
Abstract
Objective
To examine various factors associated with an increased risk of reoperation for persistent or recurrent malignant thyroid cancers.
Study Design
Retrospective cohort study.
Setting
Tertiary academic hospital centers.
Methods
Patients undergoing surgery for thyroid cancer at 2 tertiary academic institutions from 2006 to 2020 were included. Those who underwent a reoperative procedure were compared with patients only requiring 1 procedure. The Pearson chi-square and independent t test were used to compare group data accordingly. Furthermore, a binomial logistic regression was performed, while machine learning models were used to construct a predictive algorithm.
Results
This study included 2266 patients with surgically managed thyroid malignancy, of which 54 (2.4%) necessitated reoperations. Those requiring a second surgical procedure were more likely to be male (40.7% vs 20.9%, P < .001), undergo bilateral (24.1% vs 3.3%, P < .001) and lateral (16.7% vs 1.8%, P < .001) neck dissections, and have a greater number of metastatic lymph nodes (mean, 9.1 vs 3.5; P < .001) and a larger tumor size (mean, 3.0 vs 2.0 cm; P < .001). According to the binomial logistic regression model, lateral neck dissection, greater number of metastatic lymph nodes, and larger tumor size significantly increased the odds of necessitating a second procedure by 7.8 (95% CI, 2.523-24.083), 1.1 (95% CI, 1.032-1.152), and 1.3 (95% CI, 1.064-1.559), respectively. Last, machine learning models could not significantly predict the occurrence of reoperation.
Conclusion
This study identified patient- and cancer-related characteristics associated with an increased risk of requiring reoperation for thyroid malignancies.
In the last decade, the incidence of thyroid cancers has steadily increased in Canada and other developed countries. 1 While prognosis varies by staging and subtype, thyroid malignancies generally have favorable outcomes with a low cancer-related mortality rate. 2
For patients diagnosed with a differentiated thyroid cancer (eg, papillary and follicular subtypes), surgery is the first-line therapy. 3 In general, initial thyroidectomy is associated with a lower complication rate, such as recurrent laryngeal nerve injury, morbidity from neck dissection, and hypoparathyroidism, when compared with reoperative procedures for persistent or recurrent disease.4-6 In addition to the challenges of operating in scarred tissues and altered anatomy, recurrent thyroid cancers have been shown to be more aggressive. 7 Thus, early detection of recurrent or persistent cancers via diligent, targeted monitoring and screening efforts may help mitigate complications and surgical challenges while allowing for timely diagnosis of aggressive disease, ultimately leading to optimized patient outcomes. Moreover, prompt diagnosis of recurrence could minimize costs to the health care system by limiting the need for challenging reoperative procedures.
The objective of this study was to assess a cohort of patients requiring a second surgical procedure for malignant thyroid disease. This cohort was compared with a group of patients requiring only 1 procedure for malignant disease. Factors that could influence the risk of cancer recurrence or persistence requiring a secondary procedure were explored and compared between the groups including age, sex, metastatic lymph nodes (MLNs), and MLN ratio (MLNR).
Methods
Ethics Approval
This study was reviewed and approved as a multicenter project by the Research Ethics Board at the McGill University Health Center (MP-37-2021-7526) and the Jewish General Hospital (MEO-37-2022-3166) and was conducted in accordance with the Declaration of Helsinki.
Data Collection
A retrospective review was performed of patients requiring surgery for a malignant thyroid condition in 2 tertiary academic centers in Montreal, Canada, from July 2006 to December 2020. All surgical procedures were preceded by ultrasound examination and ultrasound-guided fine-needle aspiration. Final pathology was ascertained on tissues collected at the time of surgery, and diagnosis was confirmed thereafter. Patients with missing information and those with a benign or inconclusive diagnosis were excluded. Patients who underwent a second surgical procedure for recurrent or persistent thyroid malignancy were identified. The revision procedures included partial, hemi-, and subtotal thyroidectomies in addition to a varying extent of neck dissection. For this study, the group of patients requiring a single procedure is referred to as group 1, while group 2 designates those patients requiring reoperative thyroid surgery.
