
Abstract
Poor blood glucose control is a common predisposing factor for parotid abscesses; however, extensive skin necrosis secondary to parotid abscesses has rarely been reported. In this article, we present the case of a 70-year-old man with poor glycemic control admitted to our hospital with swelling, congestion, and pain in the right parotid region that had gradually increased over 15 days prior to presentation. Based on the clinical, imaging, and laboratory findings, the patient was diagnosed with a giant parotid abscess with extensive skin necrosis caused by Klebsiella pneumoniae. The abscess responded poorly to long-term treatment with intravenous broad-spectrum antibiotics, and the patient underwent daily Bacillus exchange with blood glucose level management and electrolyte monitoring via routine blood tests. At the 3 month follow-up, complete resolution of the right parotid gland abscess and skin rupture was observed.
Introduction
Parotid abscesses are usually associated with infections caused by bacteria, fungi, and viruses. Poor blood glucose control is a common predisposing factor for parotid abscesses; however, extensive skin necrosis secondary to parotid abscesses has rarely been reported. 1 Herein, we report the case of a patient with diabetes with poor glycemic control and extensive subcutaneous necrosis secondary to a right parotid abscess. Because no similar case of extensive parotid abscess has been reported in the literature, we present the relevant treatment.
Case Report
A 70-year-old man was admitted to our hospital with swelling, congestion, and pain in the right parotid region that gradually increased over the 15 days prior to presentation. In addition, the patient had fever, headache, limited mouth opening, lethargy, and poor appetite and was reluctant to swallow because of the pain and discomfort. Clinical examination revealed diffuse swelling in the right parotid region, approximately 4 cm × 5 cm in size. Surface ulceration was observed, and the local skin temperature was elevated (Figure 1a).
