
Abstract
Introduction
Sinonasal and skull base malignancies account for 3%-5% of all head and neck malignancies and less than 1% of all tumors.1-3 They can occur anywhere from the frontal sinus to the clivus, and can involve the anterior, middle, and posterior intracranial fossae. These tumors are characterized by an initial absence of clear symptoms or the presence of symptoms similar to those of benign diseases. Consequently, patients are frequently diagnosed with sinonasal and skull base malignancies at an intermediate or advanced stage of disease when the tumor mass would have already infiltrated the skull base nerves, blood vessels, and vital organs, posing a grave risk for patient survival.
Various tumors are categorized as sinonasal and skull base malignancies, including advanced sinonasal squamous cell carcinoma, adenoid cystic carcinoma, olfactory neuroblastoma, malignant meningioma, chondrosarcoma, and chordoma of the clivus. Although the complexity of these malignancies may necessitate diverse therapeutic strategies, over the past few decades, treatment modalities have shifted toward surgical resection and personalized adjuvant treatments instead of conservative approaches.4,5 However, the complex anatomy of the skull base, limited field of view associated with endoscopy, and potential for tumor-induced damage of vital organ function can result in a series of postoperative complications. 6 The intensive care unit (ICU) is often used to prevent these situations.
The ICU is an important part of the medical system because it provides critically ill patients with high-level care, including vital sign monitoring, mechanical ventilation, and medication management, to maintain patient stability and ensure effective treatment. 7 ICU care has become a common practice to ensure the postoperative safety of patients who have undergone surgery for sinonasal and skull base malignancies. However, the high cost of the ICU imposes certain limitations on its utilization and adds to the financial burden of patients.
In observational studies, confounding may occur because of differences in the distribution of baseline characteristics measured between groups, which may lead to biased impact estimates. Therefore, propensity score matching (PSM) analyses have been widely used to obtain unbiased effect estimates. To address whether patients benefit from ICU care, we used PSM to evaluate its effect on the incidence of complications among patients. These results would help clinicians make informed decisions regarding the necessity of ICU care and optimize patient care while minimizing healthcare costs.
Patients and Methods
Study Population
This retrospective study was approved by the Ethics Committee of the Affiliated Hospital of Qingdao University. One hundred and fifty-one patients with sinonasal and skull base malignancies admitted to our hospital between November 2014 and November 2022 were enrolled in our study. The inclusion criteria were as follows: age of 18 years or older, diagnosis of sinonasal and skull base malignancies that was confirmed by histopathology, tumor stage T3 or T4 according to the 8th edition of the American Joint Committee on Cancer, 8 and pure endoscopic surgery or combined endoscopic and external approach surgery. The exclusion criteria were as follows: benign diseases in the sinonasal and skull base regions, stage T1 or T2 malignant tumors, non-curative or palliative surgery, immunodeficiency or pregnancy, metastasis confirmed before surgery, and insufficient clinical data.
Patient demographic and clinical information, including sex, age, body mass index, and chronic medical diseases (diabetes, hypertension, and cardiac disease), were collected from the electronic medical record system. Information related to the procedure, such as surgical approach, dural matter exposure, operating time, intraoperative bleeding volume, and use of electromagnetic navigation, was also collected. Moreover, we calculated the modified frailty index for all patients based on previous literature, which included 11 variables. 9 All patients were followed-up for at least 3 months after surgery. Smoking was defined as the consumption of more than 1 cigarette per day for at least 1 year, irrespective of the age at which the patient started smoking and the duration since quitting smoking. Drinking was defined as consuming alcohol more than twice per week for more than 6 months. An anesthesiologist evaluated the physical condition of the patients before surgery, according to the American Society of Anesthesiologists (ASA) classification system. 10
During this study, we identified the types of postoperative complications based on studies conducted by Deschler et al 6 and Suh et al 11 ; these complications were classified as surgical or medical. Surgical complications included orbital injury, diplopia or visual changes, cerebrospinal fluid leakage, epistaxis, and chylous leakage. Medical complications included hypotension/shock, delirium, meningitis, respiratory tract infections, myocardial infarction, and hypoalbuminemia. We also investigated the readmission rate after a 3-month follow-up.
