
Abstract
Introduction:
Infantile hemangiomas (IHs) are the most common tumor of the parotid gland in children; however, there is no standard protocol for the treatment of IH. The generally accepted practice is to begin the patient on β-blocker therapy if there are no contraindications.
Objective:
The purpose of this study is to better understand the challenges and successes of management of pediatric patients with parotid IH.
Methods:
This retrospective study analyzed 15 patients diagnosed with parotid IH from 2009 to 2016 who were cared for at a tertiary care center. Demographic information, lesion characteristics, and treatment course were obtained through patient chart review.
Results:
Fifteen pediatric patients with parotid IH were evaluated. The female:male ratio was 4:1; the average age of diagnosis was 8.75 months. Most lesions were greater than 3 cm in their widest dimension (73.3%), and 13 patients underwent imaging to further clarify the parotid mass in their clinical workup. Fourteen patients began treatment with propranolol; 10 patients saw complete resolution of their IH (66.7%) and 3 had a partial response to β-blocker therapy (20%). After discontinuation of propranolol, 2 patients had regrowth 2 to 3 months later after regression and were restarted on therapy. The average duration of treatment was 9.9 ± 8.45 months. The known adverse effects of propranolol—hypoglycemia, hypotension, bradycardia, and bronchospasm—were not observed in any patient.
Conclusion:
In the treatment of parotid IH, propranolol is the generally accepted first-line therapy, as compared to corticosteroid or interferon α injections of years past. Parotid hemangiomas, however, have a lower response rate to propranolol and a similar recurrence rate compared to IH at other sites. The treatment duration necessary tends to be longer. Future studies will aim at identifying and evaluating potential predictors of outcomes to help inform the management of parotid hemangiomas.
Introduction
Infantile hemangiomas (IH) are the most common tumor of the parotid gland in children. In the 1970s, parotid gland tumors in infants and children were primarily managed with surgical removal of the primary tumor. It is reported that the majority of cases of IH involute spontaneously along a predictable timeline, with about 10% requiring active management. However, parotid gland IHs have also been reported to involute more slowly and with less satisfactory outcomes than IHs at other sites. 1
There is no gold standard for the treatment of pediatric IH of the head and neck, and particularly of the parotid gland. The generally accepted practice, however, is to begin the patient on β-blocker therapy if there is no cardiac contraindication to treatment. Treatment strategies fall into 3 categories: active nonintervention, pharmacological, and surgical. Factors considered in determining the treatment plan include size, stage, location, presence of ulceration and bleeding, functional obstruction, and risk for deformity. In cases in which watchful waiting is deemed appropriate, the lesion is observed and progression is recorded with photography. Providers may consider intervention if worrisome changes arise.
Historically, pharmacologic treatment has included the use of corticosteroids, interferon α-2a, imiquimod, becaplermin, and chemotherapeutic medications. Corticosteroids and interferon α-2a are typically injected intralesionally. 2 The oral administration of propranolol has provided a paradigm shift in the medical treatment of IH. Patients treated with propranolol have demonstrated significant improvement, even after a short course of treatment. 3 Oral propranolol has been shown to be well tolerated by patients, and adverse effects tend to be minor in appropriately selected patients. 4
This study contributes to the currently available literature by reporting our institutional experience in the challenges and successes of management of pediatric patients with parotid IH. Identifying and evaluating potential predictors of outcomes including type of treatment, number of surgical procedures, comorbidities, and analyzing quality of life measures will help inform the treatment and management that could potentially improve patient outcomes.
Patients and Methods
A retrospective chart review was performed on pediatric patients treated at Monroe Carell Jr. Children’s Hospital at Vanderbilt for hemangiomas between 2009 and 2016. Out of a panel of 489 pediatric patients with hemangiomas, 15 patients met inclusion criteria of a parotid hemangioma diagnosis or involvement of the parotid gland. Demographic information (age at diagnosis, gender, gestational age, race/ethnicity, medical history) were collected on these patients, in addition to characteristics of their clinical and treatment courses (lesion location, size, imaging performed, age at treatment initiation, treatment duration).
