
Abstract
Viruses are often implicated as a cause of sensorineural hearing loss (SNHL), particularly sudden cases, including COVID-19. Determining the viral mechanism that leads to hearing loss is necessary for its future prevention and treatment. The 47-year-old woman who is the subject of this case study presented with sudden SNHL following multiple infections of COVID-19. Following a trial of a contralateral routing of sound device, she received a right cochlear implant (CI). Following a period of high performance, additional cases of COVID-19 infection and device failure issues resulted in the explant/reimplant of 1 ear and implantation of the contralateral ear. Despite extensive rehabilitation after these events, the patient continues to experience difficulties in speech understanding, not reaching her initial high levels of right ear performance. Further research is needed to determine the implications of COVID-19 as it relates to SNHL. This case study aimed to highlight the course of treatment and provide insight into the impact of COVID-19 on sudden hearing loss and its relationship to CI performance.
Introduction
Sensorineural hearing loss (SNHL) can occur secondary to numerous viral infections, including COVID-19.1,2 While the etiology of hearing loss due to viral infections varies by virus, it has been suggested that COVID-19 may cause inflammation of nervous tissue and affect both the inner ear and auditory pathways. 3 The link between SNHL and COVID-19 was first reported in April 2020, in a COVID-19 patient with coincident SNHL. 4 Since then, there have been other reports on the association between SNHL and COVID-19 infection. 5 The primary treatment for patients with sudden SNHL (SSNHL) post COVID-19 infection has been systemic steroid treatment, intratympanic injection, combined oral and intratympanic corticosteroids, and hyperbaric oxygen therapy. 5 Typically, steroid treatment has offered the most potential for improvement of SSNHL, but if steroids or other treatment modalities fail, cochlear implant (CI) may be an option for hearing rehabilitation.6,7 This report presents a case of steroid-resistant, bilateral, sequential SSNHL associated with recurrent COVID-19 infections. We also highlight nuances regarding her eventual rehabilitation with bilateral CI.
Case Report
This case study (IRB23-1872) was deemed exempt by the University of Chicago Medicine Institutional Review Board. A 47-year-old female, fully vaccinated for COVID-19, with a history of premorbid bilateral mild to moderate SNHL (Figure 1), presented with sudden right-sided hearing loss in January 2022 after a COVID-19 infection. It should be noted this was her third documented COVID-19 infection. Otologic examination was normal, and an audiogram demonstrated a profound right-sided SNHL, as depicted in Figure 2. Timely treatment with a high-dose oral steroid taper and 3 rounds of intratympanic steroid injections resulted in no objective hearing improvement. Magnetic resonance imaging did not demonstrate any retrocochlear pathology.
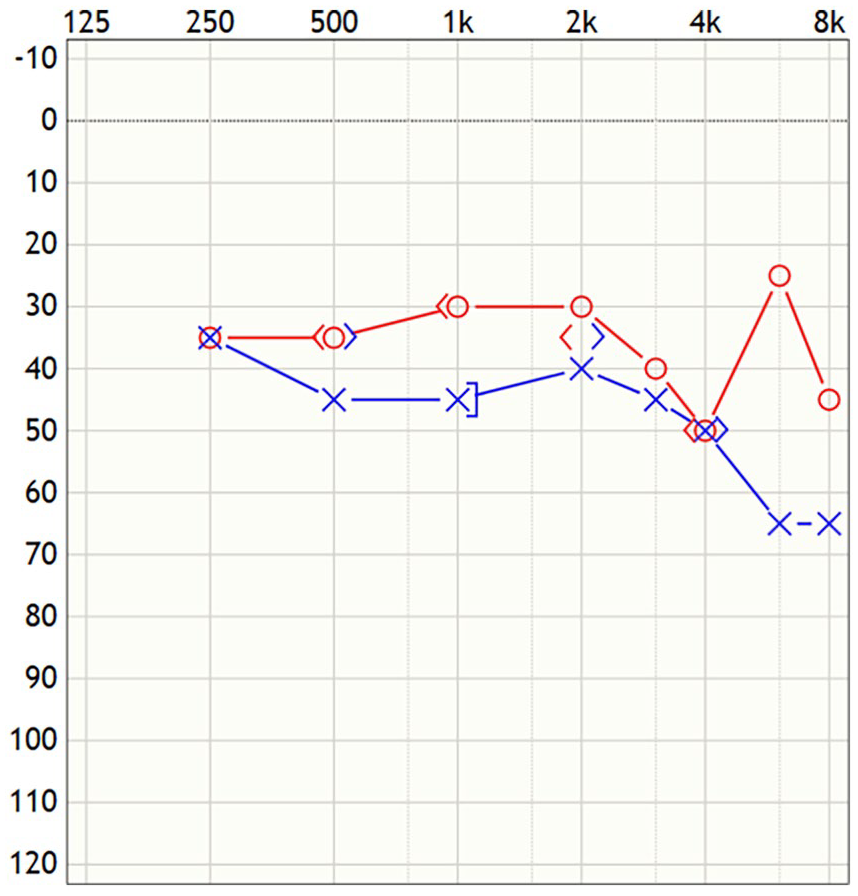
Bilateral mild to moderate sensorineural hearing loss prior to the onset of COVID-19 infections.