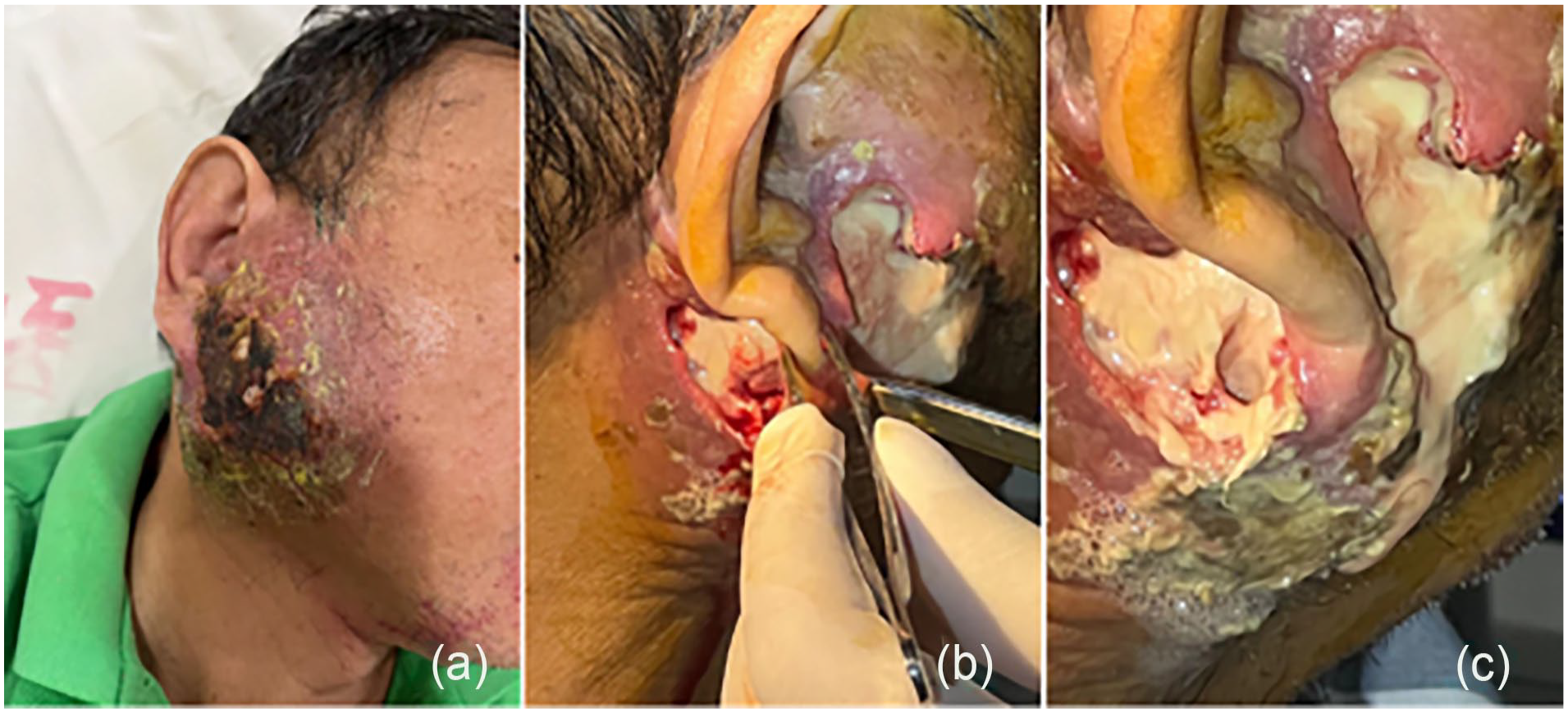
The patient’s right parotid gland before the application of BAIKERUI gauze wound dressing. (a) On hospital admission. (b) Debridement and drainage. (c) After regular dressing changes for 1 week.
On July 12, 2023, ultrasound of the right parotid gland revealed heterogeneous echotexture with intraparotid lymphadenitis, and an enlarged lymph node in the right parotid gland was suspected. The right parotid edema worsened, and suppuration was observed on the surface, which was not controlled after half a month, despite administration of intravenous broad-spectrum antibiotics. The abscess gradually worsened, penetrated the fascia to reach the deep lobe of the parotid gland, deep cervical fascia, external auditory canal, and anterior wall of the mastoid process. Furthermore, it extended outward into the facial skin, leading to skin breakdown.
Medical History
The patient had been diagnosed with diabetes mellitus and hypertension 15 and 20 years prior, respectively, and was taking nifedipine extended-release tablets orally, comprising 1 pill every morning. On admission, the fasting blood glucose level and blood pressure were 22 mmol/L and 120/80 mmHg, respectively.
Diagnostic Tests
Pus culture performed on July 24, 2023, revealed Klebsiella pneumoniae infection.
On July 25, 2023, enhanced computed tomography of the right parotid region (Figure 2) revealed a diffusely enlarged right parotid gland with a hypodense shadow measuring approximately 7.3 cm × 5.4 cm and multiple circular enhancements. In addition, extensive small gas bubbles under the skin, local epidermal breakdown, and slight thickening of the anterior commissure space were observed. However, no bone destruction was observed in the adjacent mandible.