Results
Patient Demographics
For this study, 15 patients with parotid hemangiomas were evaluated (Table 1). Twelve (80%) patients were female, and 3 (20%) patients were male. The average age at diagnosis was 8.75 months, with a standard deviation of 6.48 months. The oldest patient was 22.8 months, with the youngest at 1.2 months at diagnosis. The majority of patients were Caucasian (60%), with 1 patient of African American and Asian descent each. Two-thirds of the patients were non-Hispanic (66.7%), while a smaller percentage (13.3%) were Hispanic. Two patients had a positive family history for cardiac abnormalities or hemangioma. Only 1 patient had an additional diagnosis of an associated syndrome, which was PHACES (Posterior fossa anomalies, Hemangioma, Arterial lesions, Cardiac abnormalities, and Eye anomalies). As part of her syndrome, this patient also had a posterior fossa malformation, cardiac defects, and eye abnormalities.
Patient and Lesion Characteristics.
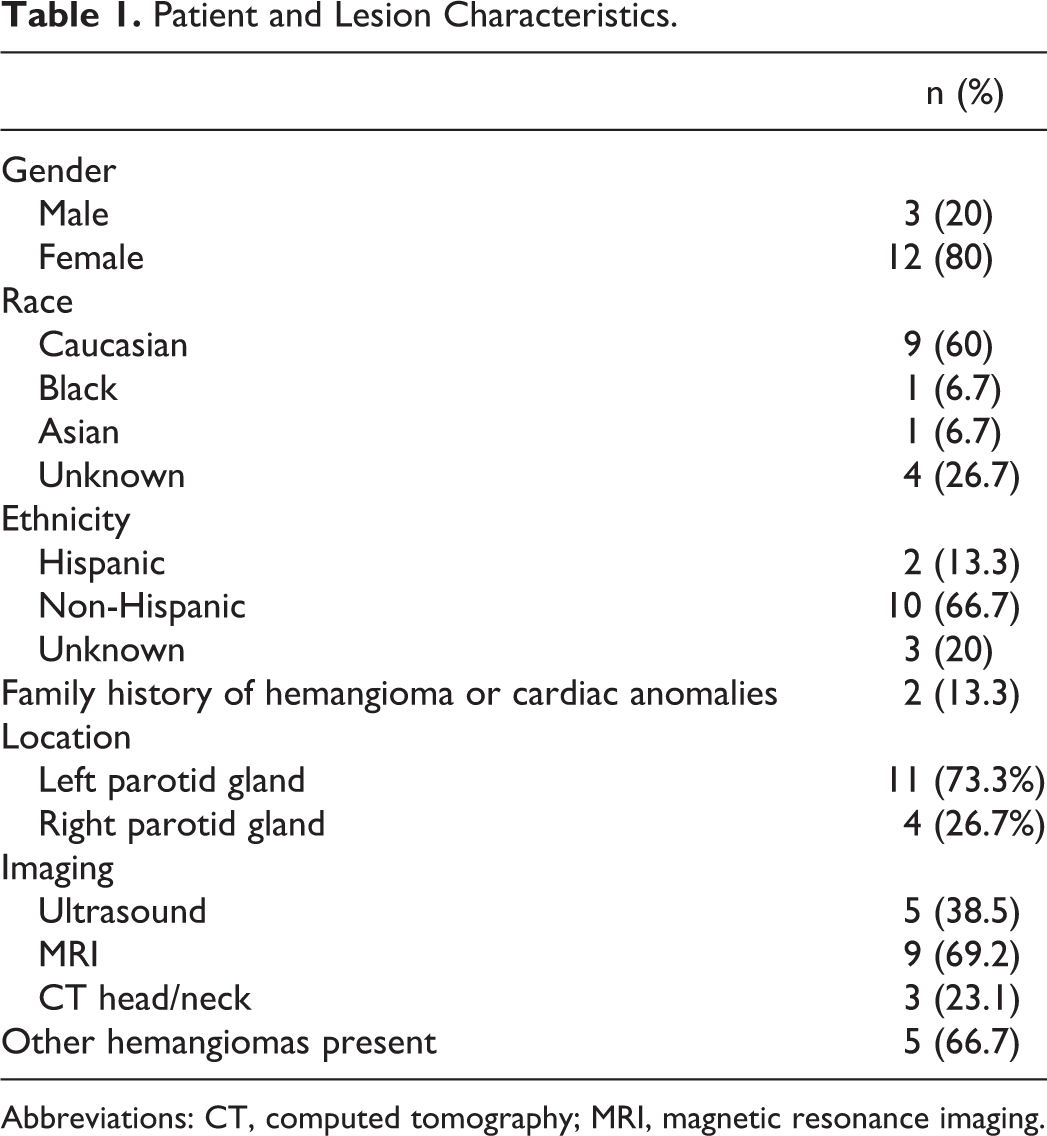
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging.
