
Abstract
Introduction
Granulomatosis with polyangiitis (GPA), formerly known as Wegener’s granulomatosis, is a rare anti-neutrophil-cytoplasmic-antibody (ANCA)-associated vasculitis that is characterized by necrosis and granulomatous inflammation of small blood vessels.1,2 The exact etiology of GPA is unknown but it is believed to be related to a dysfunction in the immune response to environmental triggers, including infectious agents and autoantigens, resulting in the overproduction of Th1 and Th17 cytokines. 3 This response leads to the formation of inflammatory granulomas within the vasculature. ANCA is present in 80% to 90% of patients with active GPA and is responsible for the activation of neutrophils, which can induce damage to endothelial cells in this multisystemic disease. 4 This dysregulation of the immune system may predispose patients with GPA to the development of cancer. 5 Further investigation of this potential association has been performed to assist clinicians in their understanding of the relationship between GPA and cancer.
Previous studies evaluating the occurrence of malignancies in patients with GPA have defined an increased risk of bladder cancer, lymphomas, non-melanoma skin cancers, leukemia, and liver cancer compared to a control population.6-9 Although the most common location of GPA vascular involvement is the upper respiratory tract (70%-100% of cases), there appears to be no definitive reported association between head and neck cancer (HNC) and GPA in the literature. 1 In the head and neck, GPA typically involves the nasal cavity and paranasal sinuses in 85% to 100% of cases. 1 Several case reports have observed the occurrence of squamous cell carcinoma of the nasal cavity arising in patients with GPA.10,11 In addition, Knight et al 8 demonstrated through a large population-based cohort study that patients with GPA had an increased standardized incidence ratio (SIR) of cancer of the oral cavity, pharynx, nose, and middle ear; however, the sample size was small (N = 3) and did not reach statistical significance. Our objective in this study was to examine whether patients diagnosed with GPA have an increased incidence of cancer in the head and neck, including disease of the sinonasal, nasopharynx, oral cavity, oropharynx, and larynx.
