
Abstract
Relapsing polychondritis (RP) is a rare chronic inflammatory disease characterized by recurrent inflammation of cartilages throughout the body, with treatment-resistant dizziness and hearing loss in 40%-50% of patients with RP. Although rare, severe binaural hearing loss in RP is an indication for cochlear implantation (CI). Therefore, there are only a few reports on CI insertion in cases of RP. This report describes a 68-year-old woman who developed binaural hearing loss due to RP. She was treated with steroids and immunosuppressive drugs; however, her hearing did not improve significantly, and she relied on written communication for conversation. Subsequently, the patient underwent CI in the right ear. The patient showed improvement in speech perception; at 14 months postoperatively, she was able to speak with lipreading, and at 2 years postoperatively, she was able to speak without lipreading. Previous case reports on CI in patients with RP have shown varying degrees of postoperative hearing improvement. Our case demonstrates the effectiveness of CI in improving hearing and speech recognition in patients with RP having semicircular canal calcification. However, previous reports have shown that speech recognition declines 13 years after CI for RP. Therefore, continuous long-term follow-up is necessary.
Keywords
Introduction
Relapsing polychondritis (RP) is a rare chronic inflammatory disease characterized by recurrent inflammation of cartilages throughout the body and a variety of symptoms. Its characteristic findings include bilateral external auditory canal chondritis, nonerosive seronegative inflammatory arthritis, nasal chondritis, ocular inflammation, airway chondritis, and vestibulocochlear disturbances. Dizziness and hearing loss occur in 40%-50% of RP cases; hearing loss in RP usually does not respond well to steroid administration. 1 Although rare, bilateral deafness in patients with RP is an indication for cochlear implantation (CI). There are only a few reports of patients with RP undergoing CI, and to our knowledge, there have been no reports of patients with semicircular canal calcification. In this report, we describe a case of bilateral hearing loss due to RP with semicircular canal calcification treated with CI, and present a literature review.
Case report
A 68-year-old woman presented with left auricular redness for 2 months, hearing loss for 1 month, and bilateral visual field disturbances for 1 week. She had a medical history of type 2 diabetes mellitus, hypertension, hyperlipidemia, and primary biliary cirrhosis. The patient also had left auricular chondritis and severe bilateral sensorineural hearing loss. She also had bilateral conjunctivitis/uveitis and nondestructive polyarthritis, as diagnosed by an ophthalmologist and physician, respectively. We performed a biopsy of the left auricular cartilage, which revealed a strong inflammatory cell infiltrate, primarily composed of lymphocytes, and significant cartilage destruction. This finding led to the diagnosis of RP. Rheumatology specialists started steroid therapy immediately after diagnosis. They added cyclophosphamide 1 month after steroid therapy; azathioprene was added 8 months later. Although her general condition improved, her hearing function did not change, and she had to communicate in writing.
Her pure-tone hearing thresholds were approximately 100 dB at 2-4 kHz on the right side and were almost scaled out bilaterally (Figure 1A). Distortion-product otoacoustic emission showed no bilateral response. Auditory brainstem response (ABR) showed a wave I of 100 dB on the right side, but no response on the left. Caloric testing revealed severe bilateral semicircular canal paralysis. Functional gains from hearing aids were not serviceable. Computed tomography showed calcification of the bilateral semicircular canals, but no calcification in the cochlea (Figure 1B). Magnetic resonance imaging: fast imaging employing steady-state acquisition revealed a decreased signal in the right and left semicircular canals and inflammatory findings in the mastoid cavity. However, no reduction in the intracochlear signal was observed (Figure 1C).
