
Abstract
Necrotizing soft tissue infection (NSTI) is a rare, but life-threatening, complication of head and neck surgery. We present a 70-year-old male with a history of immunosuppression who presented with polymicrobial NSTI following parotidectomy and neck dissection for cutaneous squamous cell carcinoma. The objective of this report was to promote awareness for NSTI following parotidectomy and selective neck dissection and highlight the management measures that can optimize survival outcomes. We performed a database search that identified 1,025 citations, of which 5 articles described classified as craniocervical necrotizing fasciitis following major head and neck surgery. Consent was obtained from the patient for inclusion in the research study and Institutional Review Board approval was waived. Our literature review yielded 6 cases of craniocervical necrotizing fasciitis following major head and neck surgery. This NSTI, however—unlike the others previously reported—was predominantly mediated by Escherichia coli, a bacterium associated with elevated mortality rates. Despite immediate awake fiberoptic intubation, repeated surgical debridement, and empirical antibiotic therapy, he deteriorated rapidly and was withdrawn from life-support on postoperative day seven. Prophylactic antibiotics, airway management, prompt diagnosis, and surgical debridement are critical for limiting mortality in NSTI of the head and neck.
Introduction
Necrotizing soft tissue infection (NSTI) has a mortality rate of 6%-33%. 1 Several factors, including age, sex, and immunosuppression, are associated with mortality in NSTI. These infections are often polymicrobial, and diagnosis is based on debridement of necrotic tissue. In conjunction with antibiotic therapy and supportive management, prompt surgical debridement of affected tissue in NSTI decreases mortality by 50%.
Head and neck NSTIs, often classified as craniocervical necrotizing fasciitis (CCNF) are often secondary to odontogenic or pharyngeal infection. 2 CCNF accounts for up to 10% of NSTIs and is associated with a high rate of mortality due to deep neck space involvement and a risk of mediastinitis. Herein, we report the first case of lethal CCNF developing within 24 h of parotidectomy and selective neck dissection for metastatic cutaneous squamous cell carcinoma (SCC). We also performed a literature review of all reported cases of NSTI following major head and neck surgery.
Case Report
A 70-year-old male presented with metastatic cutaneous SCC. One year prior to presentation, he underwent a wide local excision of a left preauricular spindle cell SCC with negative margins. His medical history was significant for end-stage renal disease, type 2 diabetes mellitus, pulmonary hypertension, ischemic heart disease, and chronic obstructive pulmonary disease. He was taking 15 mg prednisone daily for a presumed diagnosis of IgG4 disease and idiopathic retroperitoneal fibrosis. His staging CT scans demonstrated a 2.2 cm enhancing lesion of his left parotid with no radiological evidence of regional or distant metastases (Figure 1). He underwent left subtotal parotidectomy with facial nerve preservation, ipsilateral selective neck dissection (Ib–IV), and cervico-rotational flap for local reconstruction. His final pathology demonstrated a rTxN3M0 spindle cell SCC of his left intra-parotid lymph node with involvement of the parotid gland. Lymphadenectomy demonstrated 42 ipsilateral benign lymph nodes and a benign submandibular gland.

Axial CT neck with contrast demonstrating enhancing lesion of his left superficial parotid gland consistent with his primary squamous cell carcinoma.
He received preoperative cefazolin within 60 min of the initial incision, and he was started on prophylactic cefazolin and metronidazole postoperatively. On postoperative day (POD) one, he developed fever, hypotension, and tachycardia alongside rapidly progressive leukocytosis and altered level of consciousness. He subsequently required medical resuscitation for acute-onset stridor and oxygen desaturation. He underwent awake fiberoptic intubation due to supraglottic edema. He continued to deteriorate clinically requiring initiation of norepinephrine and empirical treatment with piperacillin-tazobactam, vancomycin, and clindamycin. A CT scan of his neck demonstrated aggressive infectious changes including gas loculations within the deep spaces of the left neck alongside a concern for mediastinitis (Figure 2A–B). His blood and urine cultures did not demonstrate any pathogenic bacterial growth. He underwent urgent left neck exploration and surgical debridement on POD2 with final pathology demonstrating focal necrosis of the sternocleidomastoid muscle suggestive of necrotizing fasciitis (Figure 3). His tissue culture was positive for pan-susceptible Escherichia coli (E. coli), in addition to Clostridium perfringens, with concerns for polymicrobial infection. He underwent repeat debridement on POD3. Despite appropriate management, he continued to decline clinically, and his family opted to withdraw care. He passed away peacefully on POD7.