Lesion Characteristics
The majority of patients had a left parotid gland hemangioma (73.3%), compared to the right parotid gland (26.7%). Zero percent were bilateral. Most lesions were greater than 3 cm in their widest dimension (73.3%), with the average width about 4 cm. One lesion was less than 5 mm, 2 lesions were between 1 and 2 cm, and 1 lesion was between 2 and 3 cm. Thirteen of the 15 patients in this study underwent imaging to further clarify the parotid mass in their clinical workup. Five patients had an ultrasound (38.5%), 9 patients had a magnetic resonance imaging (MRI; 96.2%), and 3 patients had a head and neck computed tomography (CT) scan (23.1%). Four patients received more than 1 type of imaging study. Three received an ultrasound examination followed by either an MRI or CT, whereas the patient with the PHACES syndrome had both MRI and CT scans performed.
Most lesions were described as soft and noncompressible, with overlying blue-purple skin color changes. Some had areas in the mass that were firm, consistent with fibrosis. No hemangiomas exhibited ulceration or were tender to palpation. All function of the facial nerve on the effected side was intact. The primary indication for treatment was disfigurement. None of the lesions proposed a risk of functional impairment or became ulcerated or bled. Five patients in the study had additional hemangiomas present in other locations on their body (33.3%). These locations were the upper back, left frontal scalp, left upper lip, right anterior chest wall, and midline anterior scalp. Upon initiation of treatment with propranolol, these lesions also regressed in size in addition to the parotid IH.
Treatment Course
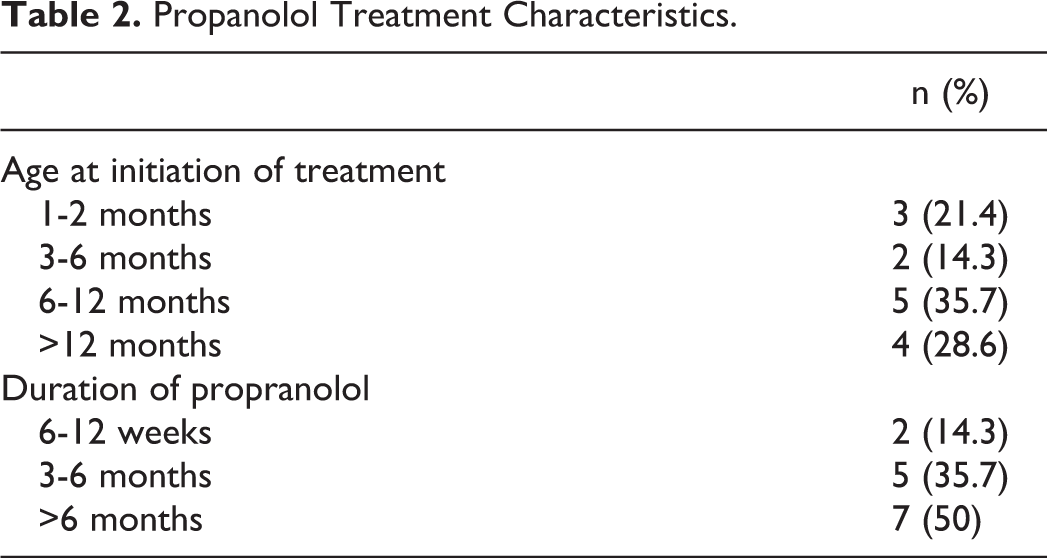
Of the 15 patients with parotid IH, 14 patients began treatment with propranolol at a dose of 2 mg/kg/d (Table 2). One patient did not start β-blocker therapy but was managed conservatively with no treatment and the hemangioma was left to involute. Median age at initiation of propranolol treatment was 9.9 months (interquartile range: 5.4-16.7 months). The oldest patient was 3 years old, and the youngest was 4 weeks old. The majority of patients continued the propranolol for more than 6 months (50%), 2 patients took propranolol for less than 6 months (14.3%), and 5 patients were treated between 3 and 6 months. The average length of time was 9.86 months of treatment, with a standard deviation of 8.49 months. The shortest time frame was 3 months, and the longest was 17 months, excluding the patient with PHACES syndrome who was on continual propranolol medicine. Of the patients who took propranolol, 3 had a partial response to treatment (20%) and 10 patients had a complete response (66.7%) where the IH regressed entirely. At the time the study was performed, the treatment for 2 patients (13.3%) was ongoing with clinical improvement. Upon discontinuation of propranolol, 2 patients had recurrence of IH 2 to 3 months later. These patients were restarted on β-blocker therapy. Two patients also completed a full course of antibiotics prior to starting propranolol.
