
Abstract
We present a case of a 50-year-old male who complained of a sore throat persisting for 2 months. Upon physical examination, multiple mucous patches were observed in the oropharynx region, but no skin lesions were found. Fiberoptic laryngoscopy confirmed these findings. The Treponema pallidum particle agglutination test and toluidine red unheated serum test (TRUST) were positive with a titer of TRUST 1:64. The patient admitted to engaging in extramarital sexual activities with several females but no males. Based on the clinical manifestations and laboratory test results, a diagnosis of secondary syphilis of the oropharynx was established. He was treated with 2.4 million units of benzathine penicillin G by intramuscular injection once a week for 3 weeks. After 1 month, the lesions completely disappeared without any symptoms. The titer of TRUST reduced to 1:2 in 1-year follow-up. This report aims to enhance physicians’ understanding and recognition of oropharyngeal syphilis, enabling timely diagnosis and effective management.
Introduction
Syphilis is a well-known systemic sexually transmitted disease caused by the bacterium Treponema pallidum, capable of infecting various organs. The clinical presentation of syphilis can differ depending on the stage of infection. Cutaneous and mucosal lesions are frequently observed during secondary syphilis. And the oral cavity is the most commonly involved in addition to the sexual organs and skin in this stage. However, the unusual clinical presentation of oral syphilis often leads to misdiagnosis or oversight in clinical practice. In this report, we present a case of secondary syphilis exhibiting oropharyngeal symptoms, highlighting the importance of recognizing and diagnosing this form of the disease accurately.
Case Report
A 50-year-old male presented with a persistent sore throat for approximately 2 months. The symptoms were aggravated by speaking and swallowing and accompanied by mild hoarseness and cough, but no dyspnea, stridor, or weight loss. The patient sought assistance at the otolaryngology department of our hospital. The fiberoptic laryngoscopy examination revealed the presence of multiple mucous patches in the oropharynx region, spanning bilateral pharyngeal side walls, lingual surface of the epiglottis, and most of the pharyngeal side wall extending to the piriform fossa (Figure 1(a)). The epiglottis was slightly swollen, and the surface of both vocal cords appeared smooth.
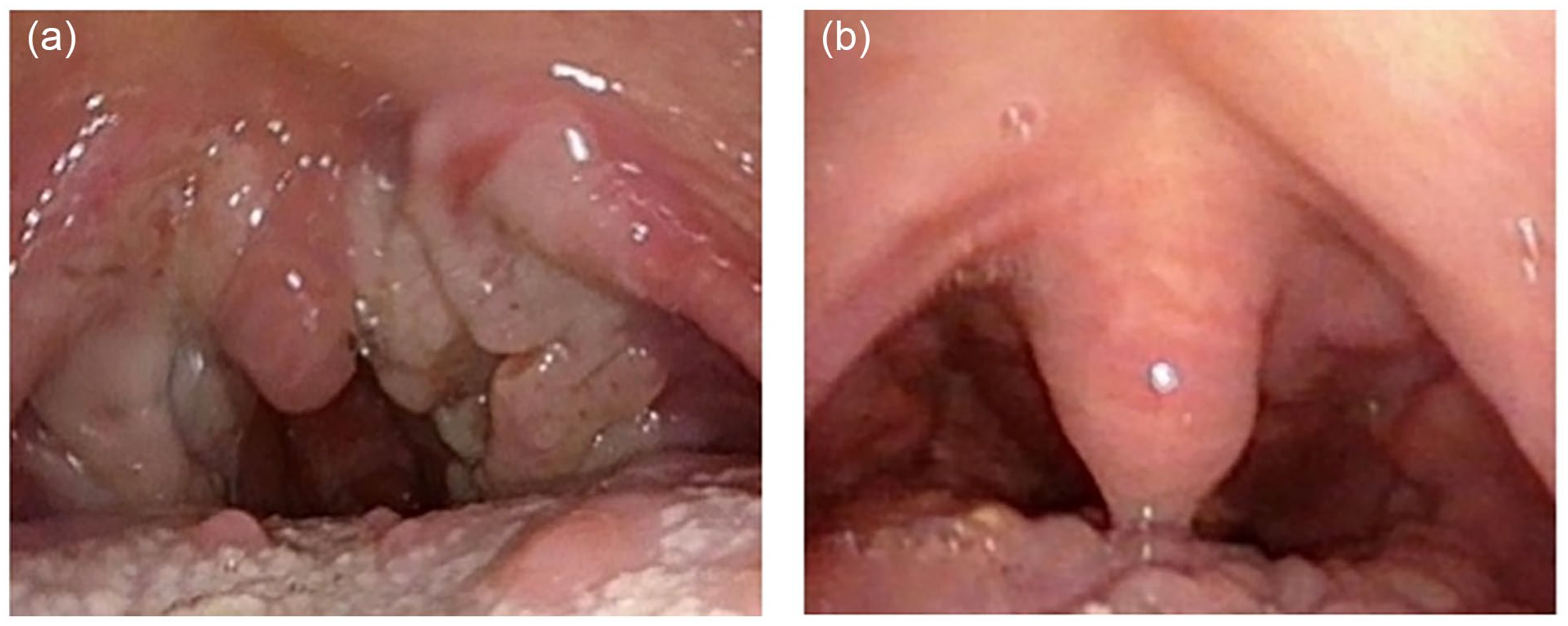
(a) Gray-white mucous patches on the soft palate and posterior pharyngeal wall. (b) The lesions on the soft palate and posterior pharyngeal wall disappeared 1 month after the treatment.