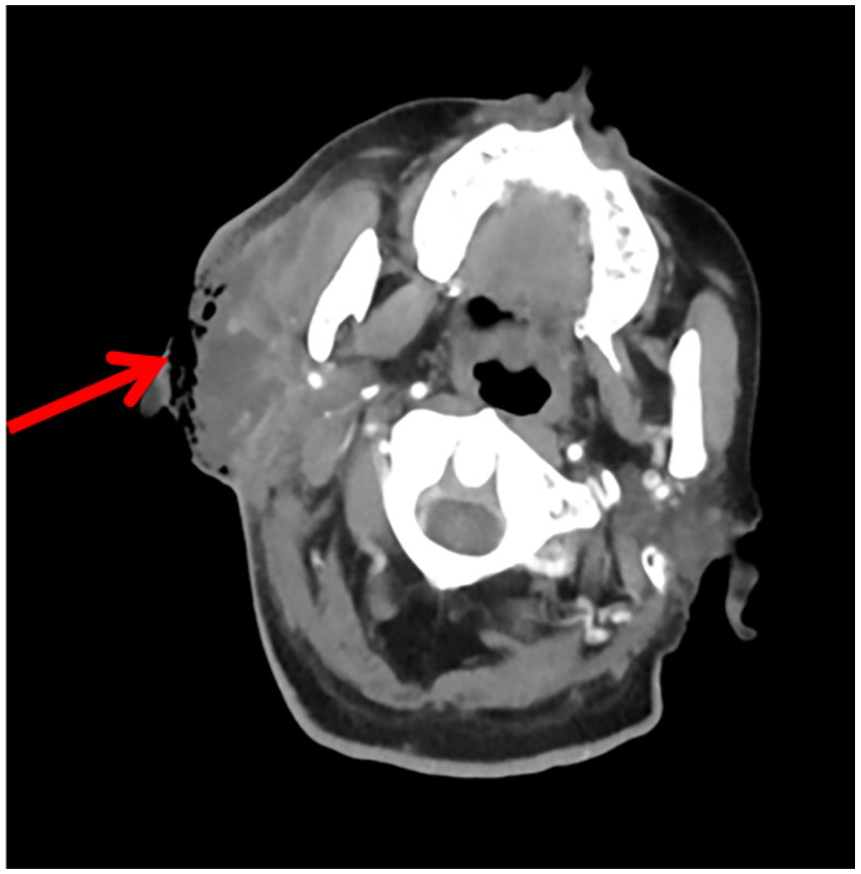
Enhanced computed tomography on admission showing a massive lesion in the right parotid gland along with local skin defects.
Diagnosis
Based on the clinical, imaging, and laboratory findings (Table 1), the patient was diagnosed with a giant abscess in the right parotid gland, uncontrolled diabetes mellitus, hypoproteinemia, and electrolyte disturbance.
Laboratory Test Findings.
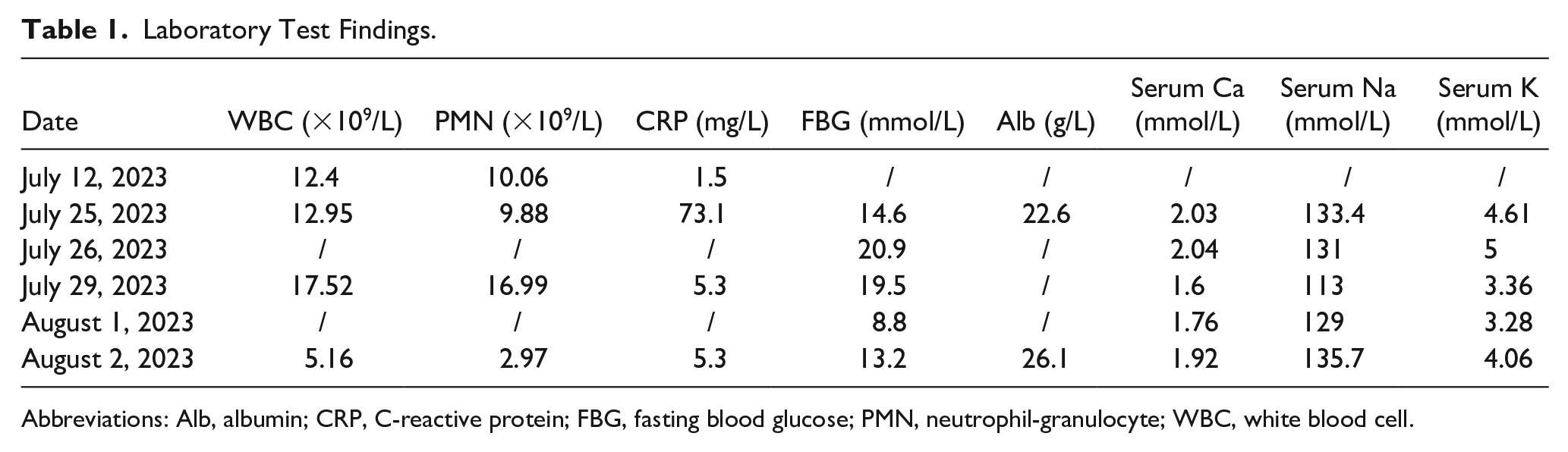
Abbreviations: Alb, albumin; CRP, C-reactive protein; FBG, fasting blood glucose; PMN, neutrophil-granulocyte; WBC, white blood cell.