Baseline patient demographics (eg, sex and age) were compared between the groups. Surgical variables of interest were the type of thyroid surgery and the extent of neck dissection. Patients initially undergoing a hemithyroidectomy and later receiving a completion thyroidectomy for classic indications were included in group 1. Thyroid cancer subtypes were examined and divided in 3 categories: papillary, follicular, and other. The papillary histology subtype comprised the following variants: follicular variant, diffuse sclerosing, solid-trabecular, oncocytic, tall cell, cribriform-morular, Warthin-like, hobnail, and columnar. Moreover, patients diagnosed with medullary, anaplastic, poorly differentiated thyroid, or sclerosing mucoepidermoid carcinoma were included in the “other” cancer subtype category. Last, the number of MLNs, MLNR, tumor size, extrathyroidal extension (ETE), and extranodal extension (ENE) were evaluated. The MLNR was calculated by dividing the number of MLNs by the total number of harvested lymph nodes.
Statistical Analysis
The Pearson chi-square test was used to analyze categorical variables, presented as numbers and percentages ( Tables 1 and 2 ). Continuous variables, presented as mean and standard deviation, were analyzed with the 2-sided independent t test. Following the univariate analyses, statistically significant variables between the groups were entered into a binomial logistic regression model to ascertain the independent effect of these variables on the likelihood that patients would require recurrent thyroid surgery ( Table 3 ). For all analyses, a P value <.05 was considered significant. Statistical analyses were performed with SPSS Statistics version 27.0 for MacIntosh (IBM).
Patient, Surgical, and Disease Variables Between the Groups. a
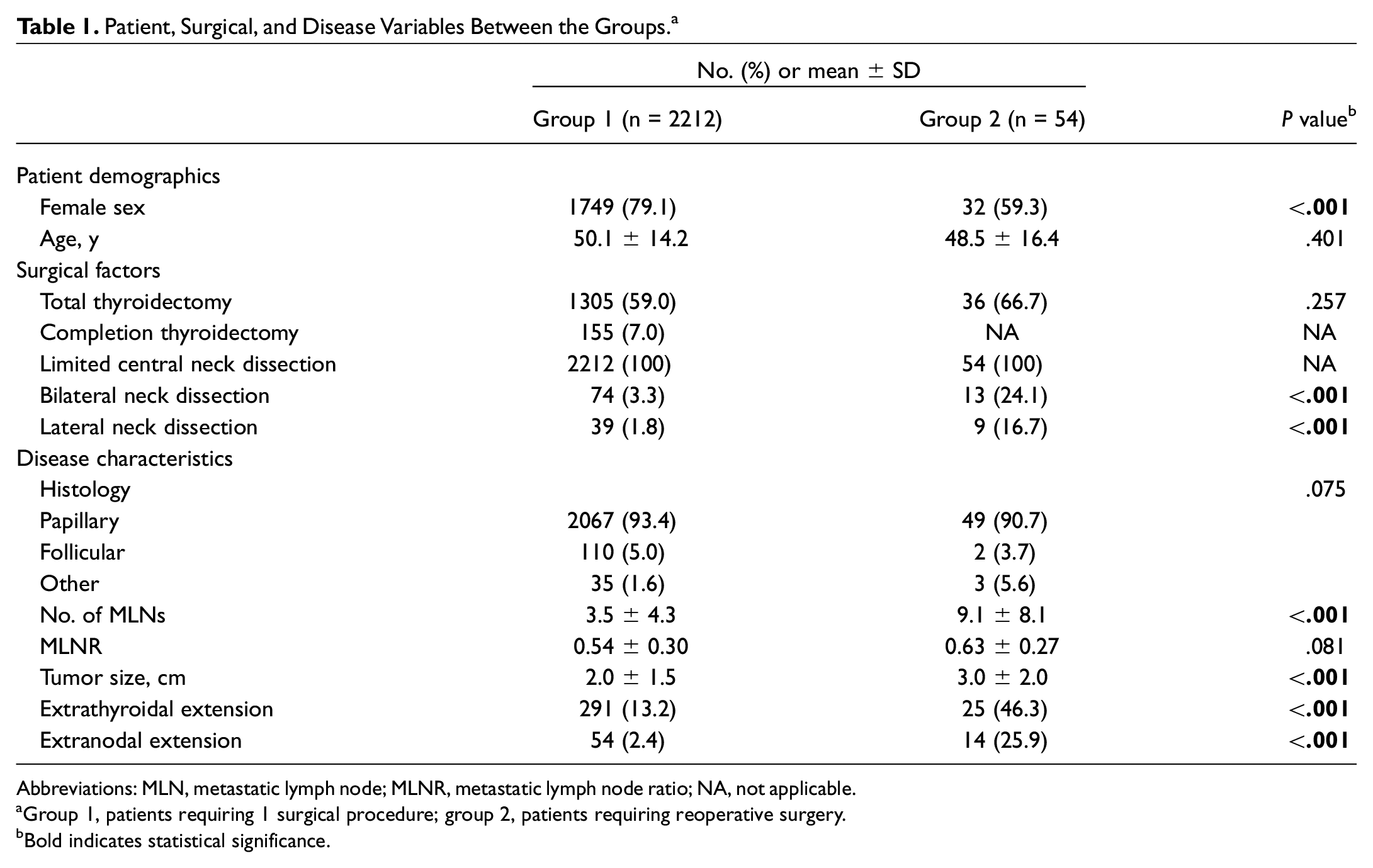
Abbreviations: MLN, metastatic lymph node; MLNR, metastatic lymph node ratio; NA, not applicable.