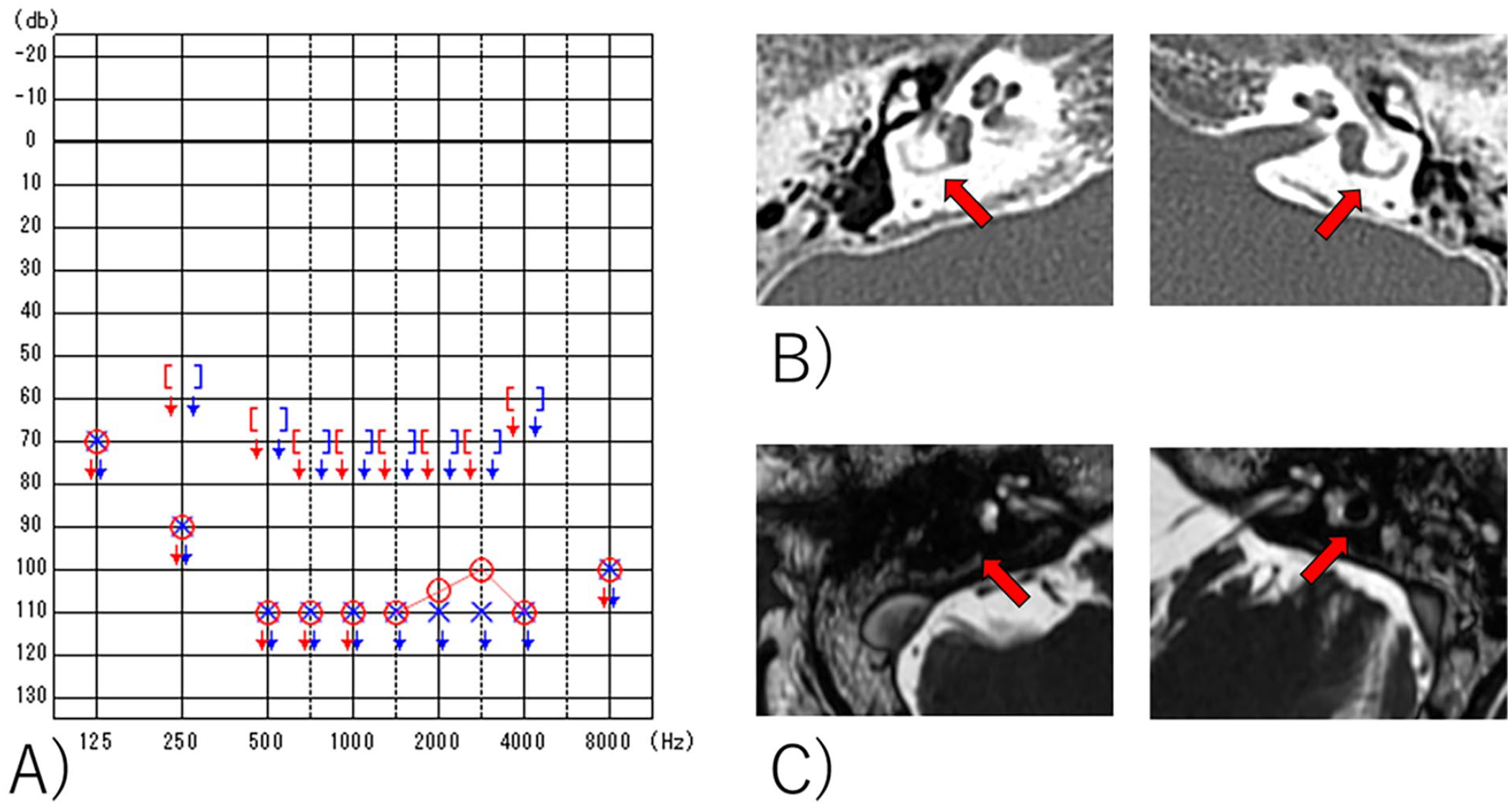
(A) Pure tone hearing thresholds. (B) Temporal bone CT findings. Calcification of right and left lateral semicircular canals present (arrows), but intracochlear calcification was not comfirmed. (C) Inner ear MRI FIESTA findings. Decreased signal in right and left semicircular canals (arrows) and inflammatory findings in mastoid cavity was present, but the signal of cochlea was preserved.
Her hearing loss was bilaterally profound, and she wanted to undergo hearing restoration. Although her hearing was almost scaled out bilaterally, she retained hearing function of approximately 100 dB at 2-4 kHz in the right ear and did not want bilateral simultaneous surgery. We planned CI in the right ear because it had more hopeful hearing results. We chose an implant with a stylet (CI612; Cochlea Corp., Sydney, NSW, Australia) because calcification of the cochlear duct was suspected owing to the presence of bilateral lateral semicircular canal calcification.
Transmastoid CI surgery was performed. Although the round window niche could be identified, the round window membrane could not, probably because of inner ear calcification. The electrode was inserted via a cochleostomy. Impedance, neural response telemetry, and wave V of the electrically evoked ABR were good for all electrodes.