Materials and Methods
Study Design
To assess the odds of developing HNC in patients with GPA, we designed and implemented a retrospective cohort study using the TriNetX analytics platform. The experimental study population included all patients with an ICD-10 encounter diagnosis of GPA between October 2003 and October 2023. The control population included all adult patients without a GPA ICD-10 encounter diagnosis treated through an outpatient visit with the utilization of low medical decision-making between October 2003 and October 2023. To be included in the experimental cohort, patients had to have an ICD-10 encounter diagnosis of GPA (ICD-10-CM M31.3). To be included in the control cohort, the patients had to have a Current Procedural Terminology code for an outpatient visit of 99203. Patients within the control cohort were excluded if they had an ICD-10 encounter diagnosis of GPA (ICD-10-CM M31.3). Patients from both the GPA and non-GPA cohorts were excluded if they had an HNC diagnosis prior to the index event. Figure 1 provides an overview of our cohort selection.
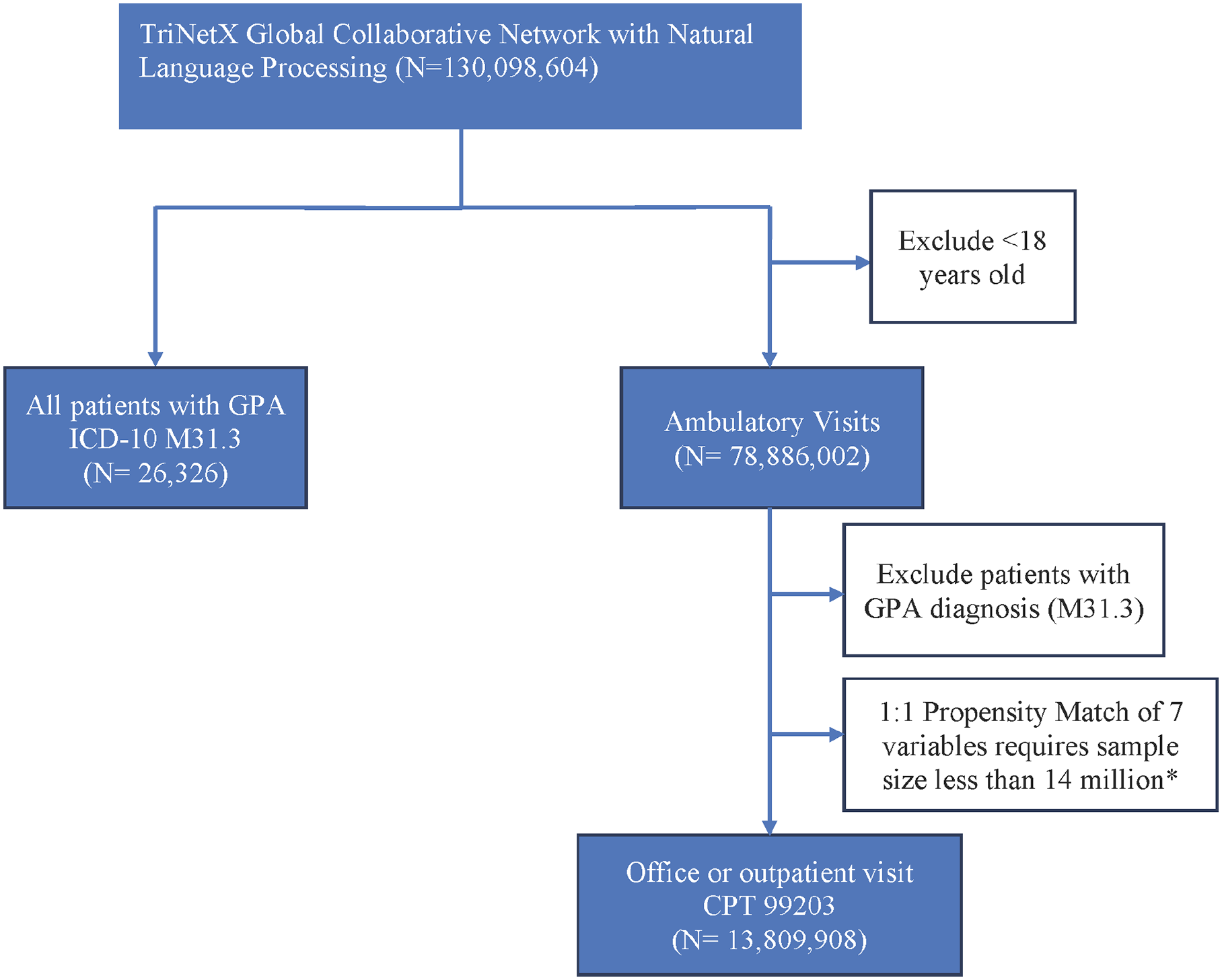
Cohort selection within the TriNetX Analytics Platform is used to compare the incidence of head and neck cancer at various anatomical subsites.
Variables
The primary outcome of this study is to assess the incidence of HNC, including subsite analyses of sinonasal, nasopharynx, oral cavity, oropharynx, and larynx diagnosed concurrently or after the corresponding index event in patients with and without GPA. The index events for the control and GPA cohorts were the time of the new patient visit in the outpatient setting and the diagnosis of GPA, respectively. Table 1 shows the ICD-10 codes used to define the various HNC subsites assessed in this study. This analysis is being performed to determine whether an ICD-10 encounter diagnosis of GPA is associated with an increased incidence of HNC.
The Anatomical Subsites Included in the Analysis of Patients Diagnosed with Cancer of the Sinonasal, Larynx, Nasopharynx, Oropharynx, and Oral Cavity in Patients with (GPA) and Without (Control) Granulomatosis with Polyangiitis.
