
Abstract
This report describes the unique case of a 37-year-old pregnant patient with a history of total thyroidectomy who presented worsening dyspnea due to a recurrent benign goiter. The goiter grew through the tracheal wall and narrowed the tracheal lumen. After unsuccessful treatment with bronchodilators and corticosteroids, the patient underwent an emergency tracheostomy and cesarean section. Cervicothoracic computed tomography revealed a 4 cm mass in the left lobe of the thyroid gland with endotracheal extension in the subglottic region. Exploratory cervicectomy revealed a macroscopically resected mass that resembles the structure of the thyroid, adherent to the esophagus, anterior to the cricoid cartilage, and the trachea. Intratracheal thyroid tissue was not excised due to the increased risk of bleeding, and endoscopically guided biopsies were performed. Histopathological examination confirmed the benign nature of the thyroid tissue. A follow-up computed tomography scan after 2 months showed spontaneous regression of the intratracheal mass, and the tracheostomy tube was successfully removed without complications.
Key Clinical Message
A rare case of a pregnant patient with a history of total thyroidectomy, presented with dyspnea due to the recurrence of a benign goiter extending into the trachea. This combination of goiter recurrence during pregnancy, intratracheal growth, and subsequent spontaneous regression during the postpartum period has not been previously reported.
Introduction
Compressive goiters and locally advanced aggressive thyroid carcinomas are the 2 main causes of upper airway obstruction. 1 While benign goiters are often asymptomatic, their growth can lead to esthetic discomfort and compressive symptoms. Upper airway obstruction is rare unless the benign goiter is significantly large or extends into the intrathoracic region, especially in cases of retrosternal localization. 2 This obstruction is typically caused by external compression rather than intratracheal growth of thyroid tissue. 3 The reported cases of benign intratracheal thyroid in the literature involve mainly intratracheal thyroid ectopia and very rare cases of intratracheal extension of a benign goiter. 3 Among these cases, there have been only 2 documented occurrences during pregnancy.4,5 Here, we present an exceptional case of a young woman with a history of thyroid surgery who experienced progressively worsening dyspnea during her pregnancy, caused by the recurrence of a benign thyroid goiter with intratracheal extension.
Case Report
A 37-year-old patient, in her first pregnancy and at 34 weeks of gestation, presented to the emergency department with dyspnea that had been present for 6 months. The patient had a history of thyroid surgery for a benign goiter, performed twice, with a lobectomy at the age of 6 years, completed by a total thyroidectomy at the age of 10 years. The patient also had hypothyroidism and was on levothyroxine therapy at a dose of 150 and 175 μg/day on alternate days. Dyspnea has worsened over the past week. Initially thought to be a severe asthma attack, dyspnea did not respond to bronchodilators and corticosteroids. As signs of respiratory distress appeared, the patient underwent an emergency tracheotomy under local anesthesia. Concurrently, a cesarean section was performed.
