
Abstract
Introduction
Thyroid surgery has evolved from a procedure with significant morbidity and mortality to one which can often be performed on an outpatient basis. Massive goiter or extensive substernal goiter are considered relative contraindications to outpatient surgery 1 and they present additional challenges in the community setting. Though most substernal goiters can be removed via cervicotomy alone, extent of disease and relationship to mediastinal structures may require sternotomy, and the need for this cannot always be predicted preoperatively. The assistance of a thoracic surgeon and additional resources required for sternotomy are not readily available in all facilities where thyroidectomy is performed, but the microdebrider is typically available and familiar to otolaryngologists given pervasive use in sinus surgery. Use of the microdebrider to facilitate removal of substernal goiter via transcervical approach alone has been previously described,2,3 but there has not been report of adoption of this technique in the community setting.
Patients and Methods
Exemption was obtained from the Institutional Review Board (IRB) at St. Luke’s University Health Network. We retrospectively reviewed thyroidectomy cases performed by a single general otolaryngologist (D.M.Y.) in a community setting from January 2017 through December 2019. Microdebrider use was identified in the operative report. The identified charts were reviewed, and sex, age, length of surgery, estimated blood loss (EBL), complications, and length of stay were recorded.
The microdebrider was used in select cases after progressive difficulty was encountered with attempted en bloc removal after standard exposure and dissection. In all cases, a cruciate incision was made through the exposed superficial capsule of the gland using a #15 scalpel blade, and a 4 mm microdebrider blade was inserted. With the tip under direct visualization, the active surface of the device was directed superficially, and power was applied to allow the instrument to work without added manual pressure (Figure 1). Safety is maintained by keeping the active surface toward the superficial surface of the gland, away from deeper structures in the neck and mediastinum, and debulking was repeatedly paused to reassess improvement in manipulation of the goiter and attempt delivery through the relatively narrow thoracic inlet. The device’s suction allows for removal of inferior parenchyma in the thoracic inlet and mediastinum without necessarily blindly placing the device within the mediastinum. Debulking was resumed if needed. Once delivered through the thoracic inlet and cervical incision, the surgery was completed in a standard fashion (Figure 2). A Lukens trap was used to collect tissue removed by the microdebrider and sent with the en bloc specimen to allow for pathologic evaluation.

Safe technique exhibited with blade under direct visualization and the active surface pointed medially to facilitate selective central debulking of the gland.
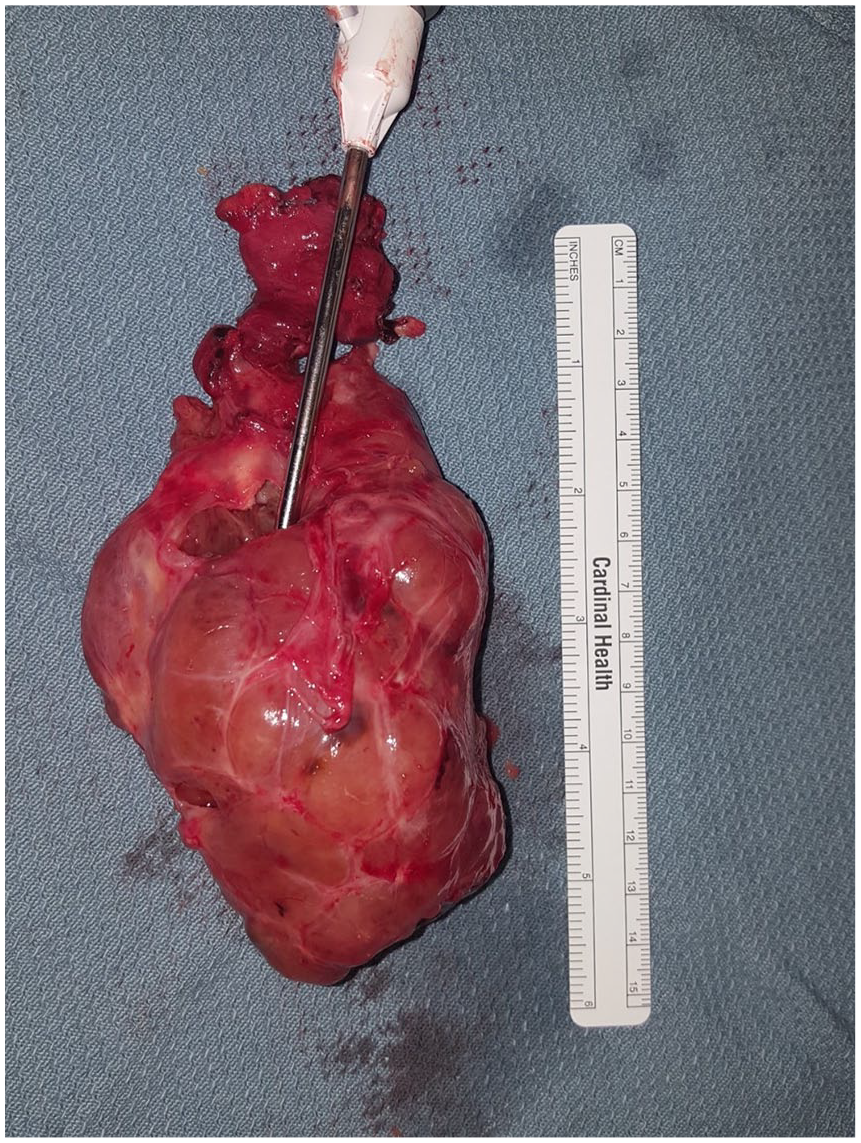
A massive goiter remains after “coring-out,” as less tissue than expected is usually needed to be removed by microdebrider to facilitate manipulation and delivery.