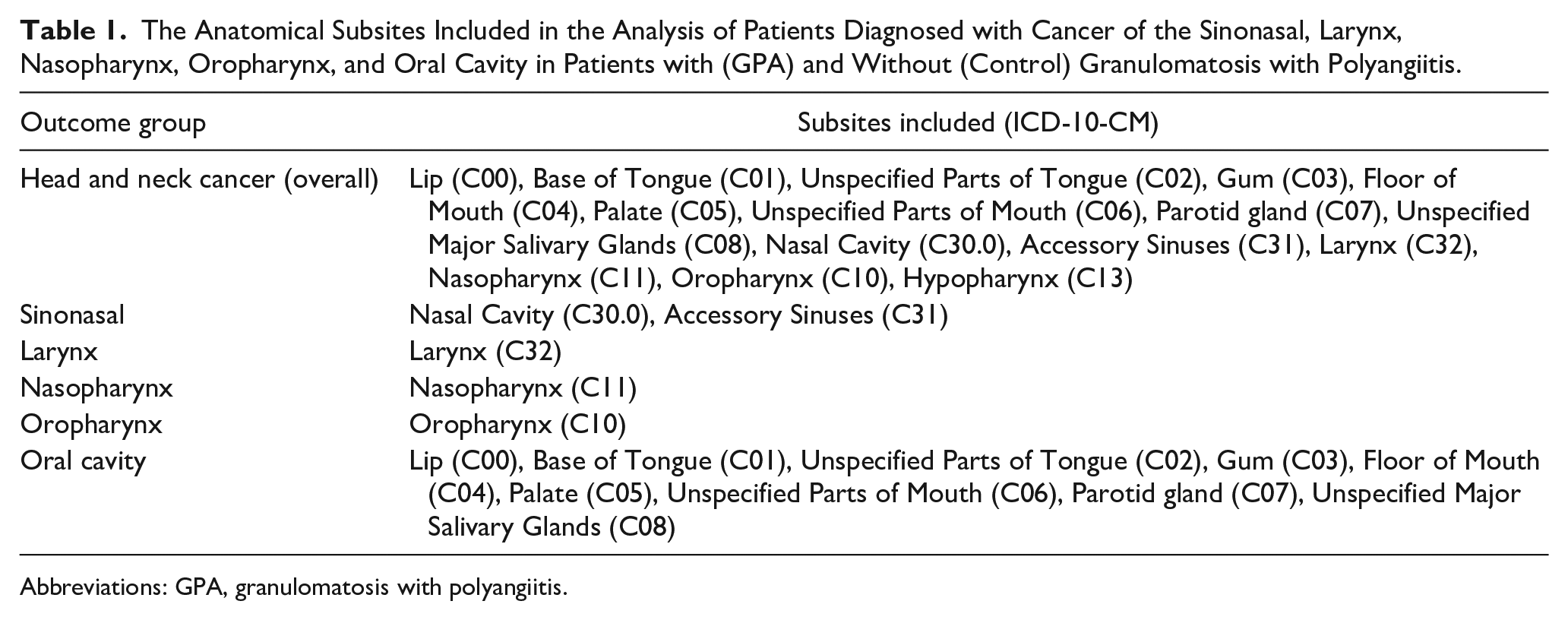
Abbreviations: GPA, granulomatosis with polyangiitis.
We also performed 1:1 propensity matching between the GPA and non-GPA cohorts to ensure similar baseline characteristics of known head and neck risk factors to control for potential confounding variables that may increase the risk of HNC other than GPA. Our analysis was performed with and without matching for the following head and neck risk factors, including age at index event, male sex, human papillomavirus (HPV) and Epstein Barr virus (EBV) exposure, tobacco use, and alcohol use, as described in Table 2. 12 We matched for age as 60% of patients with HNC are over 60, indicating the risk of this cancer increases with age. 13 Male sex has also been shown to increase the risk of HNC independent of alcohol and tobacco use. 14 We also matched for alcohol and tobacco use as these variables are the two strongest independent risk factors for HNC. 15 Since EBV is a risk factor for nasopharyngeal cancer, we balanced for recorded detectable EBV DNA (viral load) in serum or plasma of 3 IU/mL or greater by nucleic acid amplification with probe detection in the 1:1 propensity matching (LOINC 43730-1). 16 Lastly, we matched for HPV in the 1:1 propensity matching as it is a known driver of primarily oropharyngeal cancer and a lower percentage of other HNCs. 17
The Balanced Covariates for Each Outcome Group for the Analysis of Head and Neck Cancer in Patients with (GPA) and without (Control) Granulomatosis with Polyangiitis.