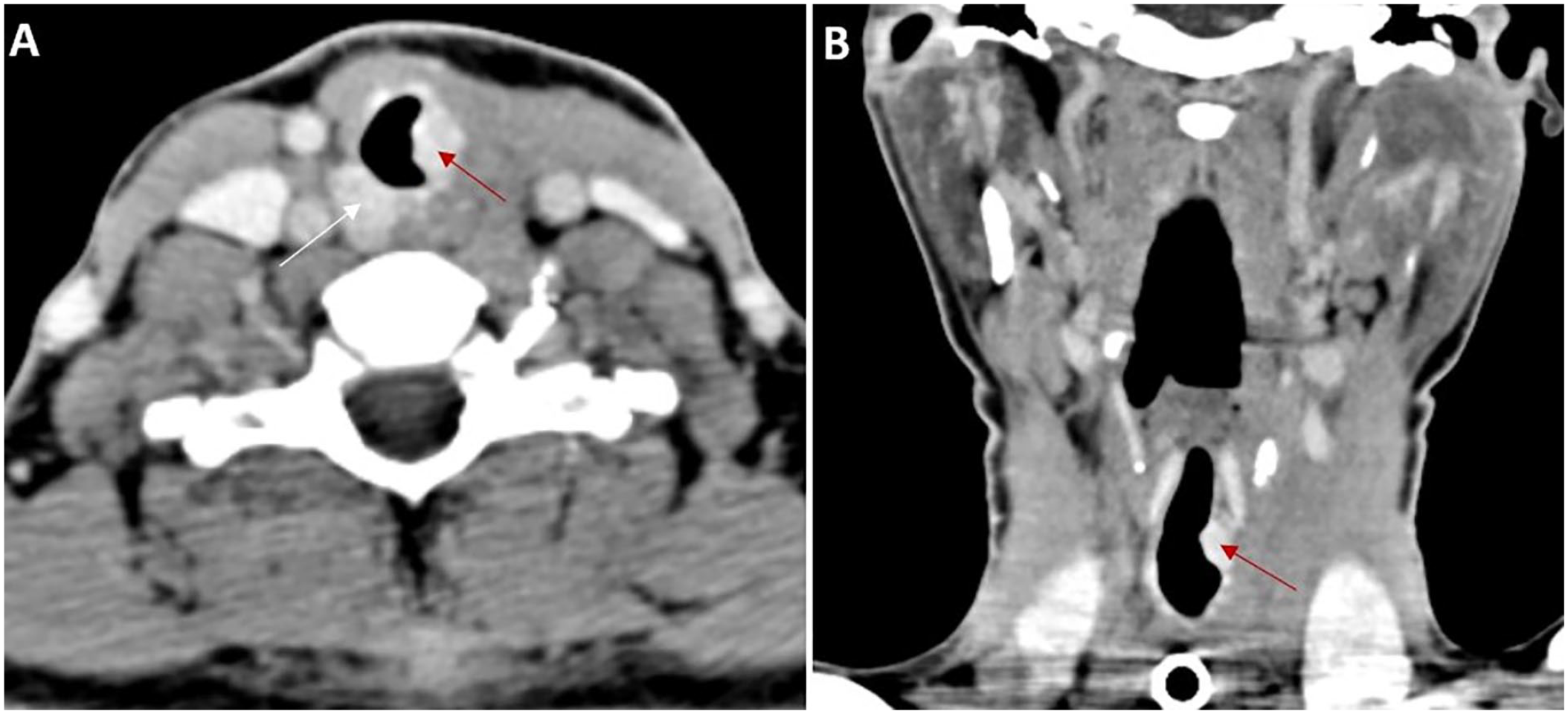
A cervicothoracic computed tomography (CT) scan revealed a tissue mass in the left lobe of the thyroid, measuring 4 cm in its largest dimension, causing posterior displacement of the esophagus and intratracheal extension into the subglottic region, resulting in near-total obstruction of the tracheal lumen (Figure 1).

Cervical CT scan with contrast, axial (A) and coronal (B) views: A tissue mass located in the left thyroid lobe (blue arrow) measuring 40 mm × 38 mm × 26 mm and extending between the trachea and esophagus causing posterior displacement of the esophagus. Intratracheal extension into the subglottic region, resulting in a significant narrowing of the tracheal lumen.
The thyroid parameters revealed hypothyroidism, with a level of thyrotropin-stimulating hormone (TSH) of 20.2 mU/L (normal range: 0.27-4.2), and a level of free thyroxine (T4) of 11.3 pmol/L (normal range: 7.0-14.0).
A bronchial nasofibroscopy demonstrated a subglottic tissue mass extending over 2 cm, characterized by a highly inflamed hypervascular mucosa with complete tracheal obstruction. The vocal cords were symmetric and mobile. No biopsy of the mass was performed due to the risk of hemorrhage.
The patient underwent direct laryngoscopy and exploratory cervicotomy, which revealed a mass in the left thyroid compartment that was adherent to the esophagus, the cricoid cartilage, and the trachea. This mass had a macroscopic extension into the trachea through the cricotracheal membrane. Shaving of the esophagus, as well as the first tracheal ring and cricoid cartilage, was performed, and the mass was excised. The intraoperative frozen section examination confirmed the presence of benign thyroid tissue with no signs of malignancy. Due to the increased risk of bleeding, intratracheal thyroid tissue was not resected and only endoscopic biopsies were taken.