Group 1, patients requiring 1 surgical procedure; group 2, patients requiring reoperative surgery.
Bold indicates statistical significance.
Patients Requiring a Second Surgical Procedure for a Thyroid Malignancy (54 Patients). a
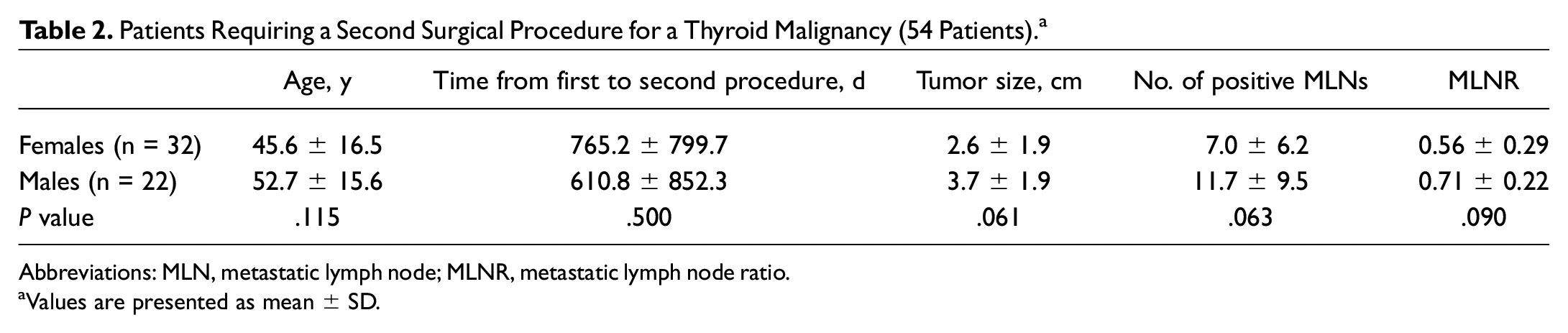
Abbreviations: MLN, metastatic lymph node; MLNR, metastatic lymph node ratio.
Values are presented as mean ± SD.
Binomial Logistic Regression Predicting the Likelihood of Necessitating a Second Procedure for a Thyroid Malignancy. a
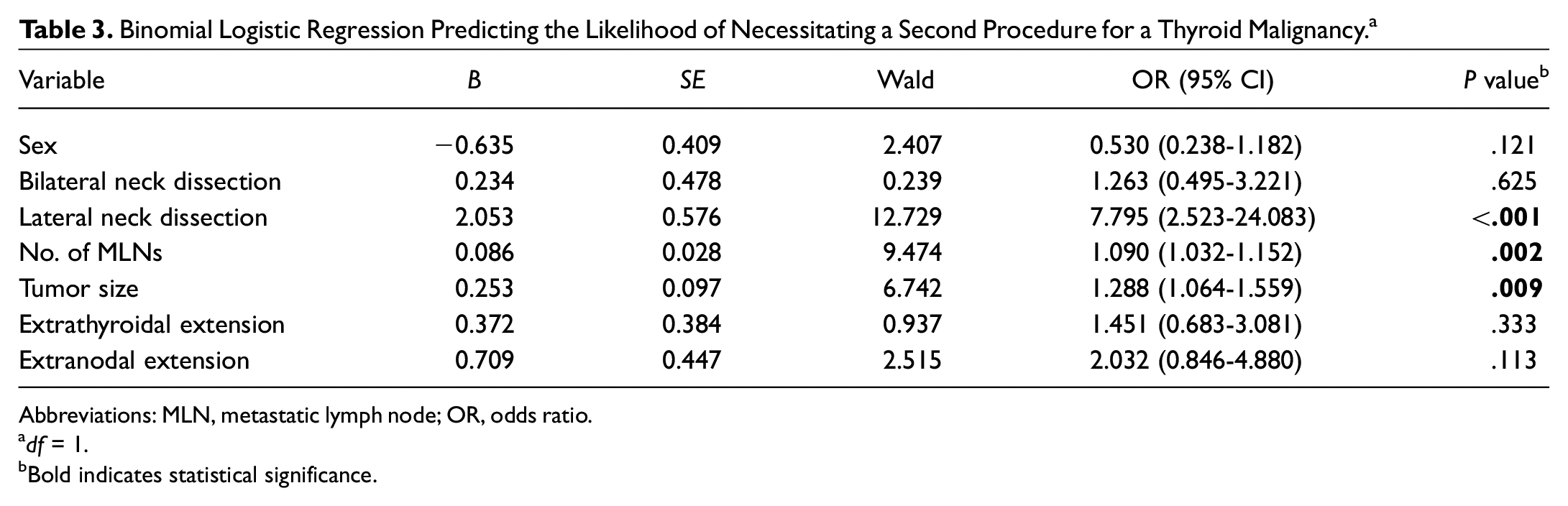
Abbreviations: MLN, metastatic lymph node; OR, odds ratio.