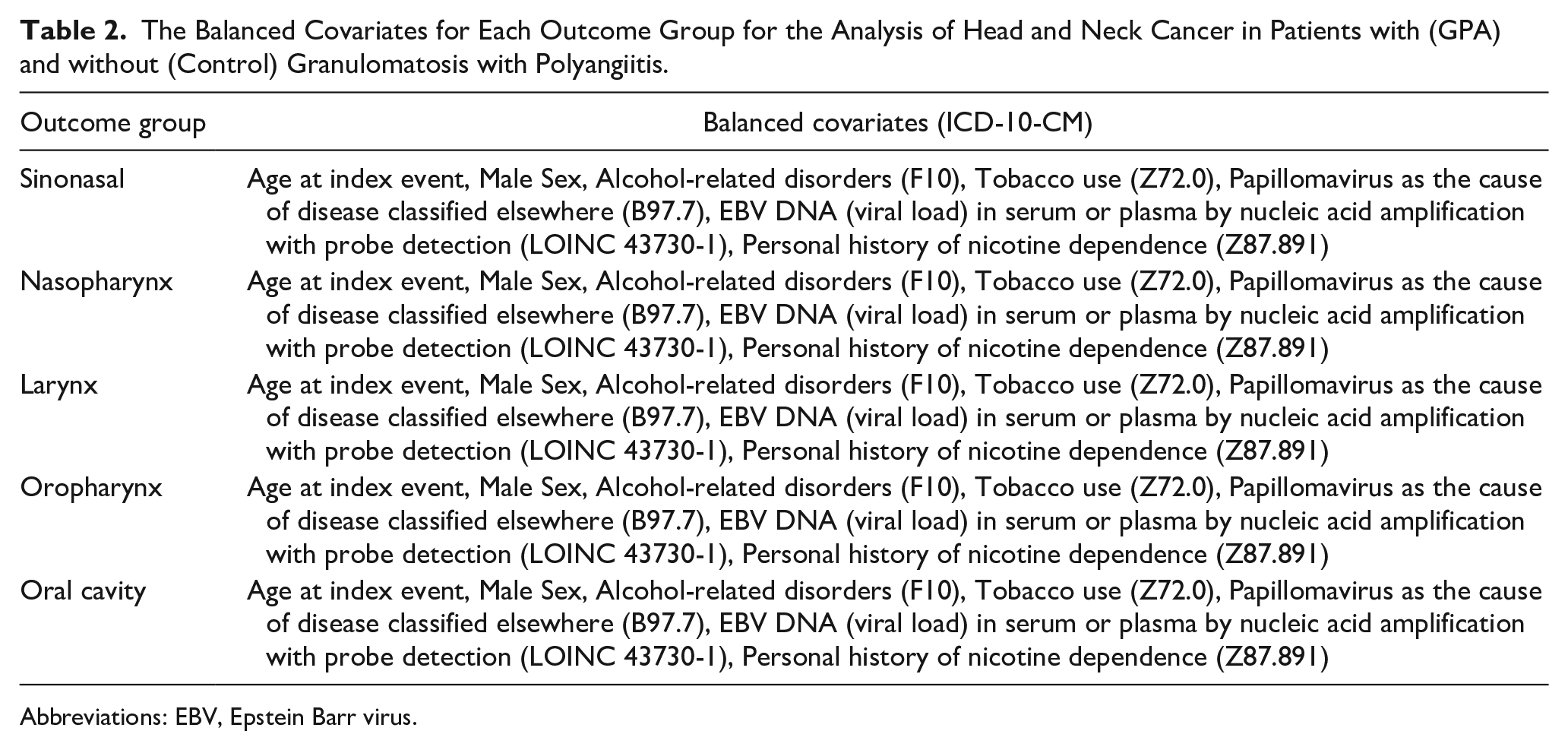
Abbreviations: EBV, Epstein Barr virus.
Data Collection
A retrospective cohort design was implemented for this study using TriNetX Analytics Network, a federated health research network that aggregates the data of 130,098,604 patients across 107 healthcare organizations (HCOs) from 15 countries, including the United States (Global Collaborative Network with Natural Language Processing). The database only contains de-identified data and has been deemed exempt from the Western Institutional Review Board by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule. Two primary patient groups were identified before variable balancing (Supplemental Materials):
GPA group (experimental), n = 26,131.
Patients without GPA (control), n = 13,693,201.
We were unable to assess the histological subtypes of the cancer cases for each anatomical location as the majority of the HCOs did not provide this data to the TriNetX analytics platform.
