
Abstract
Head and neck trauma-induced pulsatile tinnitus (PT) should be approached with caution, as it can rarely be attributed to an arteriovenous fistula (AVF). We present a 26-year-old male with a history of blunt trauma who presented delayed PT with direct AVF between the ascending pharyngeal artery (APA) and the internal jugular vein (IJV). The patient underwent occlusion of the fistula with transarterial embolization using coils and PT was completely resolved, confirming successful treatment. The delayed manifestation of PT in the APA-IJV fistula is probably due to the gradual formation of a pseudoaneurysm and subsequent AVF. This case highlights the importance of investigating PT in head trauma patients, as it can be a sign of AVF and possible complications. Overall, this case contributes to understanding delayed PT with AVF and emphasizes the importance of prompt diagnosis and treatment of AVF in patients with head and neck trauma.
Introduction
Pulsatile tinnitus (PT) may manifest as a symptom several weeks to months after head and neck trauma. Head and neck trauma-induced PT should be approached cautiously, as it can rarely be attributed to an arteriovenous fistula (AVF). AVFs in the head and neck region are typically caused by vascular damage to blood vessels that supply blood to the brain or extradural aneurysms around the venous plexus. Traumatic carotid-jugular fistulas are rare, with an incidence of 4% to 7% of all traumatic AVFs. 1 Direct AVFs between the ascending pharyngeal artery (APA) and the internal jugular vein (IJV) are extremely rare, with only one case reported to have occurred following trauma. 2 If not treated properly, traumatic AVF may progress to high-output cardiac failure, atrial fibrillation, and embolization. 1 In this article, we report a case of successful treatment of PT caused by a direct AVF between the APA and IJV that occurred after trauma. We also performed a literature review of all reported cases of direct AVF between APA and IJV.
Case Presentation
A 26-year-old male with no pre-existing medical conditions sustained a right occipital region injury after a fall while inline skating on the road. He presented to the emergency room with a persistent headache after trauma. Diagnostic imaging revealed no brain hemorrhage and fracture. He received conservative inpatient treatment at the Department of Neurosurgery. Following conservative management, the patient experienced complete resolution of all symptoms, including headache and pain in the affected area, within 4 days. Subsequently, the patient was discharged.
Two months after the trauma, the patient visited our otolaryngology clinic. The patient had persistent PT in the right ear without any other symptoms. He reported that PT began 2 weeks after head trauma. Otoscopic examination revealed an intact tympanic membrane and an external auditory canal. The patient showed normal hearing in pure tone audiometry. The patient localized the tinnitus to the right ear, describing a pulsatile pattern of 20 dB sound pressure level (SPL) narrowband noise at 2000 Hz. Auscultation of the mastoid area with a stethoscope confirmed the objective PT that coincided with the patient’s radial pulse. A digital pressure test on the IJV ipsilateral resulted in no change of PT. The patients described an increase of PT by the water occlusion test. To further validate the presence of the PT, a bidirectional Doppler (BiDop 3) with a handheld, 8 MHz probe (Koven Technology) was used to assess the mastoid area. The detected pulsatile sound was found to match the subjective tinnitus reported by the patient (Figure 1A). Consequently, additional imaging tests including enhanced temporal bone computed tomography (CT; Figure 1C), CT angiography, head and neck magnetic resonance imaging (MRI), and MRI angiography (Figure 1E) were conducted to differentiate tinnitus caused by vascular factors.