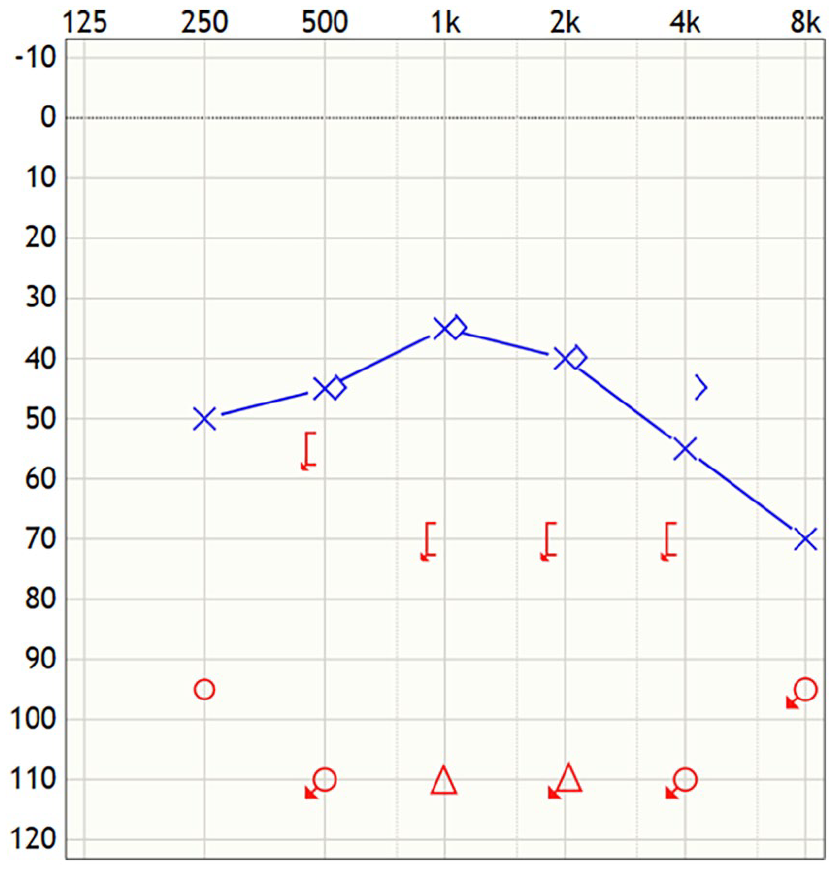
Audiogram revealing sudden, right profound sensorineural hearing loss following the third documented COVID-19 infection.
After a trial with a contralateral routing of signal device and no additional improvement in her hearing, she underwent an uncomplicated right CI with a Cochlear 632 (Cochlear Ltd.), slim modiolar device. After surgery, she experienced mild vertigo during the first week but had an uncomplicated recovery. Six months later, she achieved an 89% score on AzBio testing in quiet and was considered a high-achieving user, having returned to work.
