Some patients may not report experiencing tinnitus due to its subtle nature. Moreover, tinnitus may develop slowly over time, and patients who developed tinnitus after hospital admission were not accounted for in the statistical analysis. Tinnitus affects the functioning of the cochlea and may lead to persistent arousal of the patient’s autonomic nervous system. In addition, it has been linked to multiple comorbid conditions, particularly anxiety and depression. 24 The severity of tinnitus is known to escalate as the disease progresses. It can lead to negative psychological reactions, affecting both a patient’s personal and professional life. Consequently, it is imperative for counseling and psychoeducation to be administered when treating tinnitus. High-frequency hearing loss, 25 in particular, poses a significant risk factor for tinnitus. Nevertheless, it remains uncertain whether hearing loss alone is the sole risk factor. High-frequency hearing impairment is also harder to improve. To sum up, tinnitus negatively affects the forecast of sudden deafness patients.
To summarize our study, the analysis has identified that individuals older than 47 years, those who seek treatment more than 10 days after the onset of symptoms, and those with total deafness type curve hearing loss, significant hearing loss, concurrent tinnitus, and LDL levels exceeding 2.93 mmol/L are at an increased risk of experiencing a poor prognosis in sudden deafness cases. Therefore, healthcare practitioners should observe these patients and offer prompt interventions to enhance their prospects of recuperation.
Supplemental Material
sj-xlsx-1-ear-10.1177_01455613241232796 – Supplemental material for A Comprehensive Study on Sudden Deafness for Analyzing Their Clinical Characteristics and Prognostic Factors
Supplemental material, sj-xlsx-1-ear-10.1177_01455613241232796 for A Comprehensive Study on Sudden Deafness for Analyzing Their Clinical Characteristics and Prognostic Factors by Kaiwei Yao, Muhammad Asad Iqbal, Nida Fatima Moazzam and Wei Qian in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
The authors would like to thank Yao Kaiwei for helpful research discussions and reference suggestions. Muhammad Asad Iqbal and Nida Fatima Moazzam for writing discussions. Qian Wei for proofreading the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.