Statistical Analysis
All statistics were performed using the TriNetX built-in advanced analytics tools for comparison of cohorts as completed in previous studies.18,19 Odds ratios (OR) between the experimental and control cohorts were calculated with a 95% confidence interval (CI). The platform compares baseline and matched patient characteristics with chi-squared tests for categorical variables and independent sample t-tests for continuous variables. The TriNetX platform was used to perform 1:1 propensity matching between the GPA and non-GPA cohorts utilizing logistic regression. The TriNetX platform uses nearest-neighbor matching. The platform uses a matched tolerance level of 0.01 and a standardized difference between propensity scores of less than or equal to 0.1. All analyses within the TriNetX Analytics Network were performed on October 5, 2023.
Results
Before 1:1 Propensity Matching
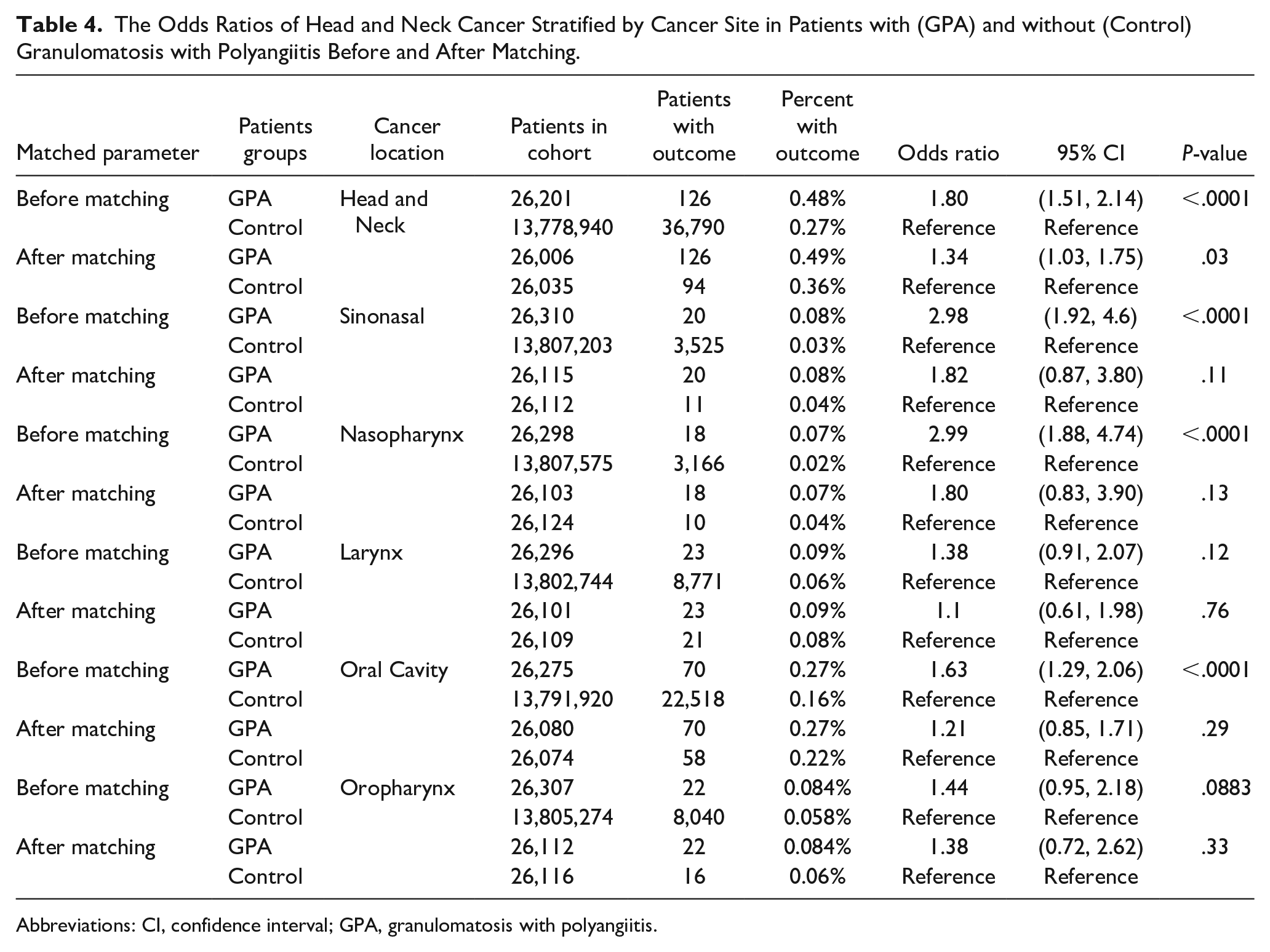
Prior to matching between the GPA and control cohort, there was a total of 26,131 patients with and 13,693,201 without GPA. The GPA patients were significantly older than the control patients (55.8 ± 18.3 vs 45.4 ± 20, P = <.001). The GPA patients were also more likely to be male compared to the control patients (43.9% vs 42.8%, P = <.001). The