PSM Analysis
In this study, a PSM analysis was performed using the “MatchIt” package of R software (version 4.2.2 for Windows; Bell Laboratories, Murray Hill, NJ, USA) and the 1:1 nearest neighbor matching method. A caliper (0.2) was used to adjust for covariate imbalances and minimize bias between groups.
Statistical Analysis
All statistical analyses were performed using SPSS 27.00 (IBM Corp., Armonk, NY, USA) and R software (version 4.2.2). Descriptive statistics for categorical variables are presented as frequencies and percentages, and comparisons were performed using Pearson’s chi-square and Fisher’s exact tests. Continuous variables were tested for normality and analyzed using either Student’s t test or the Mann–Whitney U test. Risk factors were determined using a logistic regression analysis for multivariate analyses. All tests were 2 sided, and P < .05 was considered statistically significant.
Results
Patient Characteristics
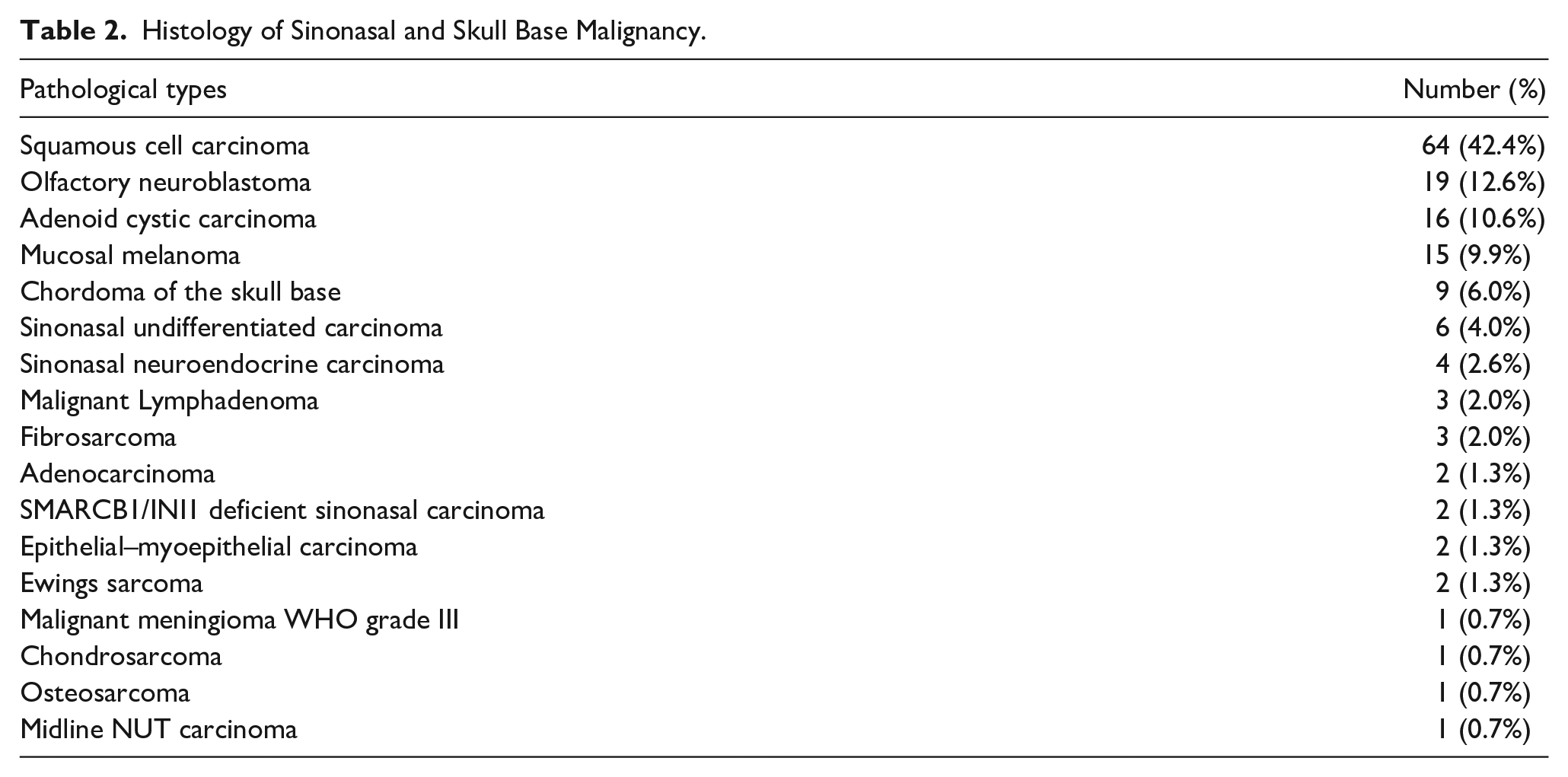