After surgery, the patient had left vocal cord paralysis and was unable to have the tracheostomy tube removed. Histopathological examination showed the presence of thyroid tissue with vesicular architecture with no signs of malignancy. The patient was put back on levothyroxine at a substitutive dose and the follow-up TSH level normalized to 1.71 mU/L 3 weeks after surgery.
An endoscopic laser resection was planned to be performed to remove the intratracheal extension of the mass. However, a control CT scan performed after 2 months showed spontaneous regression of the intratracheal mass, with the presence of 2 subglottic tissue nodules measuring 10 and 15 mm, respectively. One of the nodules had an exophytic endoluminal growth. There was no obstruction in the tracheal passage (Figure 2). Indirect control laryngoscopy revealed persistent paralysis of the left vocal cord with contralateral vocal cord compensation. Therefore, the patient was successfully decannulated and was referred for speech therapy rehabilitation. Given the spontaneous regression of thyroid mass, we have chosen to implement an active surveillance approach to monitor the remaining residue of thyroid tissue.
Cervical CT scan with contrast, axial (A) and coronal (B) views. Significant regression of the intratracheal mass with the presence of 2 subglottic nodules. The first nodule (red arrow) measures 10 mm and is located below the lateralized cricoid cartilage on the left, exhibiting an endoluminal exophytic growth. The second nodule (white arrow) measures 15 mm and is located on the right, in an extraluminal postero-lateral position.
Discussion
The present case illustrates an exceptional clinical situation of a patient with a history of total thyroidectomy who presented progressively worsening dyspnea during her pregnancy, caused by the recurrence of a benign thyroid goiter growing through the tracheal wall. This intratracheal extension was responsible for an upper airway obstruction that resolved spontaneously during the postpartum period.
To our knowledge, this is the first documented case in the literature that encompasses the simultaneous occurrence of a pregnancy-related benign goiter recurrence and intratracheal extension.
The 2 cases reported in the literature of recurrent benign goiter after total thyroidectomy with intratracheal growth were unrelated to pregnancy.6,7
Goiter recurrence is not uncommon after thyroidectomy and accounts for up to 12% of all thyroid surgeries. 8 The causes of recurrent benign goiter are primarily attributed to inadequate surgical techniques, as well as inadvertent retention of embryological remnants. 9 Subtotal thyroidectomy is the main cause of recurrence, with recurrence rates ranging up to 40%. 10 Recent reviews have shown a risk of recurrence even after total thyroidectomy. 11 Most recurrences occur in the thyroid bed after subtotal thyroidectomy, while with total thyroidectomy, they often occur in the pyramidal or thyrothymic tract. 12 The persistence of embryonic remnants from thyroid development is responsible for the recurrence of ectopic goiter. The pyramidal tract can lead to goiters between the base of the tongue and the thyroid bed. 13 In the trachea, remnants can cause intratracheal goiters. 7
Several biological factors have been associated with thyroid tissue growth and recurrence of goiter, including TSH, human chorionic gonadotropin (HCG), and local growth factors such as transforming growth factor β1.9,14 Thyroxine administration after total thyroidectomy aims to prevent hypothyroidism and reduce the risk of recurrence. However, the theoretical basis for thyroxine administration assumes TSH’s primary role in the regrowth of thyroid tissue. 9 For our patient, we believe that pregnancy and hypothyroidism with elevated TSH levels were potential risk factors associated with goiter recurrence.
The goitrogenic effect of pregnancy on thyroid physiology has been well established. 15 This effect is attributed to the combined influence of several factors during pregnancy, including increased maternal weight, iodine deficiency resulting from transplacental passage, elevated renal clearance of iodine, and elevated levels of HCG. 16 HCG has TSH-like activity due to a common α-subunit and homology between their β-subunits and binds to the TSH receptor. 16 Eggo 17 identifies other growth factors, such as estrogen, insulin-like growth factors, angiopoietins, vascular endothelial growth factors, and growth factor receptors, that can potentially contribute to increased thyroid size during pregnancy.