Treatment
Cefazolin (2 g) and moxifloxacin (0.4 g) were administered intravenously. Massive rehydration, transfusion of 10 g/day of human albumin, insulin pump for glucose control, and regular blood retesting to assess the electrolyte levels were performed.
The patient was hospitalized for 10 days with daily wound dressing to debride the necrotic fascia; however, the rupture size increased (Figure 1b and c). Subsequent application of the BAIKERUI gauze wound dressing decreased wound leakage and necrosis, thereby fostering wound healing (Figure 3a–e).

The patient’s right parotid gland after application of a BAIKERUI gauze wound dressing. (a) After wound dressing using BAIKERUI gauze for 1 week. (b) Debridement and drainage after 2 weeks of bacitracin use. (c) After wound dressing using BAIKERUI gauze for 3 weeks. (d) After wound dressing using BAIKERUI gauze for 4 weeks. (e) After wound dressing using BAIKERUI gauze for 7 weeks. (f) BAIKERUI gauze wound dressing.
Follow-Up
At the 3 month follow-up, complete resolution of the right parotid gland abscess and skin rupture was observed.
Discussion
Parotid abscesses caused by acute parotid infection are common; however, a large skin defect secondary to a parotid abscess has not been reported to date. The major challenges we encountered during treatment of this case were refractory hyperglycemia that led to abscess enlargement, electrolyte disturbances, and hypoproteinemia. The glucose-lowering regimen required several adjustments, and the patient’s blood glucose level was controlled 1 week after admission. The patient had a large skin defect with necrotic margins, which made a flap graft difficult. Therefore, conservative treatment comprising daily wound dressing using BAIKERUI gauze to remove the necrotic tissue was administered. Sepsis was avoided by effectively managing infection and avoiding drug resistance.
Diabetes mellitus is a predisposing and aggravating factor for parotid abscesses, and inadequate glycemic control can exacerbate these abscesses. Considering that infections originating from the deep cervical space can result in mediastinitis and facial nerve palsy,2,3 endocrinology consultation is crucial for regulating blood glucose levels and preventing abscesses formation. 4
The treatment of parotid abscesses consists primarily of incision and drainage with antibiotic and anti-inflammatory therapies. However, incision and drainage is not feasible in all patients with parotid abscesses, particularly in those with large parotid abscesses. BAIKERUI gauze wound dressing comprises a cotton gauze impregnated with staphylococcal enzyme and lysozyme that effectively inhibits bacterial growth on the wound surface, thereby promoting wound repair. 5 In this patient, the blood glucose level was actively regulated, and the BAIKERUI gauze surgical wound dressing applied to the wound to inhibit abscess formation and promote wound healing.
The findings in this case show that routine blood monitoring with active blood glucose control, correction of electrolyte disorders and hypoproteinemia, debridement, drainage, removal of necrotic tissue, regular dressing changes, use of gauze trauma dressings, and multidisciplinary treatment are crucial for resolution of large parotid abscesses.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Pudong New Area health system leading talent training program (Grant No. PWRI2021-07) and Pudong New Area Clinical Characteristic Discipline (Grant No. PWYts2021-15).
Patient Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Data Availability Statement
All data generated or analyzed during this research are included in the published article. Data supporting the findings in this study are available from the corresponding author on reasonable request.