This study included 151 patients. The majority of these patients were men (109 patients; 72.3%). The age of the patients ranged from 20 to 81 years (average age, 57.87 years), and 45 patients were older than 65 years of age. Stage T4 disease was observed in 108 patients (77.1%), whereas stage T3 disease was observed in 32 patients (22.9%). Furthermore, 120 patients (79.5%) underwent surgery, and 73 patients (48.3%) underwent dura mater exposure during surgery. In addition, this study included 17 different pathological types of tumors. The most common type was squamous cell carcinoma (64 cases; 42.4%), followed by olfactory neuroblastoma (19 cases; 12.6%) and adenoid cystic carcinoma (16 cases; 10.6%). Detailed patient characteristics are shown in Tables 1 and 2.
Characteristics of Patients With Sinonasal and Skull Base Malignancy.
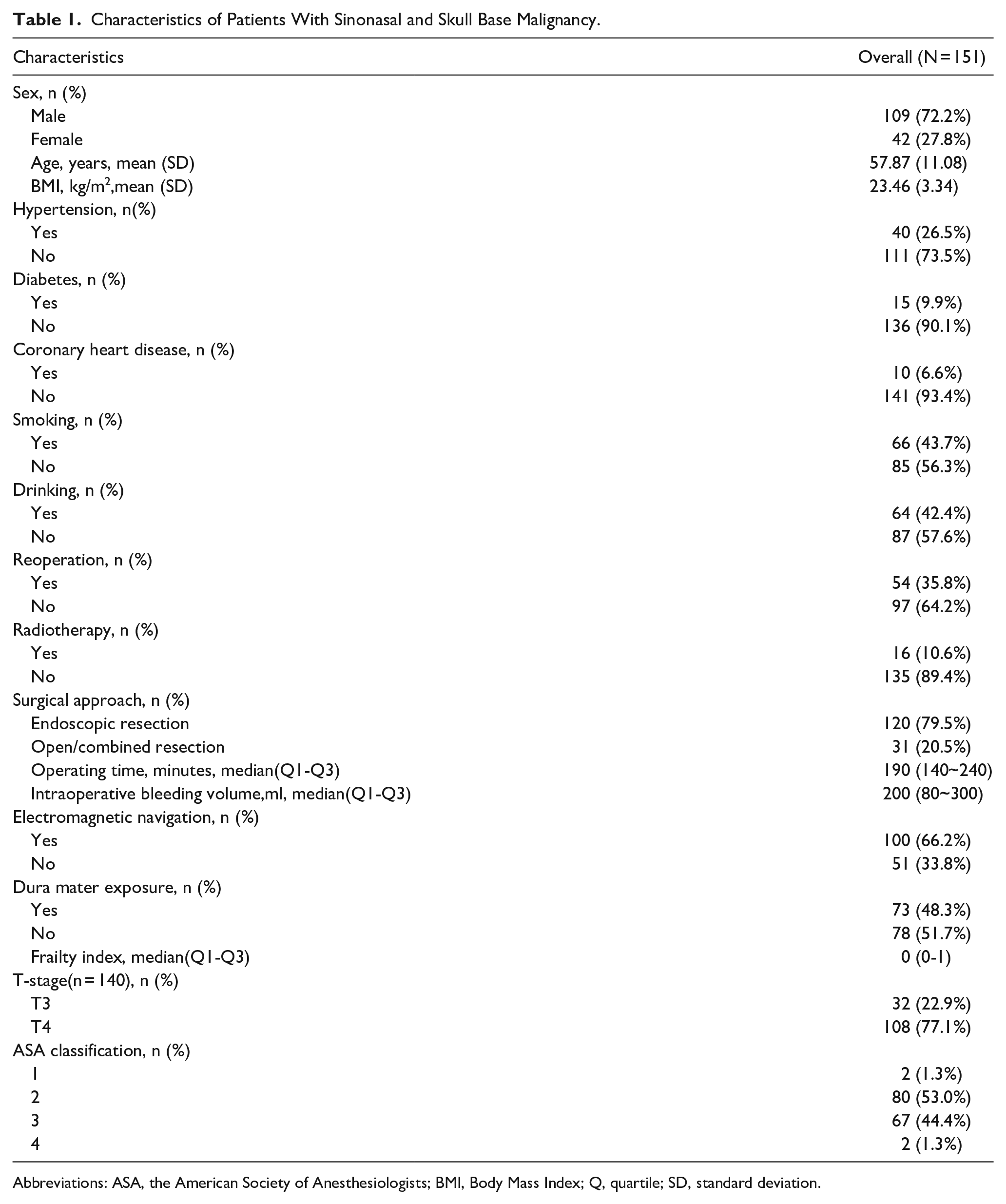
Abbreviations: ASA, the American Society of Anesthesiologists; BMI, Body Mass Index; Q, quartile; SD, standard deviation.