Propanolol Treatment Characteristics.
Of the 12 patients who started and completed propranolol treatment, 2 patients discontinued the medication with a 2-week wean period (16.7%). Ten patients discontinued the medication abruptly with no wean period (83.3%). No adverse events were observed when the propranolol was stopped, such as rebound tachycardia. None of the patients in this study underwent surgery as part of their treatment course.
Discussion
Clinically, parotid gland hemangiomas present as asymptomatic soft tissue swellings that cause the overlying skin to obtain a bluish hue. 5,6 They have the potential to enlarge and cause serious facial deformities impacting the eyes or facial nerve dysfunction. Associated cutaneous involvement is also common. 7 The lesions in this study did not cause any serious functional impairment and were not associated with ulceration, hemorrhage, or infection. Diagnosis of IH is typically made upon physical examination and clinical history, but imaging modalities can aid the diagnosis in equivocal cases. In this study, ultrasound was a first line since parotid hemangiomas are usually hypoechoic relative to parotid tissue, followed up with either CT or MRI to gain useful information on the size, depth extent of the tumor, and relationship to nearby structures. 4
Despite the lack of studies directly comparing propranolol to the previous medical gold-standard treatment of corticosteroids, propranolol is considered as first-line treatment in all infants with problematic hemangiomas. 4 A randomized controlled trial of 460 infants with severe proliferating hemangiomas requiring systemic therapy began on a dose of 3 mg/kg/d, where 88% of infants showed improvement by week 5 of treatment. 8 Higher response rates to propranolol have been seen in patients less than 1 year of age with IHs, as compared to those over 1 year of age (97% vs 74%). 9 In our patient population, the parotid hemangiomas had an overall lower treatment response rate and longer treatment course. This lower response rate could be due to the lower dosage that the patients were on compared to a higher dosage for more severe hemangiomas in other locations. Parotid hemangiomas themselves may also be less responsive to β-blockers than IH at other sites. Similar to our results, studies show that 10% to 30% of IH relapse after cessation of propranolol treatment. 10 Infantile hemangiomas in other locations have been shown to resolve in less time, with significant shrinkage of the lesion occurring within the first month of therapy. 3 Future studies will aim at identifying and evaluating potential predictors of outcomes to help inform the management of parotid hemangiomas.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.