df = 1.
Bold indicates statistical significance.
Machine Learning
A support vector machine classification algorithm was used to classify whether patients belonged to the group requiring reoperative thyroid surgery based on their patient characteristics and surgical and disease factors. The patient data were randomly divided between training and testing data subsets, where the testing subset comprised 30% of the total number of data points. The support vector machine classifier algorithm was developed in MATLAB (version R2020b; MathWorks), and linear, Gaussian, and polynomial kernel functions were used to determine group classification. The model’s performance was evaluated with the model’s loss, which quantifies the model’s misclassification (false negatives and false positives) when applied to the testing data subset. When classification models are compared, a lower calculated loss value is associated with a lower misclassification rate and thus an improved prediction accuracy.
Results
Patient Characteristics
Between July 2006 and December 2020, 2266 patients received surgery for a thyroid malignancy by a single surgeon at the aforementioned institutions. Of those, 54 (2.4%) patients had recurrent or persistent malignant disease requiring reoperation. Comparisons of various patient, surgical, and disease variables between the groups are presented in Table 1 . Although female patients were more prevalent in the single (group 1) and reoperative (group 2) surgery groups, representing 79.1% and 59.3% of patients, respectively, group 2 had a significantly higher proportion of men than group 1 (P < .001). Moreover, although not significant, group 2 had a lower mean age as compared with group 1 (48.5 vs 50.1 years, P = .401).
Surgical Factors
The number of patients who underwent a total thyroidectomy vs a less extensive procedure (eg, hemithyroidectomy) on initial presentation was not significantly different between the groups (59.0% vs 66.7%, P = .257; Table 1 ). Notably, of those in group 1, 155 patients (7.0%) underwent a completion thyroidectomy shortly after the initial procedure. Second, for patients who underwent neck dissection, comparisons between the groups were made regarding the type of dissection employed by the surgeon (unilateral and bilateral). All patients underwent a central neck exploration with a limited central compartment neck dissection. The number of patients in group 2 subject to bilateral (24.1% vs 3.3%, P < .001) and lateral (16.7% vs 1.8%, P < .001) neck dissections was higher. In summary, those requiring a second surgical procedure were more likely to have initially undergone neck dissections beyond the central compartment.
Disease Factors
The histologic classification based on the final pathology report was compared between the groups. Three categories were considered: papillary, follicular/Hurthle cell, and other. Papillary subtype was the most common, representing 93.4% and 90.7% of cases in groups 1 and 2, respectively. Moreover, the mean number of lymph nodes positively identified for malignancy (9.1 vs 3.5, P < .001) was significantly higher in those requiring reoperative surgery ( Table 1 ). Similarly, group 2 reported a larger mean tumor size as compared with group 1 (3.0 vs 2.0 cm, P < .001). Thus, a higher number of positive lymph nodes and a larger tumor size upon first thyroid cancer diagnosis are associated with an increased risk of necessitating a second thyroid operation. Last, ETE (46.3% vs 13.2%, P < .001) and ENE (25.9% vs 2.4%, P < .001) were more prevalent in group 2. Therefore, malignant spread beyond the thyroid gland and affected lymph nodes is associated with a greater risk for requiring a second surgical procedure.