Histology of Sinonasal and Skull Base Malignancy.
Complication Rates and Associated Factors
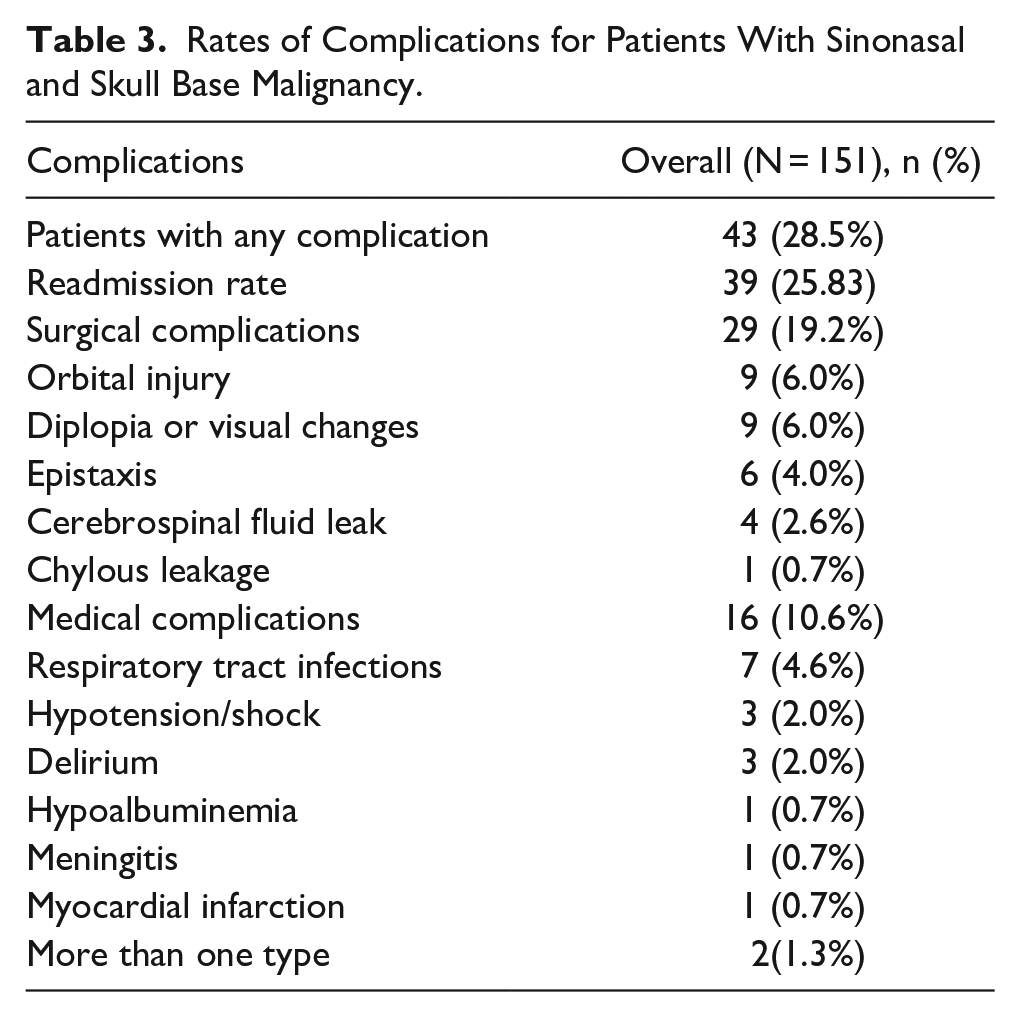
Among the cohort of 151 patients, 43 (28.5%) experienced complications. The most common surgical complications were orbital injury (n = 9) and diplopia or visual changes (n = 9). Respiratory tract infections (n = 7) were the most common medical complications. In addition, 2 patients experienced more than one type of complication. The readmission rate of patients was approximately 25.83%. The specific types of complications are listed in Table 3. Patient characteristics were analyzed to determine whether they were associated with the occurrences of surgical, medical, and other complications (Supplemental Table 1). Hypertension was associated with an increased risk of surgical complications (P = .034).