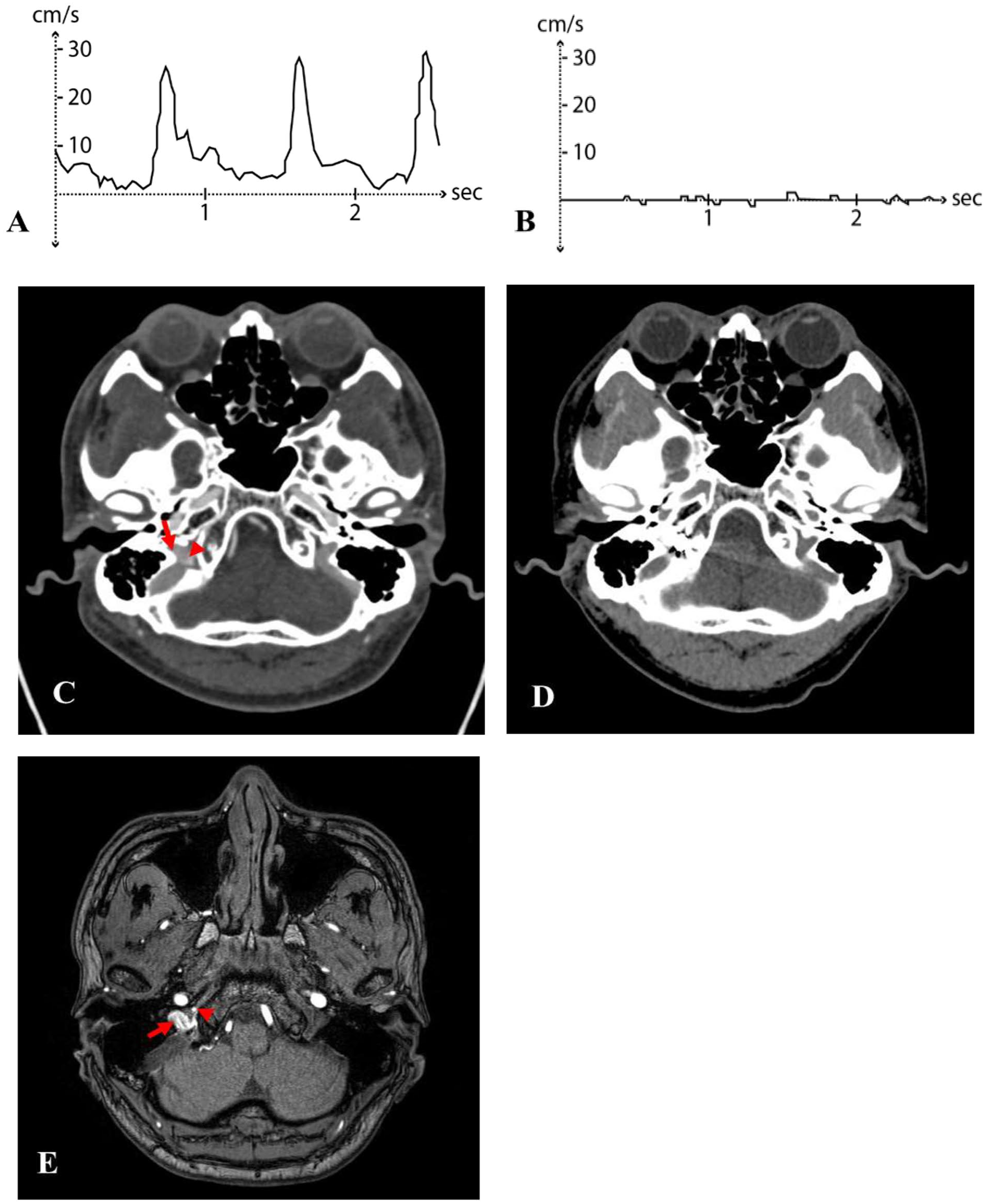
Examination with a handheld Doppler, enhanced temporal bone CT, and MR angiogram. (A) Pre-procedure examination and (B) coil embolization post-procedure examination. (C) Pre-procedure CT taken 3 months after the trauma. Internal jugular vein (arrow) and ascending pharyngeal artery (arrowhead) form a fistula. (D) Post-procedure coil embolization CT. (E) TOF of the MR angiogram. The right internal jugular vein (arrow), which is expected to exhibit a low signal, shows a high signal. This suggests that arterial flow crosses over from the ascending pharyngeal artery (arrowhead), indicating the presence of an arteriovenous fistula. CT, computed tomography; TOF, time of flight; MR, magnetic resonance.
In imaging tests, a suspected AVF was observed between the right APA and the IJV (Figure 1C and E). To further evaluate the AVF, digital subtraction angiography was performed. There was an AVF of high flow that drains from the right APA into the right IJV (Figure 2A). The patient was scheduled for transarterial embolization at the neurosurgery department, and the single hole fistula point was successfully occluded using the Optima™ 3D coils (BALT; Figure 2B and C). Following the procedure, the right PT resolved, confirming successful treatment (Figure 1B and D).
