
Abstract
Keywords
Introduction
The main goal of surgery in chronic otitis media (COM) is to achieve a safe and dry ear and restore hearing. Ossiculoplasty is a common procedure performed for hearing restoration. According to the existing literature, 1 incorporating the malleus in the reconstruction and maintaining a hydraulic lever are important for greater acoustic gain. Therefore, we developed a surgical strategy based on the principle of preserving the original ossicular chain as much as possible. There was much literature about the importance of stapes2-4,5 but limited research is available on the malleus. The condition of the middle ear is a major factor that may affect the outcome of the ossiculoplasty. However, based on our surgical strategy, patients requiring ossiculoplasty had a relatively poor middle ear condition. This study aimed to examine the factors, especially the malleus influencing the outcome of ossiculoplasty in patients with COM.
Materials and Methods
Ethical Committee Approval
This study was approved by the Research Ethics Committee of our institution on March 10, 2021 (protocol number IRB110-042-B).
Patients
This is a retrospective analysis of a surgical strategy based on the maximum possible preservation of the original ossicular chain. We included 520 COM patients who underwent middle ear surgery at our institution between January 2010 and December 2019. In 79 of these patients, the original ossicles were not preserved based on the surgical strategy, and ossiculoplasty was performed for the maximum possible preservation of the ossicular chain. This is described further in the next subsection. In the case of tympanic membrane perforations, the infection was controlled with antibiotics. Preoperatively, all cases had non-discharging ears. Computed tomography (CT) was performed in all cholesteatoma cases and when the ABG > 30 dB. All the patients received hearing tests 3 months postoperatively and were followed up for at least 1 year. Hearing tests were repeated if the patients complained of hearing deterioration during the follow-up.
The compromised middle ear condition is defined as follows: Class I: patients with tympanic membrane adhesion with promontory eardrum adhesion without cholesterol granuloma or cholesteatoma; Class II: cholesterol granuloma in the middle ear or mastoid, with or without tympanic membrane adhesion, and without cholesteatoma; and Class III: cholesteatoma in the middle ear or mastoid, which may also be accompanied by other middle ear pathologies, such as cholesterol granuloma or adhesive otitis media. All 3 classes were defined as having a compromised middle ear (Group A). Those with uncompromised middle ears were referred to as Group B. The following clinical data were extracted from the charts of the patient: preoperative audiogram, ossicular status (preserved stapes or not), reconstruction methods (interposition or columella), and postoperative audiogram after 3 months. The hearing results were reported using a four-frequency (500, 1000, 2000, and 4000 Hz) pure-tone average air-bone gap (ABG) to avoid the acoustic radiation effect in high frequencies. Successful surgery was defined as ABG < 25 dB with better hearing results.
Surgical Procedure
All surgeries were performed by a single surgeon. All patients were operated on under general anesthesia using a postauricular approach. Areolar tissue was obtained for harvesting fascia. The perforation was visualized and denuded. A tympanomeatal flap was elevated medially, and the middle ear was accessed. The canal was widened, an antrotomy was made, and the atticoantral route was checked. A canal wall-down mastoidectomy was performed. The ossicular chain was explored and checked. If the ossicular chain continuity was not destructed, the ossiculoplasty was not performed and the pathological tissues were removed as much as possible, unless the removal of some ossicular portions (eg, incus) was also necessary to completely eradicate the cholesteatoma. After removing the cholesteatoma or destructed ossicles, if the malleal manubrium or stapedial suprastructure was present, it was used as much as possible as a part of the reconstructed ossicular chain. Interposition or columella reconstruction was chosen according to the defect, as per the modified Wullstein classification. 6 If the malleus and suprastructure were intact, a type III minor columella tympanoplasty with incus interposition was performed; the lenticular process and short crus of the incus were drilled down and sculptured to fit the distance between the malleus and the stapes capitulum and then interposed. If the suprastructure of the stapes was lost but the malleus manubrium was present, a type III major columella tympanoplasty with incus or malleus head interposition was performed between the malleus manubrium and footplate. If the footplate was absent, a type Vb tympanoplasty with incus or malleus head interposition was performed between the oval window with a fascia and the malleus manubrium. If the malleus manubrium was absent, a columella with incus or malleus head was chosen. Thus, the reconstructed ossicular chain was performed by preserving or utilizing the remaining malleus in all cases with the presence of the malleus manubrium. The incus lenticular process was ground down, and the short process touched the capitulum, footplate, or oval window; the body was then attached to the fascia and tympanic membrane. If the incus was absent, the malleus head was chosen and sculptured as required. If the incus and malleus head were both absent, the cortical bone was chosen for the interposition of the columella. After ossiculoplasty, the tympanomeatal flap was repositioned with the harvested fascia inserted as an underlay (Figure 1).