Rates of Complications for Patients With Sinonasal and Skull Base Malignancy.
Impact of ICU on Complication Rates
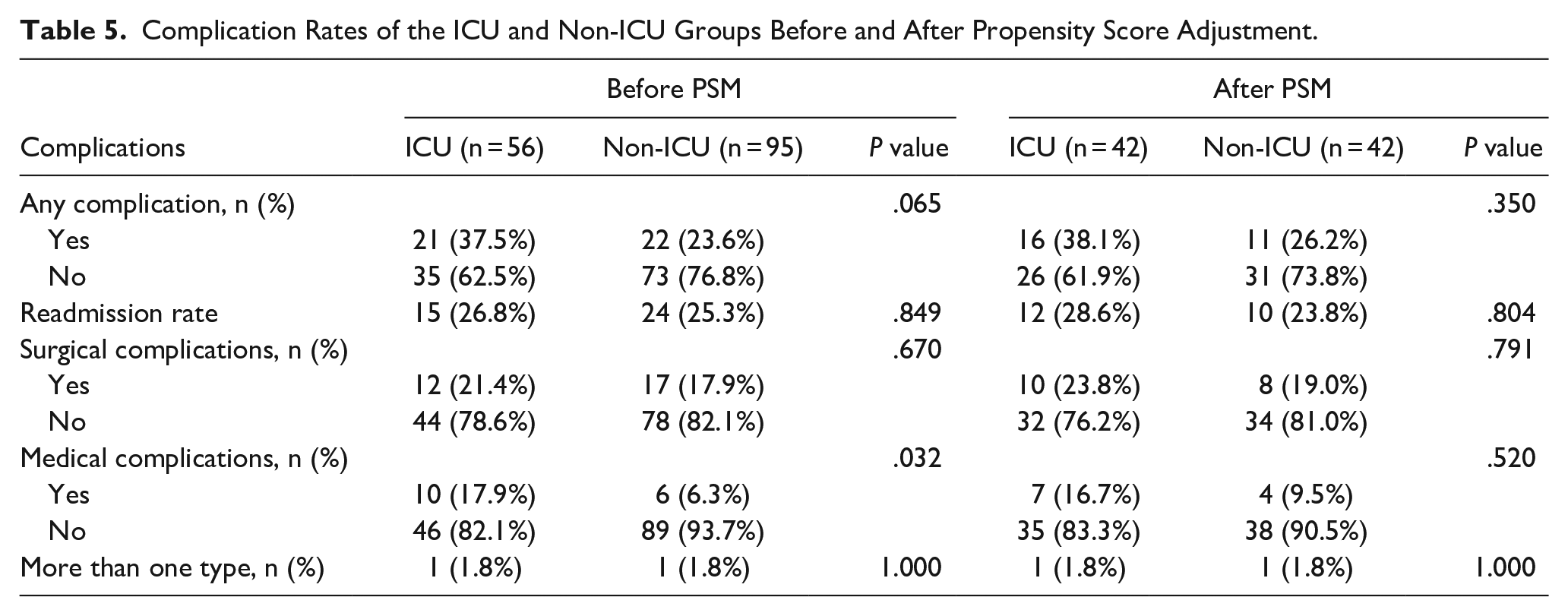
Fifty-six patients were admitted to the ICU after surgery. The baseline characteristics of the ICU and non-ICU groups before and after PSM are presented in Table 4. Statistically significant differences in sex, smoking, drinking, radiotherapy, dura mater exposure, and ASA classifications were observed between groups before adjustment by PSM. PSM was performed using these variables to generate a matched population with balanced covariates. Before PSM, patients admitted to the ICU had a significantly higher incidence of medical complications (P = .032) than patients in the non-ICU group. However, after PSM, no significant difference was observed in the incidence of complications between groups. The detailed results are presented in Table 5. The rates of individual complications after adjustment by PSM are presented in Supplemental Table 2. No differences in readmission rates between the 2 groups were observed before or after PSM.