The postoperative course was uneventful, and the patient was discharged 1 week postoperatively. Five months after CI, the hearing threshold level was approximately 30-40 dB. She showed improvement in speech recognition tests (70 dB) with 23% consonants, 36% monosyllables, 12% words, and 15% sentences 11 months postoperatively. She was able to hear speech with lipreading 14 months postoperatively. Her speech recognition ability gradually improved, and she was able to understand conversation without lipreading if spoken slowly 2 years after CI surgery.
Discussion
The pathology of RP remains unclear, but the involvement of autoantibodies against types II, IX, XI collagen and matrilin I has been reported.2,3 The diagnosis of RP is based on the following criteria: (1) bilateral auricular chondritis, (2) nonerosive polyarthritis, (3) rhinochondritis, (4) ocular symptoms (conjunctivitis, scleritis, uveitis, etc.), (5) laryngeal airway chondritis, and (6) vestibulocochlear dysfunction (sensorineural hearing loss, tinnitus, dizziness). Diagnosis is based on at least 3 clinical symptoms or at least 1 clinical symptom with histological findings.1,4 In the present case, the diagnosis of RP was made based on bilateral auricular chondritis, nonerosive polyarthritis, ocular symptoms, and vestibulocochlear dysfunction, with histological findings.
Vestibulocochlear dysfunction occurs in 40%-50% of patients with RP. 1 There are a few reports of hearing loss in RP, with Bachor’s series of 9 cases being the most notable. 5 In this series, 7 of the 9 patients had sensorineural hearing loss, but only 1 had severe sensorineural hearing loss. Seven of the 9 patients were administered steroids; however, only 2 showed improvement. This suggests that RP-induced sensorineural hearing loss tends to respond poorly to steroids. Our patient had profound bilateral hearing loss, which is relatively rare. She did not show improvement with steroids, which is consistent with the findings of previous reports.
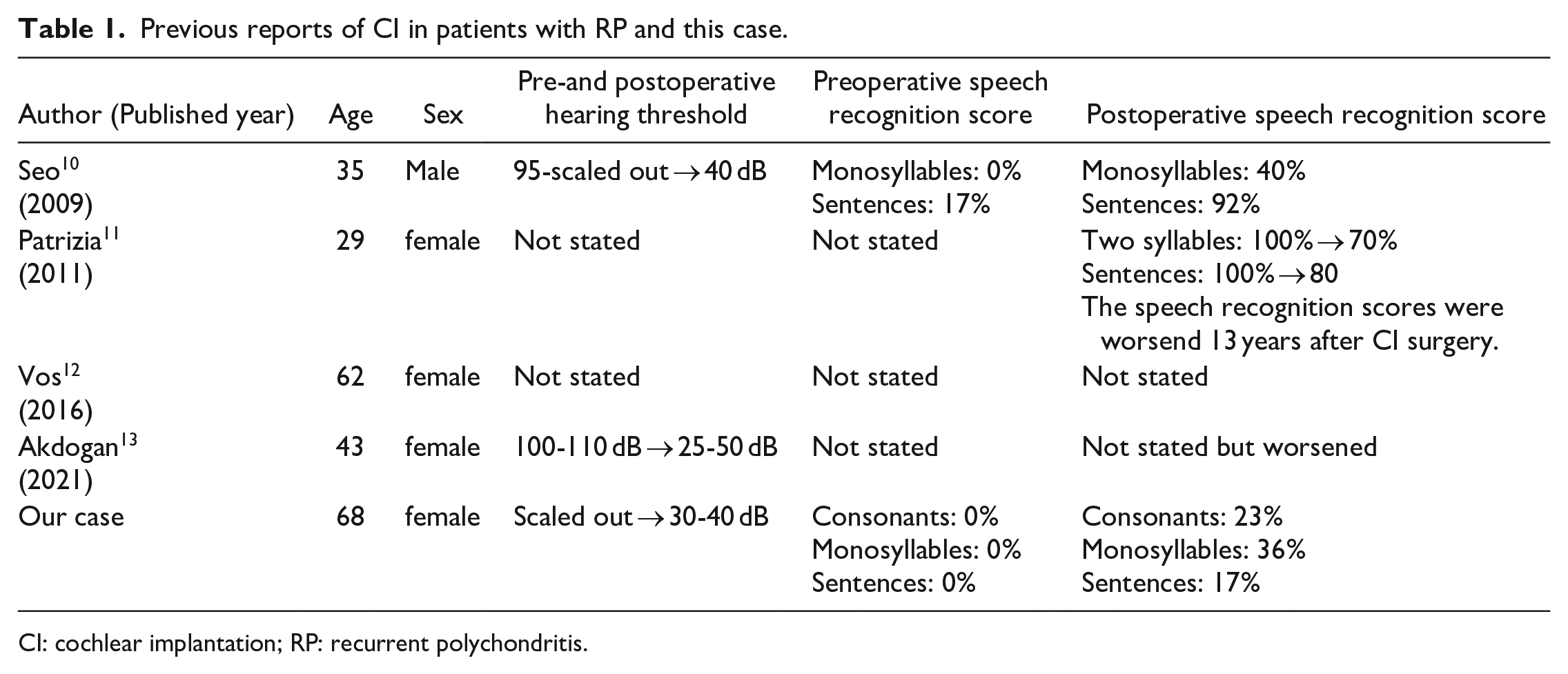
In general, cyclophosphamide, cyclosporine A, methotrexate, and azathioprine are recommended for patients with RP who have shown poor improvement with steroids.1,6 -9 Our patient was also treated with cyclophosphamide and azathioprine; although her general condition improved, there was no improvement in hearing function, and she became a candidate for CI. There have been 4 previous reports of CI in patients with RP10 -13 (Table 1). The first report of CI in a patient with RP was published by Seo et al; a 35-year-old man underwent CI, and his hearing threshold improved from 95-scaled out to 40 dB. Speech recognition improved from 0% to 40% for monosyllables, and from 17% to 92% for sentences. 