
Abstract
Goiter with substernal extension is common, with a reported incidence of up to 20% in patients undergoing thyroidectomy. It has been shown that the vast majority of substernal goiters can be removed through a cervical incision. However, if this is not possible, a sternotomy is usually required, which could add significant morbidity to an otherwise routine operation. During substernal mobilization, the surgeon’s finger is typically placed under the strap muscles and against the thyroid capsule, hooking around the inferior aspect of the gland to facilitate separation of the gland from its mediastinal attachments. In cases where the length required for successful substernal mobilization is beyond the reach of a surgeon’s fingers, the use of an alternative strategy may be required. A surgical spoon is a blunt, curved instrument that can allow safe substernal mobilization while providing the added length needed when digital mobilization is inadequate. Here, we describe the use of a surgical spoon for the safe and successful removal of a goiter with substernal extension unable to be removed with digital manipulation.
Keywords
Introduction
Goiter with substernal extension is common, with a reported incidence of 1% to 20% in patients undergoing thyroidectomy. 1 The presence of substernal extension adds a layer of complexity to the surgical management, but the general consensus is that the vast majority can be removed through a traditional cervical approach. However, if the gland cannot be extracted safely through a cervical incision, a sternotomy may be required. The use of sternotomy can add significant morbidity to thyroid surgery, therefore the successful removal of a thyroid through a transcervical approach should be pursued whenever feasible.
Goiter which extends near or beyond the aortic arch, has been shown to significantly increase the need for sternotomy and complicate safe substernal thyroid mobilization. 2 During substernal mobilization, the surgeon’s finger is typically placed under the strap muscles and against the thyroid, hooking around the inferior aspect of the gland to facilitate separation of the gland from its mediastinal fascial attachments. A finger can successfully separate the thyroid from its mediastinal attachments while being blunt enough to minimize risk of damage to the aortic arch and its associated branches. In cases where the length required for successful substernal mobilization is beyond the reach of a surgeon’s fingers, the use of an alternative strategy may be required. A surgical spoon is blunt enough to allow safe substernal mobilization while providing the added length needed when one’s finger is inadequate. Here, we describe the use of a surgical spoon for the safe and successful removal of a goiter with substernal extension unable to be removed with traditional digital mobilization. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The authors declare that there is no conflict of interest. Informed consent for publication of the case and images in a de-identified fashion was obtained from the patient.
Case Report
A 75-year-old female presented with a several-month history of a slowly enlarging neck mass accompanied by compressive symptoms, including dysphagia but no shortness of breath. A thyroid ultrasound demonstrated an 8-cm right thyroid nodule and a 3.3-cm left thyroid nodule. A computerized tomography (CT) scan of the neck with contrast was obtained, which showed an enlarged right thyroid goiter with substernal extension and leftward tracheal deviation (Figure 1). Given the symptomatic nature with a concern it would continue to grow without intervention, the patient elected for total thyroidectomy. During the surgical exploration of the substernal extent of the goiter, we were unable to fully reach the inferior aspect to successfully mobilize it. It was at this point a surgical spoon was utilized with the concave bowl of the spoon placed medially against the goiter to successfully help mobilize the thyroid mass from its mediastinal fascial attachments (Figure 2). The entire thyroid was removed en bloc without complication (Figure 3). She was discharged on postoperative day 1 without any issues. Her surgical pathology revealed papillary thyroid microcarcinomas in bilateral thyroid lobes with negative margins. The decision was made for observation with close follow-up.