Baseline Characteristics of the ICU and Non-ICU Groups Before and After Propensity Score Adjustment.*
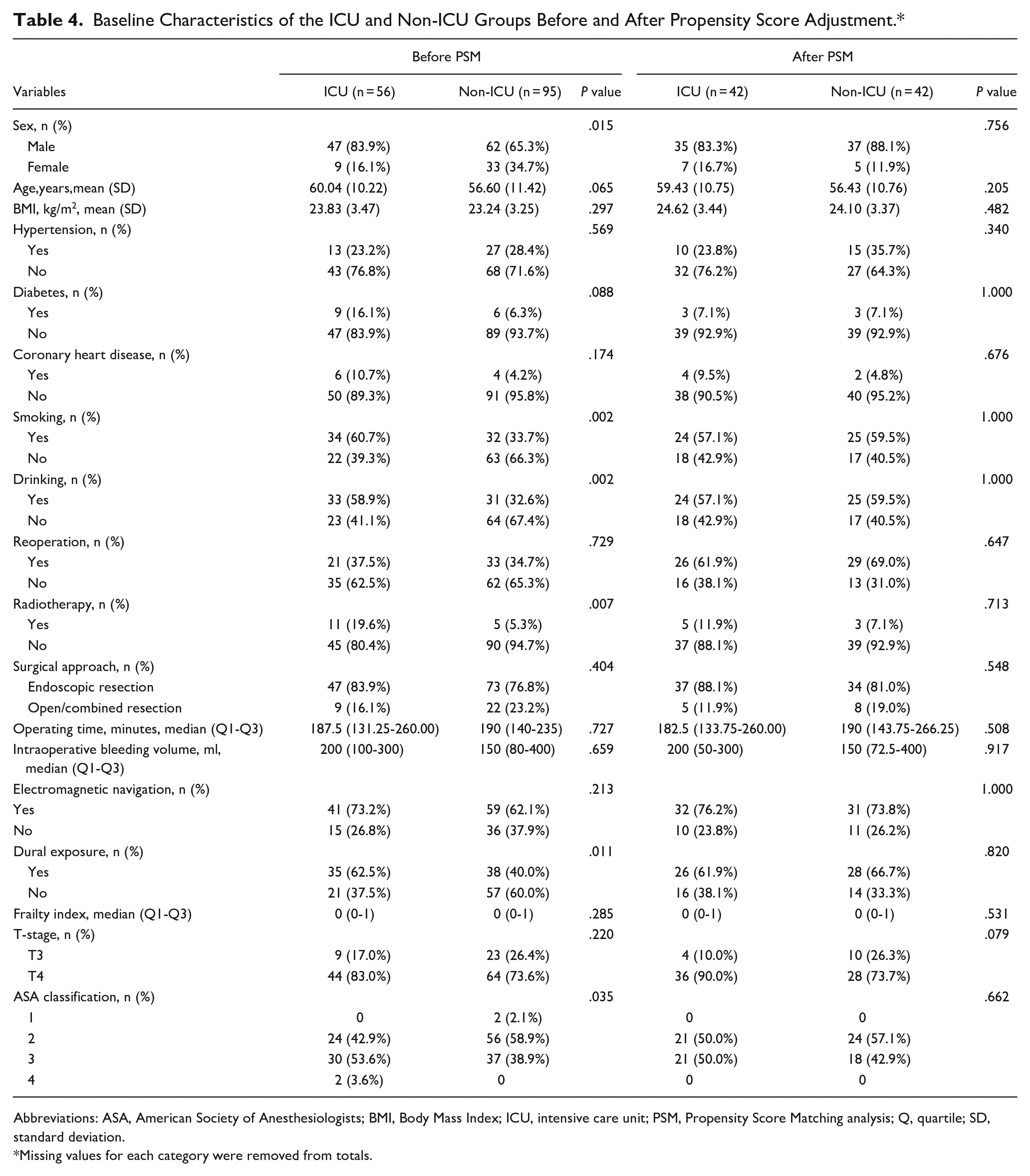
Abbreviations: ASA, American Society of Anesthesiologists; BMI, Body Mass Index; ICU, intensive care unit; PSM, Propensity Score Matching analysis; Q, quartile; SD, standard deviation.
