
Abstract

Significance Statement
The case highlights the importance of comprehensive analysis of the root cause of dysphonia. On examination, bilateral supraglottic cysts were detected; however, the vocal fold paresis and compensatory hyperfunction were the primary causes of his symptoms. This case demonstrates that targeted voice therapy can yield substantial improvement in vocal endurance and range, ultimately avoiding the need for surgical intervention in select cases.
A 42-year-old male singer presented to our office complaining of voice fatigue and dysphonia. He was the lead singer in a 4-piece band. Starting a year prior to our evaluation, he had encountered difficulties singing, often straining his voice to compensate during performances, which resulted in odynophagia. He struggled with intermittent phonation breaks and gradual development of voice fluctuations without diplophonia. His past medical history was significant for laryngopharyngeal reflux which had been treated with esomeprazole and he was referred due to bilateral vocal fold masses observed on flexible laryngoscopic examination by a laryngologist elsewhere. Our office examination revealed bilateral vocal fold paresis which was confirmed with laryngeal electromyography showed bilateral recurrent laryngeal nerve (RLN) paresis and right superior laryngeal nerve (SLN) weakness with 40% to 50% decreased recruitment in both thyroarytenoid muscles and 20% decreased recruitment in the right cricothyroid muscle. Strobovideolaryngoscopy showed bilateral supraglottic masses, considered to be a right saccular cyst or possibly a right laryngocele, and a left saccular cyst extending slightly more cephalad (Figure 1). The cysts were in contact intermittently with the superior surfaces of the vocal folds and impaired movemement primarily on the right, especially during efforful phonation. Computerized tomography (CT) scan ruled out laryngocele. Both the vocal fold masses and the vocal fold paresis were concurrently considered as the possible root cause for the patient’s dysphonia, and initial treatment began with vocal therapy.
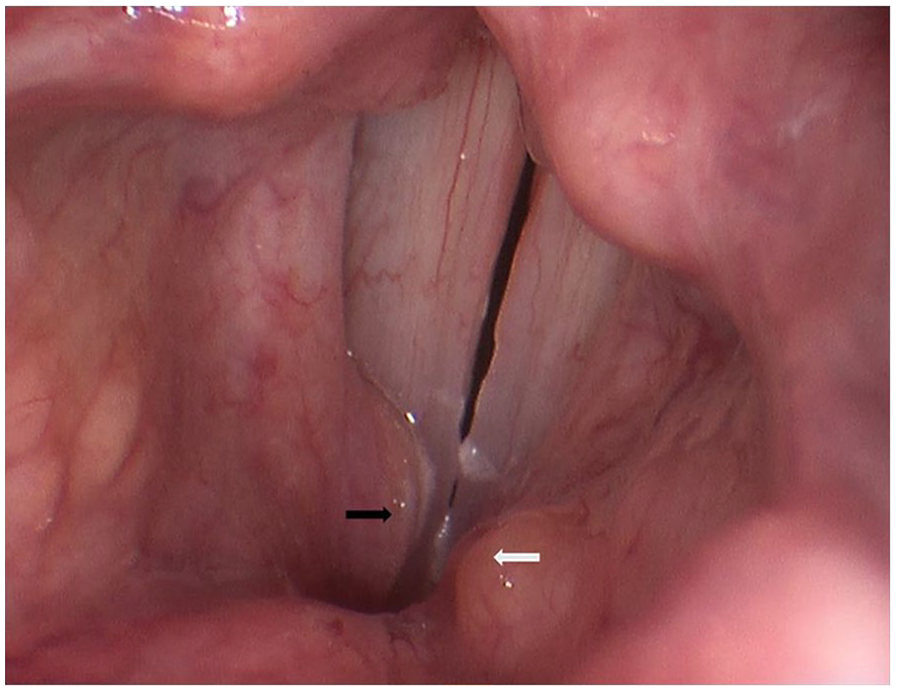
Stroboscopic examination at high pitch showing the right saccular cyst located in the anterior ventricle near the midline (black arrow) and the left-sided saccular cyst above the left false vocal fold near midline (white arrow).
Vocal fold paresis involves weakness in the RLN, SLN, or a combination of the 2. These conditions can have numerous causes, including iatrogenic injury during surgery, neurologic diseases, infections, trauma, and others. The clinical manifestations of vocal fold paresis and paralysis include symptoms such as dysphonia, hoarseness, breathiness, throat pain, and decreased vocal stamina. Unilateral RLN injury often presents as a breathy voice and may lead to diplophonia, aspiration, and dysphagia, while SLN injuries can result in changes in pitch, relatively monotone voice, decreased projection and vocal stability, and reduced high pitch range. Compensatory mechanisms such as muscle tension dysphonia may develop. In some cases, reinnervation occurs, but it often leads to synkinesis resulting in immobility or reduced mobility of the vocal fold. Treatment ranges from conservative voice therapy to surgical alteration of vocal fold position. 1
Laryngeal cysts are categorized by Desanto et al 2 as either ductal or saccular. Ductal cysts, typically smaller than 1 cm, are mucus retention cysts originating from the mucous membranes. They can be visualized on a CT scan as fluid-filled structures located from the inferior boundary of the hyoid bone to the vestibular folds. Saccular cysts, are typically larger, often measuring between 1 cm and 7 cm. Saccular cysts arise from the submucosal plane within the laryngeal saccule and can be visualized on a CT scan as fluid-filled cysts. 3 Saccular cysts can develop congenitally, presenting with early obstructive dyspnea and noisy breathing in neonates. 4 Acquired saccular cysts seldom result in airway compromise; more commonly, acquired saccular cysts present later in life with voice changes. 5 Saccular cysts can be classified further as anterior or lateral. Anterior saccular cysts are found within the saccular orifice and are visible in the anterior glottic airway. Lateral saccular cysts expand into the laryngeal vestibule, and can affect supraglottic anatomy at the level of the aryepiglottic folds, false vocal folds, and epiglottis.6,7
In this patient, differential diagnoses included laryngocele, which is seen on a CT scan as an air-filled dilation originating from the laryngeal saccule and enlargens during a Valsalva maneuver. 8 This differs from saccular cysts, which remain fairly stable during a Valsalva maneuver and which are not filled with air. Rare cystic causes of dysphonia associated with distortion of supraglottic structures include thyroglossal and third brachial cleft cysts. These conditions typically present with physical exam findings in the external neck, in addition to classic features visible on a CT scan.9,10
This patient’s symptoms were primarily due to vocal fold paresis and associated hyperfunctional compensation, not the cysts. The patient underwent conservative management with voice therapy, which significantly improved his vocal stamina. Subsequently, the patient was able to achieve a greater voice range, including higher tones. When the hyperfunction was eliminated, the cysts did not contact the vocal folds and were not symptomatic. So, surgery was not requried.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.