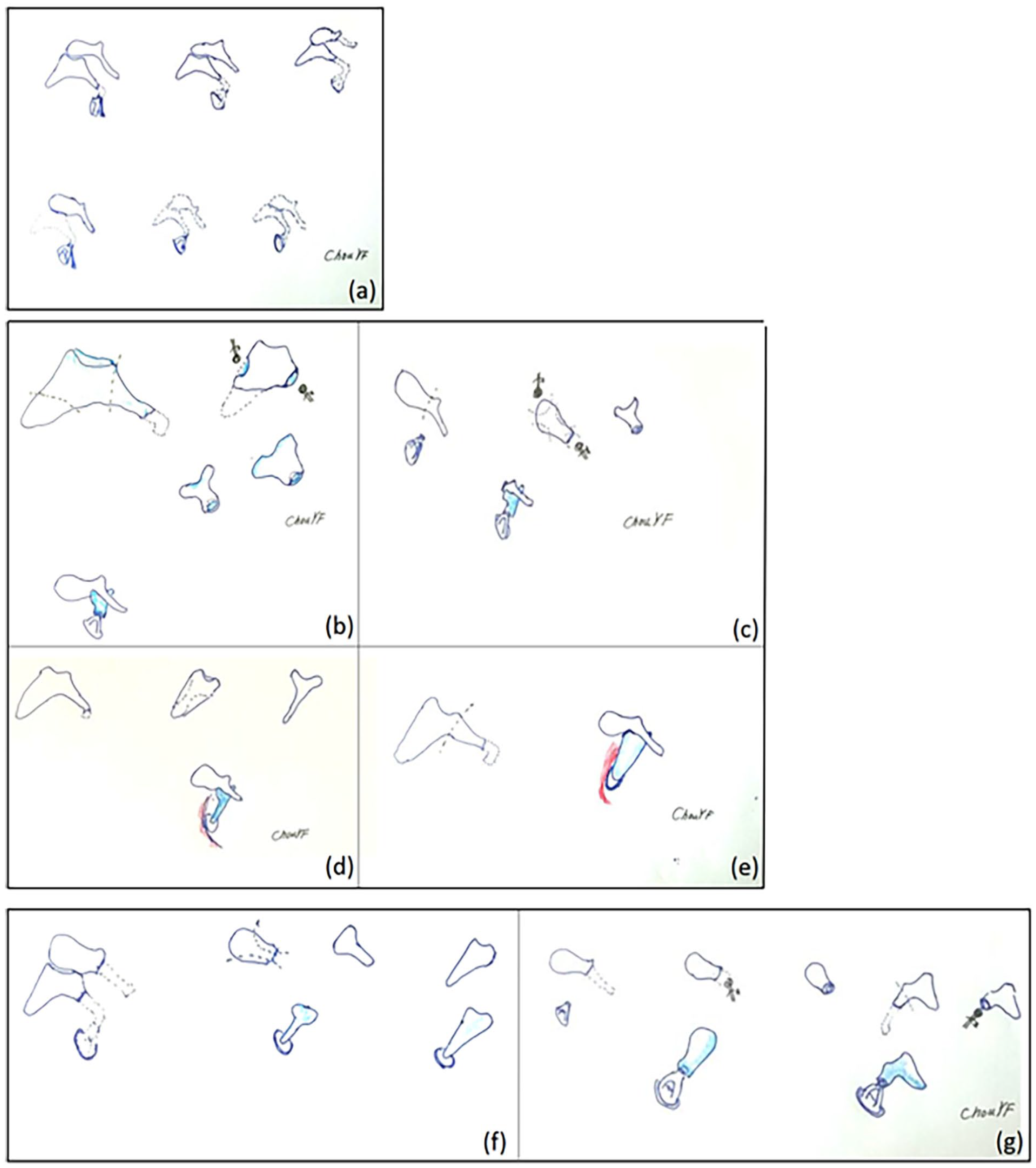
(a) Check ossicular defect. (b) Interposition with incus on stapes. (c) Interposition with malleus head. (d) Interposition with incus on the footplate. (e) Interposition with incus. (f) Columella on footplate. (g) Columella with malleus head or incus.