GPA patients had statistically significant increased exposure to HNC risk factors defined by ICD-10 and LOINC codes, including prior history of nicotine dependence, tobacco use, alcohol use disorders, and EBV and HPV infections, as shown in Table 3. Of the patients in the GPA cohort, 126 (0.48%) had an ICD-10 diagnosis of HNC. When stratifying by head and neck subsites, 20 (0.08%), 18 (0.07%), 23 (0.09%), 70 (0.27%), and 22 (0.084%) GPA patients had an ICD-10 encounter diagnosis of cancer involving the sinonasal, nasopharynx, larynx, oral cavity, and oropharynx. Patients with GPA were at an increased risk for a diagnosis of HNC compared to a control population when including all subsites with an OR of 1.80 (OR: 1.51-2.14). The subsites with a statistically significant increased risk of cancer in GPA patients compared to the control cohort included sinonasal, nasopharynx, and oral cavity, as shown by the ORs in Table 4.
Demographics and Characteristics of Patients with (GPA) and without (Control) Granulomatosis with Polyangiitis Matched by Age, Tobacco Use, Alcohol-related Disorders, and Papillomavirus-caused Disease.
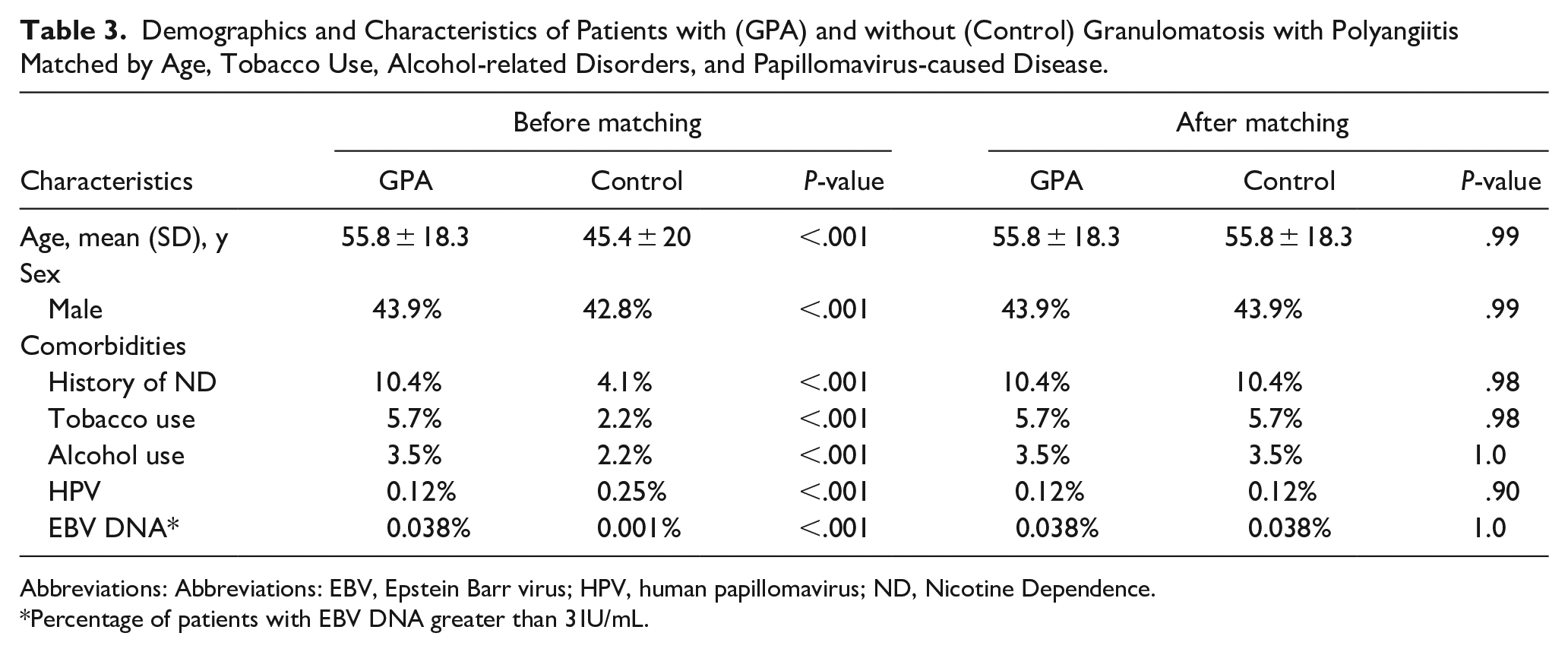
Abbreviations: Abbreviations: EBV, Epstein Barr virus; HPV, human papillomavirus; ND, Nicotine Dependence.