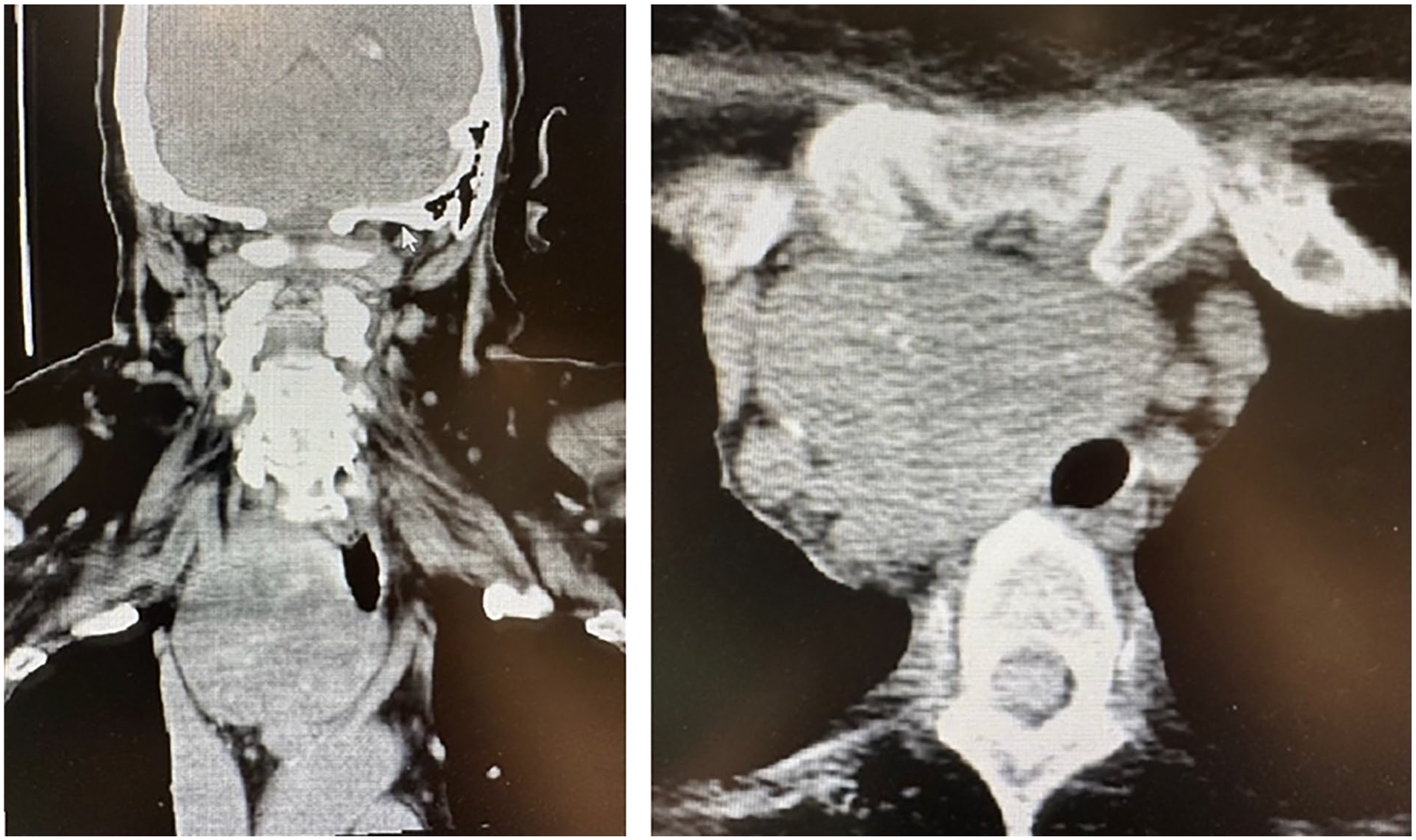
CT scan of the neck and chest with contrast demonstrates substernal extent of right thyroid goiter.