Statistical Analysis
Descriptive statistics of continuous variables were presented as mean ± standard deviation. Categorical variables were expressed using counts and proportions. The 2 sample t-test was used to compare the continuous variables between middle ear conditions (ie, compromised and uncompromised). Chi-squared tests were used to compare categorical variables.
Multiple linear regression was used to examine the difference between the preoperative and postoperative ABG and other variables, such as different reconstruction methods and tympanoplasty types (type III minor columella versus type III major columella and type Vb tympanoplasty).
Multiple logistic regression was used to examine the association between the successful ABG closure or not (ABG > 25 vs ABG ≤ 25 dB) and other relevant variables. All the analyses were done by SAS (version 9.4; SAS Institute, Cary, NC, USA).
Results
Of the 79 patients included, 36 were men and 43 were women. Their mean age was 45 (range 6-80) years. Group A included 49 ears (adhesion: 6, cholesterol granuloma: 2, and cholesteatoma: 40) and Group B included 31 ears. Three ears (1 from Group A and 2 from Group B) with bone conduction thresholds >70 dB were excluded from the study. All grades of eardrum perforation cases were higher in Group B than in Group A. The tympanic membrane healing rate at 3 months postoperatively was 100%. Type III minor columella tympanoplasty was performed in 54 ears, type III major columella tympanoplasty in 15 ears, and type Vb tympanoplasty in 8 ears. Interposition reconstruction was performed in 64 ears and columella reconstruction in 13 ears. Excluding the missing data, the preoperative threshold of air conduction (TAC) in Group A was 60.8 ± 19.0 dB, and the ABG was 35.3 ± 13.6 dB. In Group B, the preoperative TAC was 62.8 ± 23.8 dB, and the ABG was 33.1 ± 12.9 dB (Table 1). The overall success rate of surgery (ABG < 25 dB) was 54%. No extrusion occurred in any case.
Patient Characteristics.
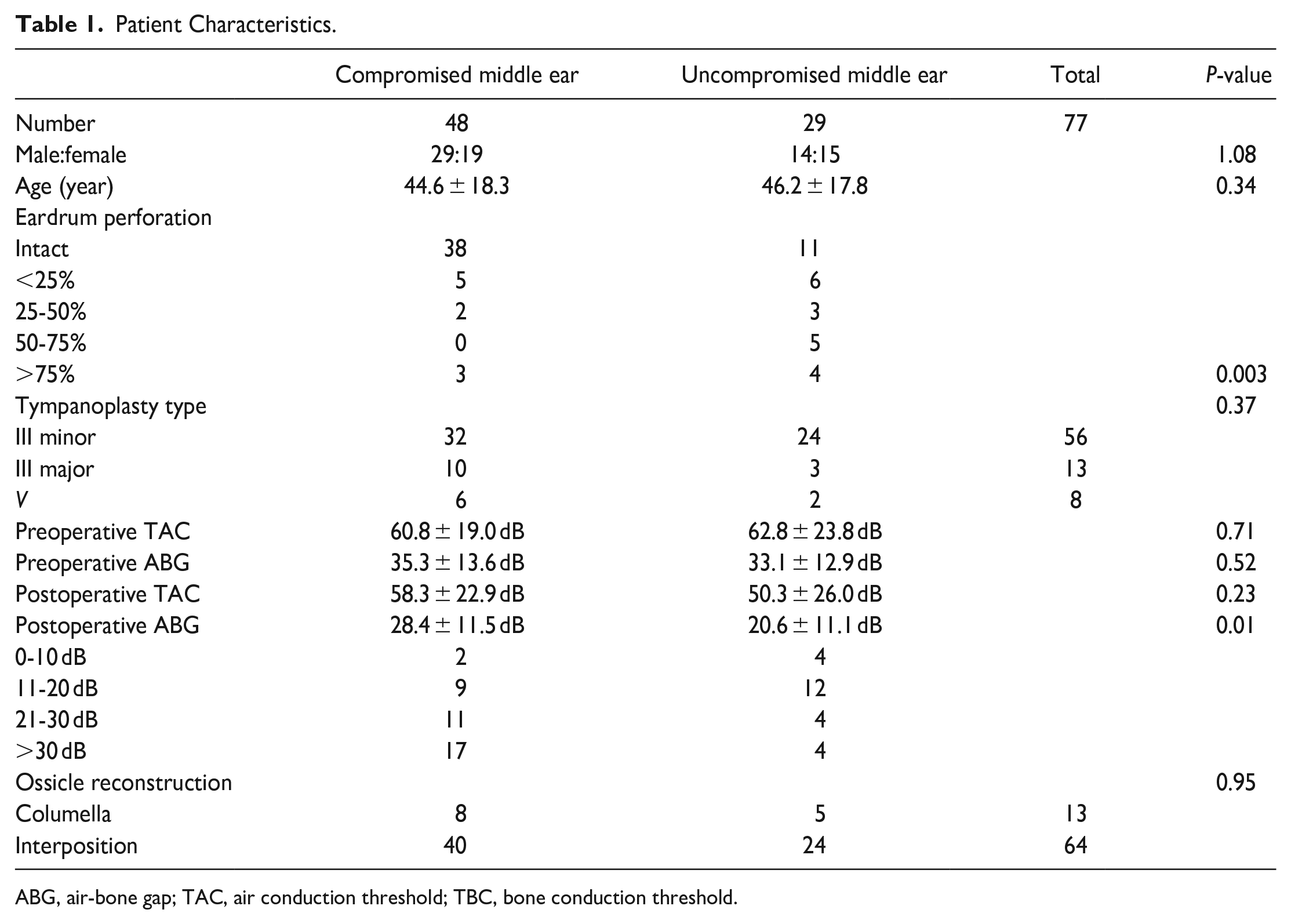
ABG, air-bone gap; TAC, air conduction threshold; TBC, bone conduction threshold.
Multiple linear regression analysis indicated that the postoperative ABG in Group B was significantly better than that in Group A [β = 7.31, 95% confidence interval (CI) = 1.93-12.69, P < .05). Furthermore, the postoperative ABG was significantly better among patients who underwent type III minor columella tympanoplasty than among those who underwent type III major columella plus Vb tympanoplasty (β = 11.42, 