Two months after her right CI surgery, she reported a sudden hearing decline in her left ear. An audiogram revealed profound SNHL in her left ear, depicted in Figure 3, and there was no improvement with high-dose steroid treatment. Due to this unusual history of bilateral, sequential sudden losses, a rheumatologic workup was performed. During this workup, she was found to be negative for antinuclear antibodies, perinuclear antineutrophil cytoplasmic antibodies, and cytoplasmic antineutrophil cytoplasmic antibodies. In addition, serum protein electrophoresis without monoclonal protein was detected. Complete blood count, comprehensive metabolic panel, hemoglobin A1c, thyroid stimulating hormone, vitamin D, immunoglobulin (IgA), and tissue transglutaminase IgA were all within normal limits. Urine analysis showed no hematuria or proteinuria. Other causes that were not high on the differential included Lyme disease and syphilis, but she had recently tested negative for syphilis antibodies as part of a separate evaluation. Lyme disease was not tested for, given a low suspicion. She was also HIV-negative. It should also be noted that after a prior abdominal surgery, she had a hematology workup for idiopathic portal vein thrombosis, which was ultimately negative.
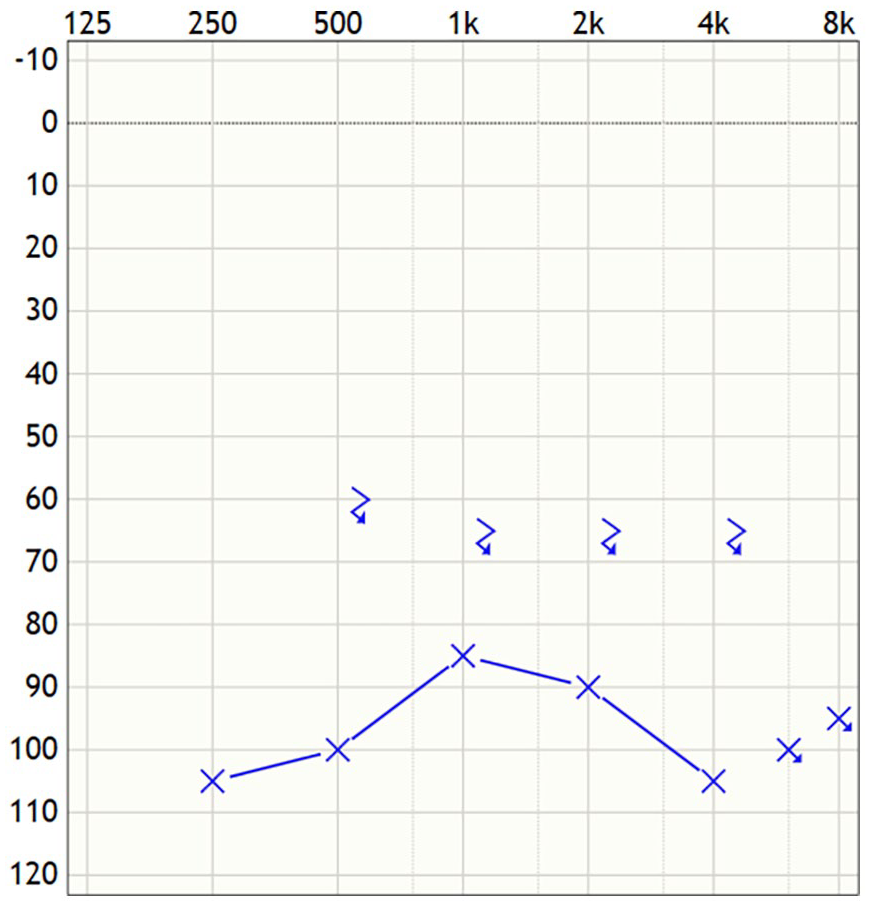
Audiogram of the left ear 2 months after right cochlear implantation. The patient reported a sudden change in hearing, which revealed a profound sensorineural hearing loss in the left ear.