Percentage of patients with EBV DNA greater than 3 IU/mL.
The Odds Ratios of Head and Neck Cancer Stratified by Cancer Site in Patients with (GPA) and without (Control) Granulomatosis with Polyangiitis Before and After Matching.
Abbreviations: CI, confidence interval; GPA, granulomatosis with polyangiitis.
After 1:1 Propensity Matching
After 1:1 propensity matching between the GPA and control cohort, there was no statistical difference in age at index, male sex, tobacco use, history of nicotine dependence, alcohol use disorders, and EBV and HPV exposure between the groups. The matched analysis indicated patients with GPA were at an increased risk of HNC compared to the control population (OR = 1.34, 95% CI: 1.03, 1.75). Cancer of each anatomical subsite was found to occur more often in patients with GPA; however, there was no statistical difference in any of the subsites examined between the groups. There were trends toward statistical significance, as the incidence of an ICD-10 diagnosis of sinonasal cancer concurrently or after an ICD-10 diagnosis of GPA was nearly two times greater than the control, as shown in Table 4.
Discussion
In this current study, we identified that patients who are diagnosed with GPA are at an increased risk for HNC independent of several known risk factors. To our knowledge, this is the first study in the literature to identify a statistically significant association between HNC and GPA.
When stratifying by anatomical subtype, GPA patients were at a statistically significant increased risk of sinonasal, nasopharyngeal, and oral cavity cancer. However, this significance was lost after 1:1 propensity matching. It remains likely that GPA patients are at an increased odds for an ICD-10 diagnosis of sinonasal cancer, as the incidence was nearly twice as high in the GPA cohort as in the control group. However, even with a large database like TriNetX, this study does not have the power to obtain statistical significance due to the rarity of sinonasal cancer. Although HNC is the seventh most common cancer globally, the incidence is low, with an estimated 890,000 cases per year. 20 As a result, incidences in this analysis are small due to the relative rarity of these conditions.
The management of GPA involves a multidisciplinary team of physicians, including rheumatologists, pulmonologists, otolaryngologists, cardiologists, and nephrologists, due to the multisystemic nature of the disease. 3 With the complexity and wide array of specialty physician involvement in the medical care of patients with GPA, we believe our findings indicate the importance of patient-physician coordination to encourage thorough clinical evaluation of patients with GPA by an otolaryngologist for symptoms related to the sinus, nose, and throat. This is because symptoms related to active GPA and HNC, like sinonasal cancer, can be indistinguishable, as clinical manifestations of both conditions include nasal obstruction, rhinorrhea, and epistaxis.21,22 While our analysis focused on assessing the association between GPA and HNC, several other studies in the literature have identified an increased risk of cancer at different anatomical locations in patients with GPA.