Missing values for each category were removed from totals.
Complication Rates of the ICU and Non-ICU Groups Before and After Propensity Score Adjustment.
Multivariate Logistic Regression Analysis
To extrapolate the options for potential patient admission to the ICU, we performed a multivariate logistic regression analysis based on univariate analysis. Sex, smoking, drinking, radiotherapy, dura mater exposure, and ASA classifications were included in the analysis, which showed that patients could be considered for ICU care if they smoked, had undergone radiation therapy, and had intraoperative dural exposure (Table 6).
Multivariate Logistic Regression Analysis.
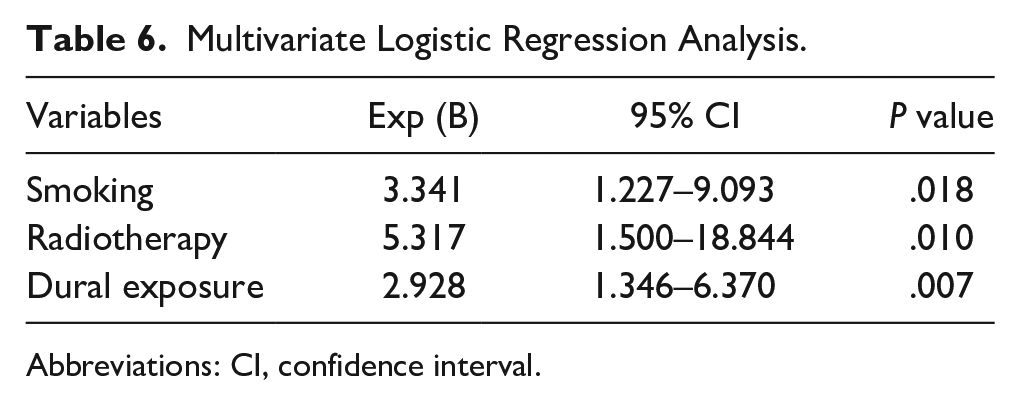
Abbreviations: CI, confidence interval.
Discussion
Sinonasal and skull base malignancies pose a clinical challenge, particularly for patients with advanced-stage disease, because tumors often invade critical structures of the skull base. Over the past few decades, advances in techniques ranging from craniofacial resection to endoscopic endonasal approach, as well as skull base reconstruction techniques, have led to improved surgical outcomes; however, complications cannot be completely prevented.5,12-16 In previous studies, the complication rates were approximately 36% for craniofacial resection and 29% for the endoscopic endonasal approach.17,18 In this study, the complication rate was 28.5%, which is not significantly different from those reported by previous studies. Several factors can influence the incidence of complications, such as tumor size, degree of tumor invasion, patient condition, and surgical approach.17,19,20 However, insufficient attention has been focused on the role of postoperative care.
Patients who undergo craniotomy are typically admitted to the neurosurgical ICU for postanesthesia management, neurological assessment, analgesic administration, and other nursing interventions. 21 ICU care is necessary for patients with severe underlying diseases. Such high risk patients who present with unstable vital signs or a comatose status are commonly admitted to the ICU after surgery or the development of complications for close monitoring and vital sign stabilization. Jerath et al 22 investigated ICU utilization and risk factors by analyzing data of 541,524 noncardiac surgery patients in Canada and found that factors such as patient age, health status, and surgery type affected ICU admission after surgery. Furthermore, they observed that patients admitted to the ICU developed a higher risk of mortality with longer hospital stay. However, because admission to the ICU mainly depends on the clinician’s experience, this grouping is non-randomized; therefore, during data analysis, large differences in the distribution of baseline characteristics between groups were observed. If these differences are not eliminated, they can cause bias in the results. Therefore, PSM analysis was performed to obtain an unbiased effect estimate. Notably, we specifically recruited patients with advanced malignancy because we hypothesized that this group would require more ICU care than patients with early-stage disease.