Group Analyses
Variables such as age, time from first surgical procedure to the second, tumor size, number of MLNs, and MLNR were compared between males and females in group 2, and none were statistically different ( Table 2 ). Interestingly, although not significant, males exhibited a larger tumor size when compared with females (mean, 3.7 vs 2.6 cm; P = .061). Moreover, in females, the mean age at the time of initial surgery was 7.1 years younger than males (45.6 vs 52.7 years, P = .115), while a greater number of MLNs (mean, 11.7 vs 7.0; P = .063) and higher MLNR (mean, 0.71 vs 0.56; P = .090) were reported for males. The mean time from first surgical procedure to the second for all patients in group 2 was 702.3 days (1.92 years) with a standard deviation of 809.5 days (2.22 years) and, although not significant, was longer in females (765.2 days) vs males (610.8 days). Moreover, surgical parameters for the first and second procedures were compared. Initially, all patients underwent either a total (36/54, 66.7%) or hemi-/subtotal (18/54, 33.3%) thyroidectomy. Further, the second operation consisted of 13 partial, hemi-, or subtotal thyroidectomies (24.1%), while the remaining patients underwent neck dissections only (41/54, 75.9%). All patients underwent a limited compartment neck dissection during the first and second procedures.
Logistic Regression
Based on the univariate analyses, the following variables were entered into a binomial logistic regression model to identify the independent risk factors for reoperative surgery: sex, bilateral neck dissection (BND), lateral neck dissection (LND), number of MLNs, tumor size, ETE, and ENE ( Table 3 ). Patients were excluded from the analysis if any data points were missing. The final model included 458 patients in group 1 and 39 in group 2 and was statistically significant (χ 2 [7] = 54.0, P < .0001). Of those undergoing 1 surgical procedure, the model correctly predicted 98.9% of cases (specificity). However, just 15.4% of those necessitating a second surgical procedure were correctly classified by the model as having received one (sensitivity). The overall percentage accuracy in classification was 92.4%. The positive and negative predictive values of the model were 54.5% and 93.2%, respectively. Of the 7 variables, LND, number of MLNs, and tumor size were the only prognostic factors identified to statistically contribute to the model. Thus, the odds of thyroid reoperation increased by a factor of 7.8 (95% CI, 2.523-24.083), 1.1 (95% CI, 1.032-1.152), and 1.3 (95% CI, 1.064-1.559) if a patient initially received an LND, had a greater number of MLNs, and had a larger tumor size, respectively.
Support Vector Machine Model
The support vector machine model developed for this study did not achieve successful prediction rates. When all patient demographics and disease and surgical factors were used as predictor variables, the number of patients retained by the model was reduced from 2266 to 311. Patients were eliminated due to missing data for at least 1 of the variables considered. The reduced number of data points caused the model to be severely underfit, which compromised its performance as measured by its misclassification rate. To mitigate this problem, certain predictor variables were selected for their relevance and for the greater availability among the patients. The group of predictor variables selected to train the model were age, sex, total thyroidectomy, LND, BND, tumor size, malignancy type, ETE, and ENE. This allowed for a total of 2061 patients to be used for the development of the model.
Discussion
While recurrent/persistent thyroid cancer malignancies requiring surgery are uncommon, they pose an increased surgical risk for patients. Based on the univariate analyses, being of male sex and undergoing either a BND or LND at the initial surgery was associated with a greater risk of reoperation. Moreover, a higher number of MLNs and larger tumor size, in addition to having a malignancy exhibiting ETE or ENE, were all factors associated with an increased risk of eventually requiring a second procedure. Furthermore, the logistic regression model was statistically significant. Of the 7 variables, LND, number of MLNs, and tumor size were the only factors that contributed significantly to the model. Moreover, the machine learning algorithm was not conclusive and could not adequately predict the need for a second procedure due to the low number of patients necessitating one (2.4% of the total patient data set).
Patient Demographics
While female sex was more prevalent in both groups, the proportion of male patients was higher in the group requiring reoperation. These results suggest that when a thyroid malignancy requiring surgery is diagnosed in a male, the odds of cancer recurrence or persistence is greater. In line with our findings, studies have showed that men with an established thyroid cancer diagnosis have a worse prognosis, often translating to higher mortality and lower disease-free survival rates. 8 However, importantly, the more aggressive thyroid malignancy subtypes, such as anaplastic and medullary, have equal incidence rates between males and females. 9 Thus, this observed discrepancy between sexes is often attributed to the phenomenon that males generally present with more advanced cancer upon initial diagnosis as opposed to more aggressive pathologic subtypes. 9 Our study contributes to existing research by showing that males have a greater risk of cancer recurrence or persistence, which may be contributing to generally poorer prognosis in this population.