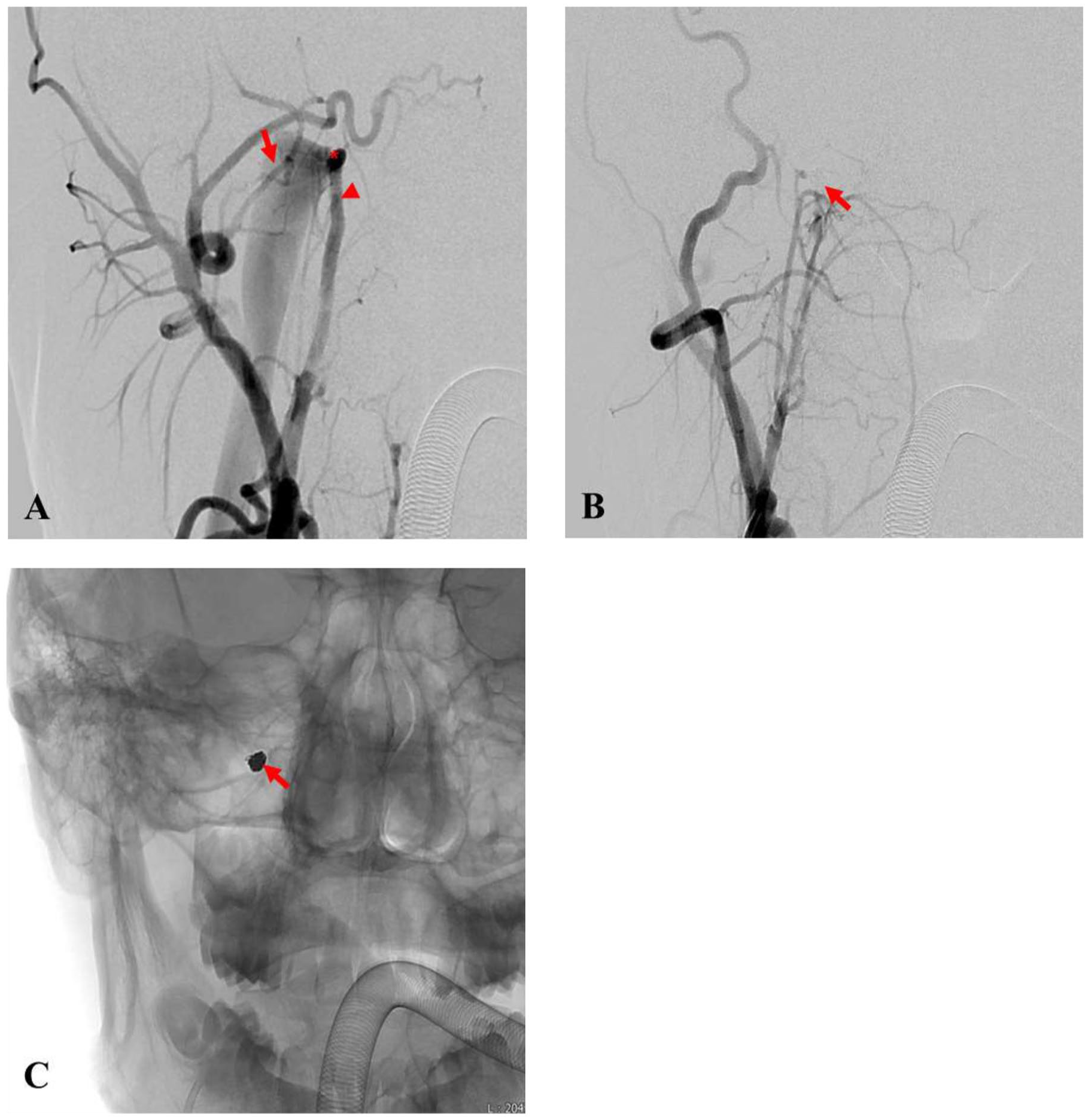
Transfemoral selective angiogram. (A) Pre-embolization diagnostic angiogram. Internal jugular vein (arrow), ascending pharyngeal artery (arrowhead), and direct arteriovenous fistula (asterisk). (B and C) After transarterial embolization (arrow).