95% CI = 5.16-17.68, P < .01). There were no significant differences between the 2 methods of reconstruction (interposition and columella) (Table 2). The results of the logistic regression analysis showed that an uncompromised middle ear and type III minor columella tympanoplasty were significantly related to a successful surgery (Table 3). Multiple linear regression analysis also indicated that the postoperative improvement of TAC in Group B was significantly better than that in Group A (β = −13.56, 95% CI = −24.20 to −2.92, P < .05). However, the difference between preoperative and postoperative ABG values was not significant between Groups A and B, the different types of tympanoplasty, or the type of reconstruction (Table 2).
Association Between Middle Ear Condition, Tympanoplasty Types, Ossicle Reconstruction, and Difference Between Postoperative ABG, the Difference Between Preoperative and Postoperative ABG and TAC.
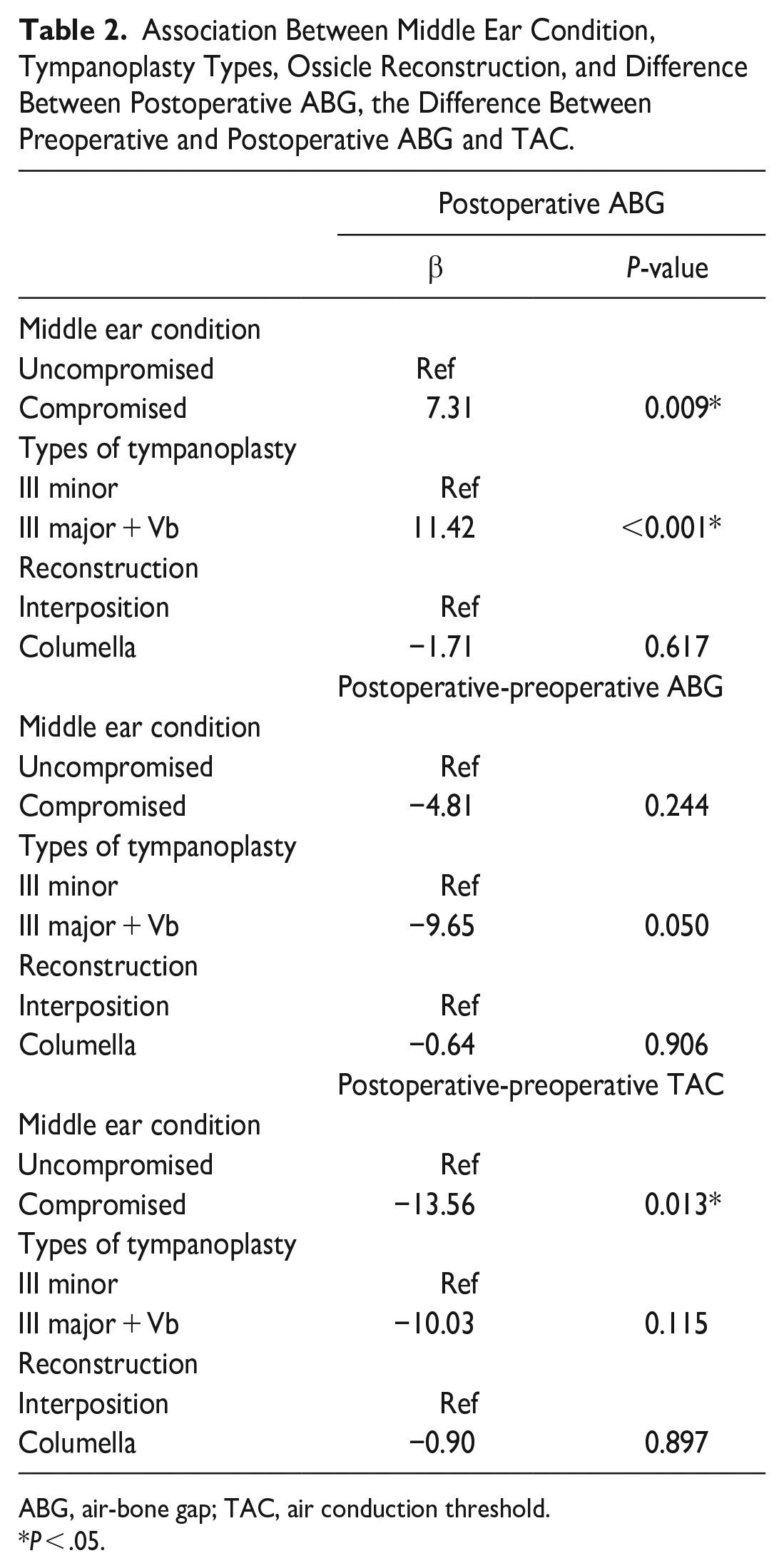
ABG, air-bone gap; TAC, air conduction threshold.
P < .05.
Association Between ABG Closure and Middle Ear Condition, Type of Tympanoplasty, and Ossicle Reconstruction.
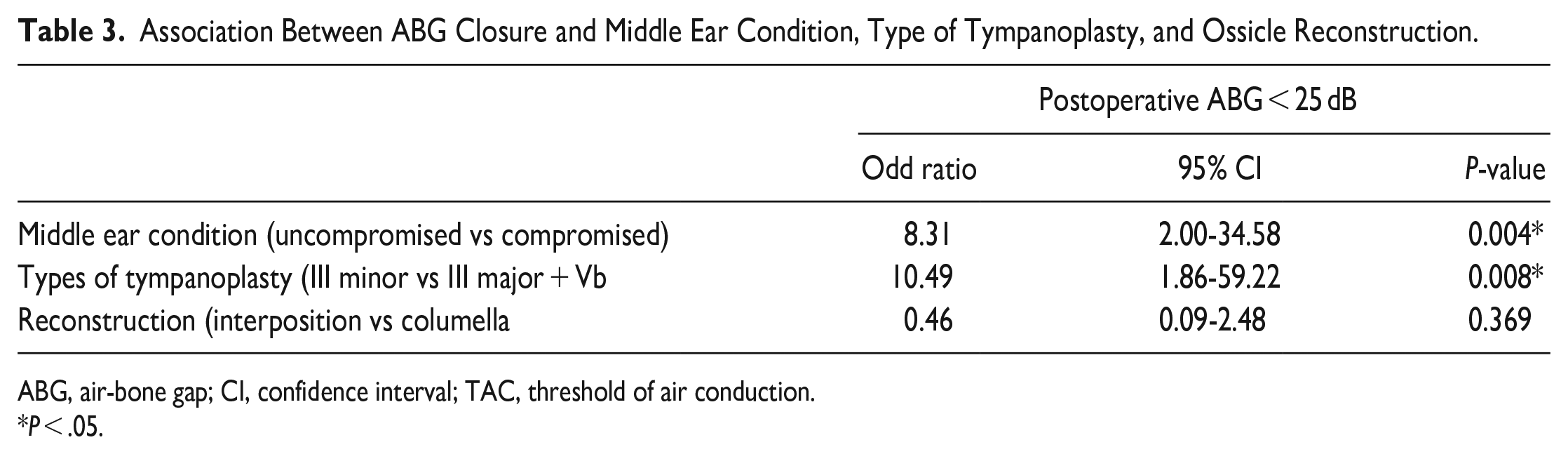
ABG, air-bone gap; CI, confidence interval; TAC, threshold of air conduction.