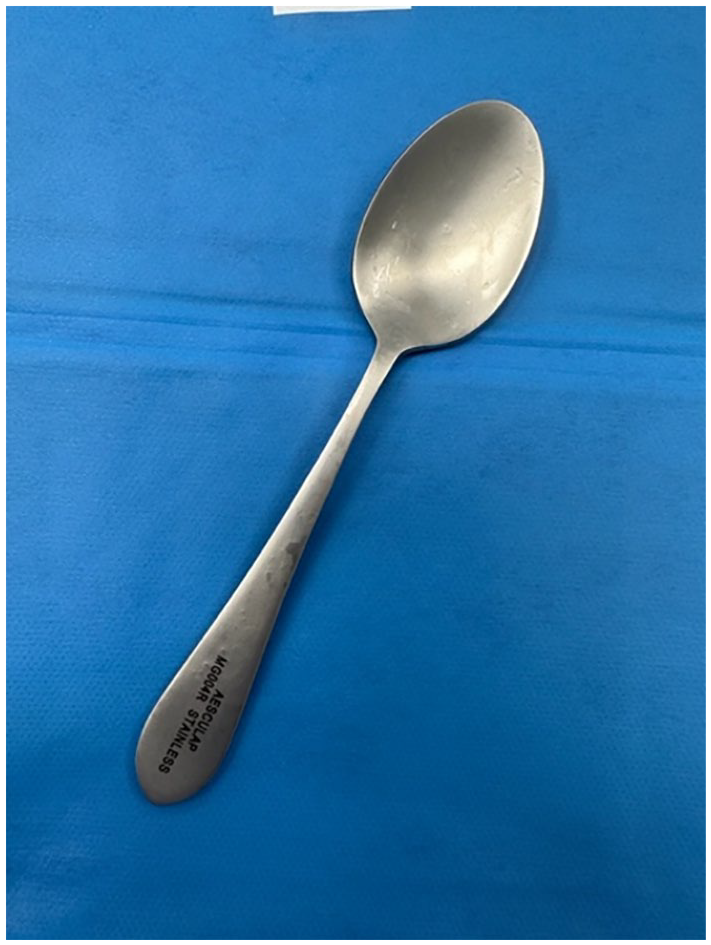
Sterile steel spoon used in substernal mobilization.
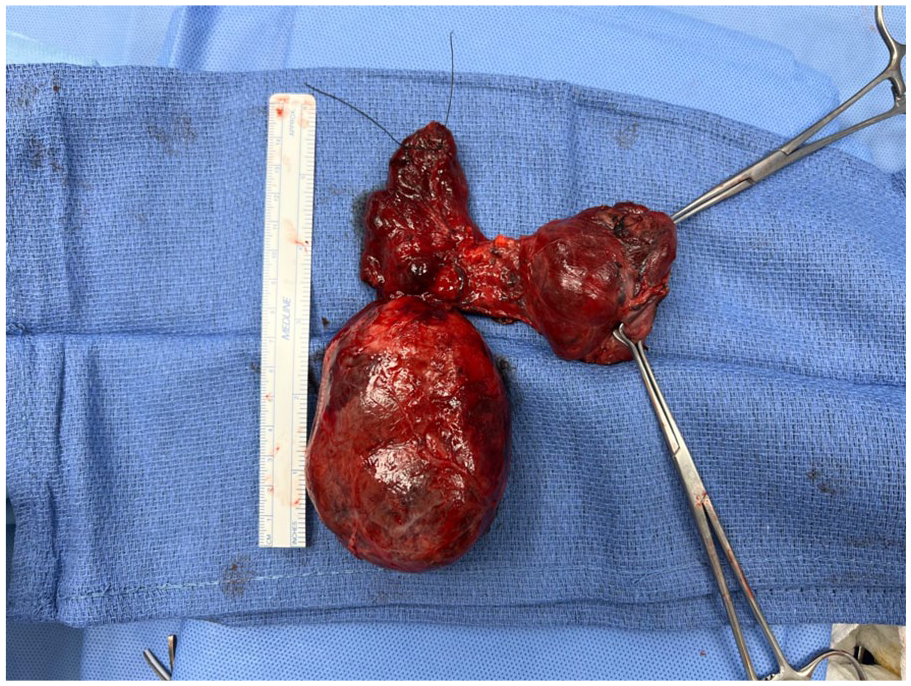
Large right goiter following successful removal.
Discussion
Substernal goiter is common, although there is no clear consensus on a clear definition. Commonly accepted definitions include a substernal goiter that has extended below the plane of the thoracic inlet, 3 or one that has more than 50% of its mass extending inferior to the thoracic inlet, 4 although several others have been proposed.5,6 Given this heterogeneity of the definition of substernal goiter, it comes with no surprise that incidence rates reported in the literature vary considerably, ranging from 1% to 20%. 1 Given the common nature of substernal extension, the ability of the thyroid surgeon to manage this pathology definitively and safely is of the utmost importance.