Previous assessments of cancer incidence after diagnosis of GPA have been conducted through nationwide databases, single-institution retrospective studies, and prospective multi-institutional clinical trials.6,8,9,23,24 Of these five studies, all but one identified patients with GPA to have an overall increased risk of cancer, with SIRs ranging from 1.6 to 3.8.6,8,9,24 When assessing the occurrence of bladder cancer among patients with GPA, Knight et al and Faurschou et al both reported statistically significant SIRs of 4.8 and 3.6 when compared to a healthy control population, respectively.8,9 The high incidence of bladder cancer in patients with GPA has been linked to medical management with cyclophosphamide, which suggests the cancer is not secondary to ANCA-associated vasculitis.7,9 Furthermore, additional analyses have identified statistically significant increases in the occurrence of liver cancer, 8 leukemia,8,9 lymphoma, 8 and non-melanoma skin cancer8,9 in patients diagnosed with GPA. Interestingly, while the nasal cavity and paranasal sinuses are the most common locations of GPA involvement in the head and neck, only Knight et al 8 included these subsites within their analysis. In their study, the combined SIRs for cancer of the oral cavity/pharynx and nose/middle ear were 1.9 (95% CI: 0.2-6.9) and 14.1 (95% CI: 0.4-7.9), respectively. Our findings reinforce this potential increased risk of HNC in patients with GPA.
GPA is not the only autoimmune and inflammatory disorder to be associated with cancer, as rheumatoid arthritis, 25 systemic lupus erythematous, 26 and primary Sjögren’s syndrome 27 have all been reported to have statistically significant increases in overall cancer risk. The current hypothesis related to the development of cancer in patients with chronic autoimmune disorders is related to the effect of immune system dysregulation.28,29 However, since our analysis included patients diagnosed with GPA before and concurrently with their HNC diagnosis, it is also reasonable to consider whether this ANCA-associated vasculitis is secondary to the HNC in some rare cases of concurrent diagnoses.
Several different types of cancers have been linked with the development of vasculitis, including lymphoid and myeloid cancers, myelodysplasia, and various solid tumors.30-33 However, previous studies have reported malignancy-associated vasculitis to only amount to approximately 0.4% to 4.2% of all vasculitis cases.34-36 A study by Pankhurst et al 37 specifically assessing the incidence of cancer before or concurrent with the diagnosis of ANCA-associated vasculitis in 200 British patients reported a 6-fold increase in cancer occurrence compared to a healthy control population. Although the study does not differentiate between GPA and microscopic polyangiitis, their findings indicate GPA may develop as the result of cancer development. In prior case reports evaluating patients with GPA and nasal cavity carcinoma, GPA has been reported to precede cancer, and our study suggests that HNC may develop after a GPA diagnosis.
This study has several limitations. We were unable to define the histological subtypes of the HNC, as the data are noted provided by the majority of HCOs included within the TriNetX platform. While this study evaluates the risk of cancer among the largest number of GPA patients to date in the literature, the number of cancer cases in each subgroup remains low due to the rarity of each condition, limiting our overall sample size. This prevented our study from being adequately powered to identify the head and neck subsites with statistically significant increased risk of diagnosis in patients with GPA. Lastly, the increase in cancer diagnoses among patients with GPA diagnoses may also be due to detection bias, as patients with active disease may be followed by physicians more frequently and more thoroughly.
Conclusion
In conclusion, the odds of HNC are higher in patients with a concurrent or prior diagnosis of GPA after matching several HNC risk factors. Of studies examining the association between cancer and GPA, this current study provides the largest sample size to date in the literature, suggesting reliable correlative results in our findings. While this study indicates there is a potential association between HNC and GPA, future large-population-based studies are needed to confirm the anatomical subsites with the highest risk of cancer in patients with GPA.
Supplemental Material
sj-docx-1-ear-10.1177_01455613231223409 – Supplemental material for Assessing the Association Between Head and Neck Cancer and Granulomatosis with Polyangiitis
Supplemental material, sj-docx-1-ear-10.1177_01455613231223409 for Assessing the Association Between Head and Neck Cancer and Granulomatosis with Polyangiitis by David Hoying, Ian Dorney, Todd Otteson, Jason Thuener and David C. Kaelber in Ear, Nose & Throat Journal
Footnotes
Data Statement
Our data can be accessed via the TriNetX platform.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by the Clinical and Translational Science Collaborative of Cleveland, which is funded by the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Science Award grant, UL1TR002548. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Ethical Approval
The MetroHealth System does not require ethical approval for this article because the TriNetX platform has been deemed exempt from the Western Institutional Review Board (IRB) by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule.
Statement of Human and Animal Rights
This article does not perform any experimental procedures on human or animal subjects.
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained because the TriNetX platform reports only de-identified data and has been deemed exempt from the Western Institutional Review Board (IRB) by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.