Surgical Factors
Of significance, we found that those eventually requiring a second surgical procedure were more likely to have undergone either a BND or LND during the initial operation. Extensive dissection is an indicator of disease spread to regional structures such as lymph nodes. Importantly, while the presence of lymph node metastases has been shown to be an indicator of disease recurrence, it is unclear whether it is also a good prognostic tool for evaluating survival.10,11 Interestingly, a study conducted by Ohshima et al concluded that bilateral modified radical neck dissection in those with risk factors for aggressive disease should be undertaken to prevent a second operation. 11 However, while this study does not contradict this finding, we show that those undergoing a BND or LND are at an increased risk for reoperation.
Disease Characteristics
Multiple disease factors examined in this study were significantly different between the groups. For those patients with recurrent or persistent cancer, we report a higher number of MLNs and a larger tumor size. Similar results have been reported previously. In a study evaluating papillary thyroid cancer, higher MLNR and larger tumor size were significantly correlated with cancer recurrence. 12 Similarly, Tran et al indicated that in those with papillary thyroid cancer, an initial tumor size measuring >2 cm is associated with a 5-time increased risk of recurrence when compared with that measuring <2 cm. 13 Analogously, in a systematic review, a tumor size >2 cm was a significant risk factor for papillary cancer recurrence. 14 In line with the literature, our findings highlight the importance of considering disease factors such as tumor size and number of MLNs when evaluating risk of cancer recurrence or persistence.
Moreover, ETE and ENE were more prevalent in those eventually requiring a second procedure. These results are consistent with the ones we presented earlier. Those requiring a second procedure are more likely to have cancer exhibiting spread outside the thyroid gland to surrounding lymph nodes and tissues, thereby necessitating more extensive dissections, including LND and BND. Given these findings, we posit that greater disease spread increases the risk that remaining cancer cells persist, sufficiently multiply, and eventually become a clinically detectable cancer necessitating reoperation. The aforementioned mechanism is in line with the concept of a disease reservoir following initial treatment, which can be undetectable or detectable via biochemical or imaging modalities but likely leads to persistent disease. Recent research suggests that reoperation for thyroid cancers may result largely from persistence of original disease as opposed to recurrence. 15 In fact, in a study conducted by Bates et al evaluating 92 reoperations for thyroid cancers, just 3 procedures (3.2%) were performed for true recurrent cancers, while the majority, 71 reoperations (77.2%), were attributed to persistent initial malignancies. 15 Persistent disease was ascertained in cases when any of the following 3 parameters were met at follow-up within 1 year of initial surgery: abnormal ultrasound, elevated thyroglobulin, or persistent elevated thyroglobulin antibodies. 15 Furthermore, in instances when the time interval from first to second procedure is minimal, Bates et al theorized that patients are likely never disease-free during that interval, leading to eventual clinically relevant persistent malignancy. We report a mean elapsed time of 702.3 days (22.7 months) between the first and second procedures, similar to the median time to reoperation (21 months) in the cohort examined by Bates et al. Thus, in our cohort of patients, it should be suspected that a large proportion of reoperations are from disease persistence from a potential reservoir as opposed to recurrence. This information may have important implications for adjuvant therapies and clinical follow-up.
While this study adds to the growing body of literature on this topic, there are certain limitations that should be mentioned. First, our sample size is modest and did not allow for subanalyses among different types of cancers or for adequate machine learning prediction modeling. Second, length of follow-up for group 1 was variable and determined per clinical parameters, which does not allow for comparison between the groups. Third, preoperative data, such as number of MLNs identified on preoperative ultrasound, were not available. These data should be collected in the future as certain preoperative disease factors could also be contributing to an increased risk of recurrence. Last, with the advent of molecular genetics and its role in thyroid cancer, future studies should aim to evaluate relevant genetic mutations and markers as potential risk factors for cancer recurrence. 16
Conclusion
Male sex, BND, LND, larger tumor size, and greater number of MLNs, in addition to larger tumor size and the presence of ETE or ENE, are risk factors associated with requiring a second operation for recurrent or persistent thyroid malignancies. Many of these findings are in line with the current literature. Prospective studies with larger samples sizes and additional disease factors, including genetic markers, are needed to further understand the role of patient, disease, and surgical factors on the risk of reoperation in the context of thyroid cancer persistence or recurrence. Such research would allow for identification of prognostic factors able to predict recurrent thyroid surgery more accurately.