A unique aspect of our case report is the presence of intratracheal extension of the recurrent goiter, which grew significantly during pregnancy. Only 2 cases of pregnancy-related goiter with intratracheal thyroid growth have been documented. Døssing et al 4 reported a case of pregnancy-associated upper airway obstruction caused by intratracheal ectopic thyroid tissue. Sung et al 5 presented a case of upper airway obstruction during pregnancy resulting from intratracheal extension of adenomatous thyroid hyperplasia. These 2 patients did not have a history of total thyroidectomy, as opposed to our case. In addition, these 2 cases illustrate the 2 suggested hypotheses to elucidate the intratracheal growth of thyroid tissue. One theory, referred to as the “malformation theory,” proposes that improper development of the thyroid gland leads to the separation of an embryonal thyroid fragment, which is sequestered within the trachea. This theory explains cases of intratracheal ectopic thyroid goiter. 18 Another theory, known as the “ingrowth theory,” suggests that intratracheal thyroid tissue is the result of direct invasion of properly formed mature thyroid tissue through tracheal cartilage. This theory is supported by the anatomical connection observed between the intraluminal and extraluminal portions of the gland, as seen in our case. 19
The clinical presentation of a thyroid goiter with intratracheal extension includes respiratory difficulties, cough, stridor, and even dysphagia. 7 Distinguishing this stridor from asthma-related wheezing can be challenging during physical examination. 7 The diagnosis is not always straightforward, but if suspected, it can be established by CT and laryngo-tracheoscopy. 4 In our case, the preoperative diagnosis was thyroid malignancy with tracheal invasion. Another potential diagnosis, such as malignant tracheal tumors, 5 was excluded based on imaging findings, including the absence of tracheal thickening, the presence of an intraluminal mass with an enhancement pattern similar to that of the thyroid gland, and the connection between intratracheal extension and thyroid goiter.
Tracheotomy under local anesthesia is generally necessary to relieve dyspnea. 3 Factors that determine the management approach include the size of the lesion, the age of the patient, the presence of local symptoms, the state of thyroid function, and histological findings. 7 Surgical excision, radioiodine ablation, and thyroid suppressive therapy are the treatment options. 7 Gold standard therapy involves excision of the thyroid goiter and intratracheal mass. Complete excision is imperative in the cases of histological malignancy. 7 For benign tumors, it is recommended to perform an intratracheal mass along with or without hemithyroidectomy. 3 The 2 commonly used surgical methods for intratracheal thyroid masses are the endoscopic laser-assisted approach and the open cricoid procedure. 7 Radiation ablation with hormonal suppression has only limited success. 20 For our patient, hemithyroidectomy was performed primarily to obtain a histological diagnosis. Resection of the intratracheal mass was not performed due to its benign nature and the increased risk of difficult-to-control bleeding, especially when cold instruments were used for endoscopic procedures. However, an endoscopic laser resection was planned to be performed at a later stage.
A spontaneous regression of intratracheal thyroid mass was observed after a 2-month postpartum period. We speculate that this regression can be attributed to the resolution of hypothyroidism with normalization of TSH levels, but more importantly, to the disappearance of goitrogenic factors related to pregnancy.
Conclusion
In conclusion, we describe a rare case of a pregnant woman with a history of total thyroidectomy presenting with dyspnea due to a recurrent benign goiter extending into the trachea. This is an extremely rare combination of goiter recurrence during pregnancy, intratracheal thyroid growth, and spontaneous regression that occurred during the postpartum period. No other case reports have this combination, as far as we know.
Footnotes
Acknowledgements
All authors approved the final version and have the agreement to be responsible for all aspects of the work in ensuring that questions related to the accuracy.
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases.
Patient Consent
Obtained from the patient in writing.
Grant Number
No financial support was received for the research.