10 The second case was reported by Patrizia et al.; a 29-year-old woman improved her speech recognition score to 100% for both 2 syllables and sentences, but preoperative speech recognition scores were not stated. However, 13 years postoperatively, there was a decline in speech recognition scores from 100% to 70% for 2 syllables, and from 100% to 80% for sentences. 11 A third case was reported by Vos et al; a 62-year-old woman showed improved speech recognition after surgery, but preoperative and accurate speech recognition scores were not stated. 12 The fourth case was reported by Akdogan et al; a 43-year-old woman showed hearing threshold improvement from 100-110 dB to 25-50 dB. However, her speech recognition performance worsened after CI surgery. 13 In our case, the auditory threshold of a 68-year-old woman improved from scaled out to 30-40 dB. Speech recognition scores improved from 0% to 23% for consonants, 0% to 36% for monosyllables, and 0% to 17% for sentences. She was able to understand conversations without lipreading if spoken slowly. Although she and her family were satisfied with the results of CI, we must carefully monitor the long-term course of her hearing and speech function, as long-term hearing prognosis may occasionally be suboptimal. 13 Compared with previous reports, the speech recognition score in this case was not optimal, especially for sentences. A possible reason is that the patient might have a mild/slight developmental disorder, and if she was not able to understand long or difficult sentences before RP onset, it may have affected her ability to understand sentences after CI. However, there are other possible pathological reasons, such as central hearing impairment caused by RP. In this case, speech intelligibility must be carefully monitored.
Previous reports of CI in patients with RP and this case.
CI: cochlear implantation; RP: recurrent polychondritis.
Conclusion
In this case, CI was performed for bilateral deafness caused by RP with semicircular canal calcification, and the patient showed improved hearing function and was able to understand conversation without lipreading, which suggests the effectiveness of CI for RP. However, the long-term course of hearing and speech function must be carefully monitored, as long-term hearing prognosis may occasionally be suboptimal.
Footnotes
Date Availability Statement
Sharing does not apply to this article because no date sets were generated or analyzed during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Grant-in-Aid for Early-Career Scientists (19K18744) from the Ja-pan Society for the Promotion of Science and the Takeda Science Foundation.
Ethical Approval
The study was conducted with the approval of the Institutional Review Board of Keio University (Ethics Approval Number 20200033, April 27, 2020).
Statement of Human and Animal Rights
All procedures performed in this study were in accordance with the 1964 Helsinki declaration and its later amendments.
Statement of Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.