After a period of observation, she eventually elected to have a left CI performed (Cochlear 632 device; Cochlear Ltd.) in March 2023, and the surgery was uncomplicated. Soon after the left ear implantation, there was a sudden, subjective decline in her right implant performance. Objective testing noted short electrodes at 9 and 10, loudness growth was unable to be achieved, and sound remained barely audible. She later reported a consistent throbbing sensation and pain at the right incision site. An integrity test did not reveal any failure with the right implant. Our team considered these changes in the right implant to be a soft failure, and she underwent a subsequent right CI revision in June with a Cochlear 632 device (Cochlear Ltd.) without complication. Normal electrode impedances and electrically evoked compound action potential responses were noted intraoperatively. Final analysis from the manufacturer on the explanted device revealed short circuit electrodes caused by physical contact of the electrode wire bundle to the electrode ring, causing insulation damage.
Despite the revision of her right CI, she still has difficulty understanding speech, especially in complex environments. Her left CI continues to have a high-pitched sound quality and poor understanding with a lack of loudness growth, raising concerns for a potential soft failure. A device integrity test for the left CI was ultimately unremarkable. Her continued auditory rehabilitation has unfortunately been impeded by another recent COVID-19 infection. The resulting slow hearing rehabilitation with both devices has prevented a return to work as she is unable to comprehend verbal communication.
Discussion
This case presents an unusual history of bilateral, sequential sudden hearing loss in a patient with 5 documented COVID-19 infections between 2020 and 2023 and poor rehabilitation after bilateral, sequential CI. Despite having received appropriate vaccinations and boosters, the exact nature of her recurrent COVID-19 infections remains undetermined. While she does have a history of urticaria, rhinitis, and food allergies, there does not appear to be a component of immune deficiency (had normal IgA levels) or autoimmune disease. Further immunological workup could be undertaken to investigate the cause of her COVID-19 sensitivity. To date, only a few cases have reported the use of CI for profound hearing loss related to COVID-19 infections. A 2023 case report follows a patient with profound bilateral SNHL post COVID-19 who received bilateral CI. 8 Two months after activation, this patient achieved improved understanding and decreased tinnitus. There are 2 other published reports of patients who received CI post COVID-19 who had satisfactory outcomes.9,10 These reports, while limited in numbers, indicate that patients with SNHL, presumably secondary to COVID-19 illness, are expected to perform as well as other patients with different SNHL etiologies. Unlike these cases, our patient experienced poor performance after revision surgery of the right implant and had additional symptomatic COVID-19 infection despite appropriate vaccination.
An interesting aspect of our patient’s case is the failure of her right implant, which required eventual reimplantation. Analysis revealed electrode shorts, and we believe this to be the ultimate cause of failure, as opposed to some effect from her prior COVID-19 illness. However, her poor performance after revision suggests there may be some neural dysfunction of unknown etiology. Saki et al 11 have reported the first 2 cases of CI failure in previously implanted pediatric patients following COVID-19 infection. They presented with speech perception deterioration in both quiet and noisy settings. COVID-19 infection was not suspected until the patients developed interstitial pneumonia. 11 While there have been no in-depth studies regarding long-term effects after infection, the COVID-19 virus utilizes the angiotensin-converting enzyme 2 receptor to infiltrate cochlear endothelial cells and the surrounding neurons.11,12 Our patient’s repeated COVID-19 infections may have damaged spiral ganglion cells, causing poor performance in the right ear after reimplantation and limited benefit from the left implant. Degradation along the auditory neural pathway prevents proper central processing. The COVID-19 virus also deoxygenates erythrocytes, which may lead to hypoxia within cortical regions involved in auditory processing and potential permanent damage and hearing loss. 13
Identifying COVID-19 as a potential cause of SNHL can affect the chosen course of treatment. 14 Specific markers, such as elevated C-reactive protein, neutrophil-to-lymphocyte ratio, and systemic immune-inflammation index, may be markers of poor prognosis in COVID-19-related SNHL. 15 How helpful these markers may be in predicting treatment response with steroids or CI performance is unclear. Ultimately, COVID-19 may damage numerous potential targets within the central and peripheral auditory pathways, and there is not one common phenotype of COVID-associated hearing loss. Further research is needed to understand how COVID-19 contributes to SNHL, which will have significant implications for treatment and rehabilitation options.
Footnotes
Data Availability
Information supporting this case study is available from the corresponding author, JDS, on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
As this is a case study, it was deemed exempt from the Institutional Review Board process at the University of Chicago.
Informed Consent
Written consent was obtained from the subject of this case study who allowed for its submission.