Our findings indicated that ICU-level care did not reduce the complication rates of these patients, thus validating the results of previous studies. A meta-analysis by Almeida et al found that routine ICU admission after elective intracranial neurosurgery may not confer any significant benefits to carefully selected patients and could lead to higher costs. 23 Similarly, Wunsch et al 24 observed no decrease in mortality rates at hospitals with higher rates of ICU utilization and Kahan et al 25 analyzed data from 27 countries and concluded that postoperative ICU admission did not improve survival outcomes.
The variations in study outcomes may be attributed to differences in study populations, disease types, and regional levels of development, which could affect the clinical significance of ICU utilization, particularly if patients admitted to the ICU have a poor health status. This may also explain why medical complication rates are higher among patients admitted to the ICU before PSM. After PSM, this difference disappeared, and ICU admission did not have an impact on complications. Therefore, we believe that the ICU offers more potentially preventive treatment for patients with sinonasal and skull base malignancies, and its use should be standardized to avoid unnecessary expenses.
Although the complexity of the pathologic types of skull base tumors makes it difficult to compare them with one another, and the need for postoperative ICU care is relatively low, we hope that this preliminary investigation, which explores the potential impact of ICU use, will provide fundamental data and insights for future in-depth studies. For this reason, we also used multivariate analysis to determine the factors influencing patient admission to the ICU, seeking potential clinical practice guidelines and evidence. The analysis revealed that smoking, radiotherapy, and dural exposure significantly influenced whether patients were admitted to the ICU after surgery.
Surgical complications were related to the patient’s surgical procedure, whereas medical complications were associated with postoperative care and dependent on the patient’s physical fitness. In addition to the complications mentioned in other publications, we included others, such as chylous leakage and delirium. These additional complications are highly relevant to the treatment course and contribute to the comprehensive analysis of the incidence of complications. Moreover, the use of a consistent and comprehensive list of complications by such studies is necessary to standardize the study process.
This study had several limitations. First, patient admission to the ICU depends on many factors, including the patient’s condition and doctor’s recommendation. However, certain factors that affect the effectiveness of ICU care, such as the patient’s economic level, healthcare awareness, cooperation, and the level of nursing care, were not included in the analysis. The ommision of these factors may introduce a higher level of uncertainty into the results of this study. Second, in this retrospective study, not only was the sample size small, but the integrity of some indicators, such as tumor volume, was impaired. Third, selection bias and the presence of confounding factors may have affected the accuracy of results, and old data may not be applicable to current clinical practice, considering the continuous advancement in hospital care. Therefore, the results of this study require further validation. Future multicenter collaboration may help expand the sample size and allow further investigation of the impact of ICU admission on the survival outcomes of patients with nasocranial base tumors.
Conclusion
Preliminary investigations have shown that ICU admission does not reduce the complication rate of patients with sinonasal and skull base malignancies, thus providing valuable insights regarding the rational allocation of medical resources and reduction of the economic burden on patients. Further studies are necessary to verify the impact of ICU admission and obtain a higher level of evidence.
Supplemental Material
sj-docx-1-ear-10.1177_01455613231215195 – Supplemental material for Association of Complication Rates and Intensive Care Unit Use With Sinonasal and Skull Base Malignancies: A Propensity Score Matching Analysis
Supplemental material, sj-docx-1-ear-10.1177_01455613231215195 for Association of Complication Rates and Intensive Care Unit Use With Sinonasal and Skull Base Malignancies: A Propensity Score Matching Analysis by Ce Wu, Longgang Yu, Lin Wang, Xudong Yan, Shunke Li, Junfeng Wen and Yan Jiang in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
This work was supported by grants from the Program for National Natural Science Foundation of China (81770978).
Consent Statements
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Natural Science Foundation of China.
Ethical Statements
This study was approved by the Ethics Committee of the Affiliated Hospital of Qingdao University.
Grant Number:
81770978.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.