Given the characteristic findings observed during the endoscopic examination, the patient was suspected to have secondary syphilis and was subsequently referred to the department of dermatology. Following further inquiry, the patient admitted to engaging in extramarital sexual activities with several females, including oral sex, but denied any involvement with males.
Physical examination revealed gray-white patches on the soft palate and posterior pharyngeal wall, with hyperemia of the pharyngeal mucosa and tonsil I enlargement. These lesions were slightly elevated and surrounded by erythema. No superficially enlarged lymph nodes were palpable, and no generalized skin rashes or anogenital ulcerations were detected. Laboratory tests indicated normal liver and renal function, with negative results for human immunodeficiency virus antibody, viral hepatitis, and human papillomavirus (HPV) nucleic acid. However, both the Treponema pallidum particle agglutination (TPPA) test and toluidine red unheated serum test (TRUST) were positive with the titers of TRUST 1:64.
Based on clinical manifestations, laboratory tests and characteristics of endoscope examination, a diagnosis of secondary syphilis of the oropharynx was established. Treatment consisted of a 3-week course of 2.4 million units of benzathine penicillin G, administered once weekly. One month later, the lesions completely disappeared without any symptom (Figure 1(b)). After 1-year follow-up, the problem did not relapse without other reported skin lesions and the titers of TRUST reduced to 1:2.
Discussion
In recent years, there has been a global increase in the incidence of syphilis. It is known as “the great masquerader” due to its various presentations and multiple-system involvement. 1 Acquired syphilis is classified into 4 stages based on its activity and clinical manifestations: primary, secondary, latent, and tertiary. 2 Oral manifestations can be observed in any stage, while they are most commonly associated with the secondary stage. In a review by Schuch, out of 40 cases of acquired oral syphilis, 92.5% were diagnosed as secondary syphilis. 3 Approximately 25% of untreated primary cases can progress to secondary syphilis after several weeks to a few months. 4 Oropharyngeal lesions in secondary syphilis appeared as slightly elevated-type plaques, ulcerated and covered with pseudomembrane, or multiple mucous patches that may coalesce into serpiginous lesions, known as “snail-track ulcers.” 5 The lips, tongue, hard and soft palates, uvula, and tonsils are the most involved. Most patients do not experience obvious symptoms, although some may have mild throat pain and a foreign body sensation without fever. However, these clinical manifestations are nonspecific.
Syphilis is mainly transmitted through unprotected sexual behaviors, although occasional transmission can occur through blood contact or mother-to-infant vertical pathways. 6 Andrade et al. reported 4 clinical cases of oral syphilis, all of which were associated with the practice of oral sex. 7 Although the direct link between oral sex and oral syphilis remains unclear, it is considered a potential route of infection. The definitive diagnosis of oropharyngeal syphilis is based on serologic testing for Treponema pallidum, including TPPA, TRUST, venereal disease research laboratory, rapid plasma reagin, and direct detection of organisms using dark-field microscopy or polymerase chain reaction techniques. Histopathological examinations of syphilis are generally nonspecific and usually indicate the body’s response to the infection. 4 In our case, the lesions were predominantly observed in the oropharynx region, displaying typical gray-white mucous patches. Based on the clinical manifestation and serological tests, a diagnosis of secondary syphilis was made.
On certain occasions, the lesions of oropharyngeal syphilis may resemble whitish verrucous plaques, leading to a consideration of condyloma acuminatum as a differential diagnosis. Given the current epidemic of HPV-related oropharyngeal squamous cell carcinoma, it is crucial to distinguish syphilis from carcinoma. Ameya et al. reported 6 cases of oropharyngeal syphilis which presented similar to squamous cell carcinoma of the oropharynx. 8 Additionally, other conditions like aphthous/traumatic ulcers, fungal infections, pseudoepitheliomatous hyperplasia, lichenoid mucositis/lichen planus, immune-mediated vesiculobullous disorders, and even dysplasia should also be considered in the differential diagnosis. 9
It was reported that about 8%-40% syphilis patients in early stage could develop into tertiary syphilis if they were not given regular treatment. 10 Early confirmatory diagnosis and immediate standard treatment are clinically crucial to prevent disease progression to tertiary syphilis and avoid complications affecting multiple systems. Due to the nonspecific and atypical clinical manifestations of oropharyngeal syphilis, it can be easily missed or misdiagnosed without the support of laboratory tests. This case serves as a reminder for physicians to enhance their understanding of syphilis involving the oropharyngeal region, enabling them to make accurate diagnoses and provide appropriate treatment.
Footnotes
Data availability statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.