The Tinnitus Handicap Inventory (THI) was administered to the patient, and before the procedure, the score was 40 out of 100, corresponding to Grade 3, indicating moderate tinnitus-related impairment.3,4 After the intervention, the patient’s THI score dropped to 0 points, which confirmed the disappearance of tinnitus. As an assessment of depression related to tinnitus, the Patient Health Questionnaire-9 (PHQ-9) was administered to the patient. 5 Before the procedure, the patient scored 7 points on PHQ-9, which improved to 0 points afterward, indicating a significant improvement.
Discussion
PT occurs in less than 10% of all patients with tinnitus, and tinnitus that can be heard objectively by a physician is called objective PT. The source of PT lies within the blood vessels of the cranial cavity, the head and neck area, and the thoracic cavity. It can be heard as a local turbulence when there is a change in blood flow, or normal flow sound can be heard louder due to increased bone conduction in the inner ear or masking of external sound for some reason.6,7 PT is categorized into arterial, arteriovenous, and venous pulsatile, depending on the source of the sound. One of the causes of arteriovenous PT is AVF in the head and neck area, which is very rare. AVFs in the head and neck area occur mainly as a result of damage to the blood vessels supplying the brain or damage to extradural aneurysms around the venous plexus. These AVFs are clinically important because the occurrence of venous outflow from an AVF can lead to a phenomenon of vascular steal, which has the potential to cause additional brain damage. 6 As a result, adequate blood supply to the brain tissue may be compromised, potentially leading to neurological complications such as stroke. In addition, it can alter the direction and pressure of blood flow, increasing the risk of thrombosis formation or hemorrhage.
Furthermore, even if direct AVF does not cause additional complications, the treatment of tinnitus is essential due to its association with an increased incidence of depression, anxiety, and somatic symptom disorders. 8 In this case, the Korean version of the PHQ-9, a screening test for depression, was conducted before and after the procedure to determine the extent of tinnitus-related depression. The PHQ-9 is a self-report survey in which patients rate 9 items on a scale from 0 to 3. A total score of 6 or higher on PHQ-9 suggests a possible depressive disorder. 5 Before the procedure, the patient in this case had a PHQ-9 score of 7, indicating a depressive disorder, which improved to 0 after the procedure. Therefore, the treatment of tinnitus is crucial as it is linked to mental health problems.
Direct AVFs between the APA and the IJV can occur due to their anatomic relationship. The APA is a branch of the external carotid artery. It gives rise to the neuromeningeal trunk, which supplies the meninges through the jugular foramen. Along with the APA, other structures that traverse the jugular foramen include the IJV, glossopharyngeal nerve (cranial nerve IX), vagus nerve (cranial nerve X), and hypoglossal nerve (cranial nerve XII). Consequently, a direct AVF can anatomically occur between the APA and IJV. Traumatic AVFs typically occur as a result of penetrating injuries such as gunshot wounds, stab wounds, or central catheterization, while cases caused by blunt trauma are rare.9,10 In the case of this patient, AVF occurred at the level of the jugular foramen after blunt head trauma. The jugular foramen is bounded anteriorly by the temporal bone and posteriorly by the occipital bone. The impact from the fall likely transmitted through the occipital bone, which could cause damage as it exited through the structures at the jugular foramen. Furthermore, during head movements, excessive strain or flexion of the skull and neck could have led to vascular injury at the bony sites where pressure is exerted significantly. 11 However, direct AVFs between the APA and IJV are extremely rare.