Results
One hundred seventeen thyroid surgeries were performed over the 3 year period and 4 (3.4%) included use of the microdebrider. All 4 cases were identified to be substernal goiters initially on ultrasound and then by computed tomography (CT) cross-sectional imaging. Three patients were female, 1 was male, with a mean age of 58.2 (38-74) years. The average length of surgery was 137 (116-170) minutes. Average EBL was 237.5 (100-500) ml. Closed suction drains were initially placed in 2 of the 4 cases. One patient developed postoperative hematoma requiring return to the operating room, evacuation, and cautery of a bleeding site with an additional EBL of 350 ml, and a drain was then placed. No other complications were encountered, and all patients were discharged after overnight observation. Pathologic evaluation was completed for both the intact gland and Lukens trap collected specimen without difficulty. All thyroid surgeries undertaken during the 3 year period were completed and none required sternotomy.
Discussion
Although many substernal goiters can be removed through a transcervical approach without sternotomy, it can be difficult to predict these patients preoperatively. Identification of which goiters will be amenable to delivery without sternotomy is even more paramount in the community setting where appropriate resources, that is, thoracic surgery colleagues, may not be readily available. Previously, extension below the aortic arch, posterior mediastinal location, duration of disease >160 months, thyroid tissue density, and shape have all been identified as factors affecting need for sternotomy.4,5
Of note, CT scans had been obtained prior to surgery in the 4 cases where the microdebrider was used, and cross-sectional imaging should be obtained in the setting of any suspicion of substernal disease based on symptoms, physical examination, ultrasound, or chest X-ray findings to allow for appropriate planning.
The technique we utilized was developed based on established principles to minimize risk during use of the microdebrider in endoscopic sinus surgery, and it is virtually identical to the method recently described by Dagan and Kleid. 3 We similarly found blood loss during the use of the microdebrider to be much less than expected, and the majority of the EBL encountered in our cases occurred before the decision was made to debulk. Removal of only a small portion of tissue allowed for improved access and mobilization of the substernal goiter out from the mediastinum (Figure 2).
Though one patient developed postoperative hematoma requiring treatment, none of our patients had recurrent laryngeal nerve injury, hypoparathyroidism, or other complications, and all were discharged after overnight observation. Evaluation of a greater number of cases is required to compare EBL, length of surgery, complications, and other outcomes of removal of substernal goiter using this technique compared to removal via cervicotomy alone, or cervicotomy plus thoracotomy. With increased familiarity, otolaryngologists may choose to apply this technique earlier during surgery, which may affect outcomes as well. Before employing this method, ensure the microdebrider is available for use and the operating room staff has familiarity with setup and operation.
The microdebrider can be used to safely and effectively debulk substernal goiter, facilitating removal via transcervical approach alone. Incorporating this technique in community-based thyroid practice for select cases provides the surgeon with an opportunity to increase the breadth and depth of their care by undertaking goiters that would otherwise be unfeasible without additional colleague assistance and providing an option to avoid sternotomy if not predicted preoperatively.
Footnotes
Acknowledgements
The authors have no acknowledgments to disclose.
Authors’ Note
This article was presented at the 2020 American Academy of Otolaryngology—Head and Neck Surgery Annual Meeting & OTO Experience as a virtual poster presentation; September 2020.
Consent Statement
Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.
Data Availability Statement
The data to support the findings of the study are available from the corresponding author on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case series was obtained from the Institutional Review Board (IRB) at St. Luke’s University Health Network (Protocol: SLIR 2020-79).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Institutional Review Board (IRB) at St. Luke’s University Health Network (Protocol: SLIR 2020-79) approved protocols.