P < .05.
Discussion
In this study, autografts were used for all cases. A systematic review has shown that there is no difference in decibels gained between autografts and partial ossicular replacement prostheses (PORPs) but a better closure rate was observed with a PORP. 7 The advantages of autografts are that they are cost-effective, have a low extrusion rate, and pose no risk of disease transmission. In our study, the extrusion rate was 0. The disadvantages include a small ossicular remnant, long operation time, and the possibility of residual disease. 8
Our results indicated that the middle ear environment and the presence of an intact suprastructure of the stapes are the most important prognostic factors for a successful ossiculoplasty. No significant difference was observed between the interposition and columella methods of reconstruction. The possible hypothesis is the breaking of acoustic transformer theory. Acoustic transformer theory includes the catenary lever effect, malleoincudal lever effect, and hydraulic lever effect. First, when the patient had COM, the catenary lever effect between the malleus and tympanic membrane will be weak due to the fibrosis or thickening of the tympanic membrane. Second, the malleoincudal lever effect will disappear because the incus is broken. Finally, the sound energy should be transferred to stapes to maintain the hydraulic lever effect. Therefore, the suprastructure is the most important and the malleus may be not necessary for ossicle reconstruction. These results are compatible with those of previous studies.7-9 In our study, 83% of the patients in Group B had a postoperative ABG ≤ 25 dB, similar to that reported in the literature.5,9,10 In a prospective study of 80 cases of ossiculoplasty, Chavan et al. 9 reported an overall success rate of 80%, with success defined as a postoperative ABG < 25 dB; they concluded that autologous incus was the most useful graft material as they observed success rates of 85.28% for autologous incus, 79.16% for PORP, and 75.86% for total ossicular replacement prosthesis. They also concluded that the success rates in cases with diseased middle ear mucosa and cholesteatoma were lower than those in cases without these conditions; however, the difference was not statistically significant. They also reported extrusion in six cases. Choudhary et al., 10 who defined a postoperative ABG of >20 dB as a failed case, reported a success rate of 64.29% for the autologous incus group and 31.81% for the Teflon PORP group. The extrusion rates of PORP and autologous incus were 18.18 and 7.14%, respectively. Kotzias et al. 5 defined success as an ABG of ≤20 dB and reported an overall success rate of 61% in their study. They used the Middle Ear Risk Index (MERI) to define the middle ear status. A high MERI was related to the lowest success rate (36.4%). They also concluded that the presence of the stapes suprastructure was the most important factor contributing to the success rate (85.7%). These results are compatible with those of our study. In our study, the success rates of type III minor columella tympanoplasty (with stapes suprastructure) were significantly better than those of type III major columella and Vb tympanoplasty (without stapes suprastructure). These results imply that the stapes suprastructure is the important factor that influences the hearing result. Evaluating the stapes suprastructure on preoperative temporal CT can predict hearing improvement after ossiculoplasty. In addition, there was no significant difference between the interposition and columella reconstruction methods, which implies that the malleus may not be needed for ossicle reconstruction. TazkNn et al. 3 reported 192 cases of ossiculoplasty performed using the canal wall-down procedure. The mean postoperative ABG was 21.16 dB. Our results were mildly poor compared to this study in which the middle ear condition was relatively poor.
The limitations of our study were that it was a retrospective study and some cases were lost to follow-up. Further prospective studies or meta-analyses are required to confirm the results of our study.
Conclusion
Our results indicate that complex cases compromised by adhesions, cholesteatoma, and cholesterol granuloma have worse outcomes regarding hearing improvement and success rates, while those with intact stapes suprastructure have better outcomes. These findings are consistent with those of previous studies. The malleus may not be needed for ossicle reconstruction.
Footnotes
Acknowledgements
We would like to thank Dr. Ling Yi Wang and Wei Chuan Change of the Epidemiology and Biostatistics Consulting Center at the Buddhist Tzu Chi General Hospital for their help and support for the statistical analysis.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.