In patients with substernal goiter, the most common presenting symptoms include those of airway compromise, including dyspnea, orthopnea, and sometimes severe airway compromise. Less common symptoms include dysphagia, hoarseness, and superior vena cava syndrome. Many cases of substernal goiter are asymptomatic. 7 General indications for total thyroidectomy include: thyroid cancer, toxic multinodular goiter, toxic adenomas, and goiter with compressive symptoms. 8 Regarding those with substernal extension, some authors state that simply the presence of substernal extension is an indication for surgery. 3 Others reserve surgery for cases with significant symptoms, radiographic evidence of tracheal deviation, or progressive enlargement during surveillance.9-11
In goiter with substernal extension, the question of whether a sternotomy will be required is one of the most integral parts of preoperative planning. It has been shown that over 90% of substernal goiters can be safely and definitively removed through a cervical approach, although given that sternotomy is still required in select cases, careful preoperative planning and consultation of a thoracic surgeon are still required. 12 Many preoperative factors have been shown to increase the likelihood of requiring sternotomy for successful gland removal. Harder thyroid tissue radiodensity, 13 posterior mediastinal involvement,13-15 subcarinal extension,13,14 presence of an ectopic nodule, 14 extension beyond the aortic arch,15,16 and a thoracic goiter component wider than the thoracic inlet 16 have all been shown to correlate with the need for intraoperative sternotomy.
In removal of substernal goiter via a transcervical incision, the successful and safe mobilization of the inferior aspect of the thyroid from its mediastinal attachments is integral in the avoidance of sternotomy. Patients at high risk of injury during this step of the procedure commonly have close association of their goiter with 4 important anatomic landmarks, including: the carina, the aortic arch, the pleura of the lungs, and the esophagus. Goiter in close association or beyond the aortic arch represents an especially challenging factor in the safe removal of substernal goiter. 2 Given the close association of many substernal goiters to many important and vital anatomic landmarks; inferior mobilization of the goiter requires careful blunt dissection. This is most commonly attempted after separation of the strap muscles off the goiter followed by establishment of an avascular extracapsular plane anterior to the common carotid artery. The surgeon’s finger is then advanced into this plane and hooked around the inferior aspect of the substernal component in a side-to-side motion to separate the goiter from its mediastinal attachments. In cases where the inferior aspect of the goiter cannot be successfully reached with finger dissection, we propose the use of a surgical spoon as a viable alternative. The spoon is blunt enough to not put nearby structures at risk while also providing the needed length for complete inferior mobilization. The spoon is used to both help free mediastinal attachments and allow slow consistent pressure against the inferior aspect of the thyroid lobe to help deliver it without gland rupture.
Regarding the characteristics of the surgical spoon that we utilized, it is composed of surgical-grade stainless steel and does not bend. It is a “medical instrument” manufactured by Aesculap® (3773 Corporate Parkway Center Valley, 18034 PA, USA). Others may use more routine, commonly available spoons, but we are unable to comment on their suitability as there are many varieties, all subject to different manufacturing processes and standards. Generally, the ideal spoon would be surgical-grade stainless steel without any form of plating (i.e., chrome), should not bend during use, and be autoclavable to ensure sterility.
There have been various surgical uses of a spoon described in the literature. It was first described for use as an orbital retractor during osteotomy placement for the repair of orbital fractures. It has also been described for use in eyelid surgery being placed between the globe and the eyelid to prevent injury to the globe. The spoon has also been described for use in dermabrasion of the lips. A dessert spoon was placed between the teeth and lips to function as both a base of abrasion and to protect the teeth and gums. 17 In open anterior acromioplasty for chronic impingement syndrome, the use of a dessert spoon has been used to protect the underlying rotator cuff while suturing. 18 During arthroscopic meniscal suturing for meniscal repair of the knee, a household spoon has been described as being used to act as a retractor and to protect the underlying neurovascular structures. 19 A spoon has also been described for use to protect against underlying visceral injury while suturing during thoracotomy closure. 20
Conclusions
In patients with substernal goiter requiring surgical removal, a surgical spoon can be a useful adjunct for successful inferior goiter mobilization.
Footnotes
Authors’ Note
This article was presented at the American Head and Neck Society 11th International Conference on Head and Neck Cancer, July 9, 2023 in Montreal, Canada as a poster presentation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.