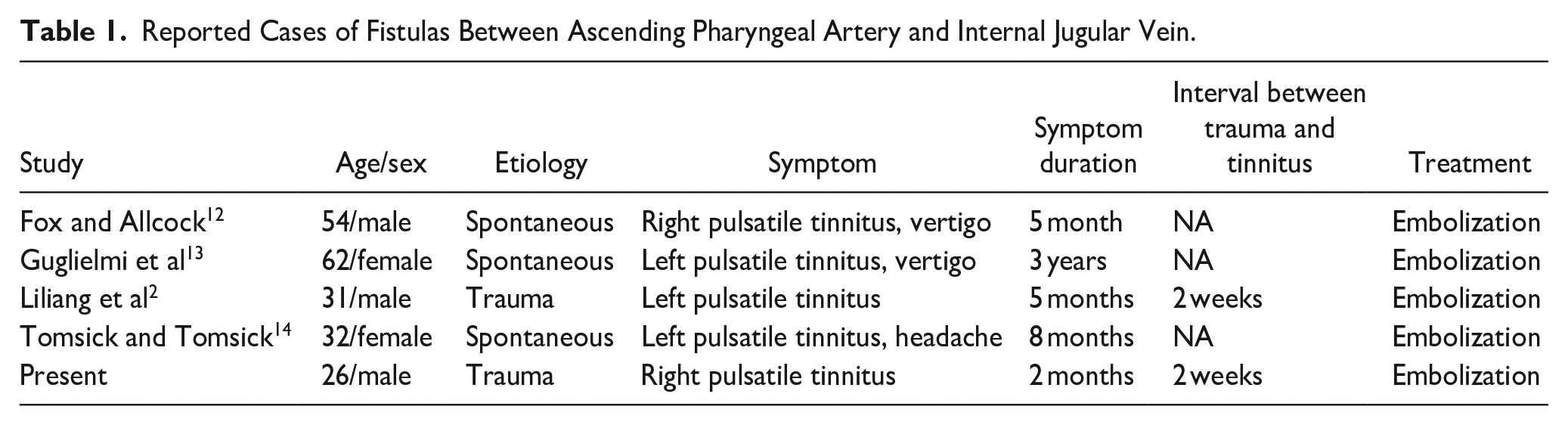
Since Fox and Allcock 12 reported the first case of embolization of spontaneous APA-IJV fistula in 1978, only 5 cases including this case have been reported to date. All reports on AVF between AVF and IJV have been summarized in Table 1.2,12-14 All cases presented PT as a clinical symptom. Among these cases, 2 cases including this case were reported to occur after trauma. The time interval between head trauma and the onset of PT was 2 weeks. The delayed manifestation of PT in the APA-IJV fistula after trauma is attributed to the underlying pathophysiology of fistula formation. When the arterial wall is injured, arterial bleeding occurs within the surrounding soft tissue. A pseudocapsule, composed of fibrin and platelets, develops, limiting the ongoing bleeding into surrounding tissues. The absence of layers of arterial wall in this pseudocapsule, rendering it structurally weaker than a true aneurysm, defines it as a pseudoaneurysm. 15 Concurrent injury to an adjacent vein can lead to the extension of the pseudocapsule between the artery and the vein, leading to the formation of AVF. 16 The delayed onset of PT, typically occurring approximately 2 weeks after trauma, may be attributed to the gradual formation of direct AVFs between APA and IJV.
Reported Cases of Fistulas Between Ascending Pharyngeal Artery and Internal Jugular Vein.
The presence of PT can be crucial in the evaluation of head trauma patients as it can help clinicians differentiate the presence of AVF which can lead to serious complications. Therefore, a thorough imaging evaluation should be conducted among patients experiencing PT to promptly detect and treat direct AVF, thereby preventing any potential secondary complications. Even in patients who are unable to communicate their symptoms due to altered consciousness, objective tinnitus can be detected through simple such as mastoid auscultation or Doppler ultrasound. On reporting this symptom, we performed auscultation and Doppler ultrasound, confirming the presence of objective tinnitus. If objective PT is identified in a patient with head trauma, a comprehensive imaging evaluation should be conducted to differentiate the presence of AVF. Consequently, a prompt imaging evaluation was initiated, which swiftly identified a direct AVF in this case. AVF was effectively treated through intervention, leading to immediate alleviation of patient’s symptoms.
Conclusion
Head and neck trauma-induced PT should be approached with causion, as it can rarely be attributed to an AVF. The delayed manifestation of PT in the APA-IJV fistula is likely due to the gradual formation of a pseudoaneurysm and subsequent AVF. This case highlights the importance of investigating PT in patients with head and neck trauma as it can be a sign of AVF and potential complications. Overall, this report contributes to understanding rare cases of PT and emphasizes the importance of prompt diagnosis and treatment of AVF in head and neck trauma patients.
Footnotes
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a 2020 Research Grant from Kangwon National University; and a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2017R1C1B5076065). The funders had no role in the study design, data collection or analysis, decision to publish, or manuscript preparation.
Ethical Approval
The study protocol was approved by the Institutional Review Board of National University Hospital (IRB 2023-07-004). Written informed consent was obtained from the patient for their anonymized information to be published in this article.