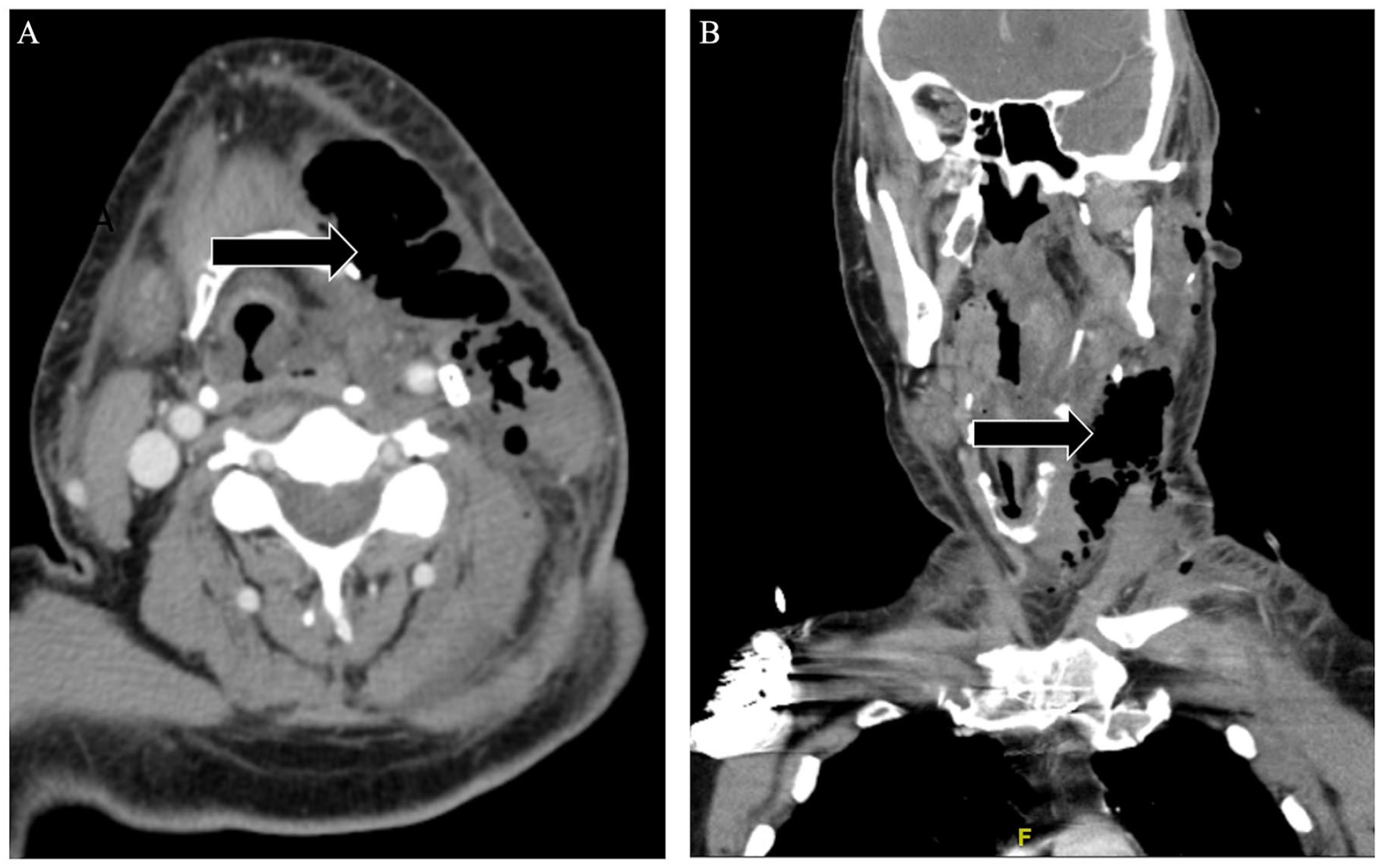
(A). Axial CT neck with contrast demonstrating gas loculations and soft tissue inflammation along the left neck at the level of the hyoid bone. (B). Coronal CT neck with contrast demonstrating gas loculations within the left lateral neck suggesting involvement of the deep neck spaces to the level of the glottis.

Clinical photograph demonstrating extent of surgical debridement following the diagnosis of necrotizing soft tissue infection.
Discussion
We present the first description of CCNF developing in an immunosuppressed patient within 24 h of parotidectomy and selective neck dissection performed for regionally metastatic spindle cell SCC. We performed a database search that identified 1,025 citations, of which five articles described CCNF following major head and neck surgery (Table 1; Appendix 1).2 -6
Craniocervical Necrotizing Fasciitis Following Major Head and Neck Surgery (N = 6).
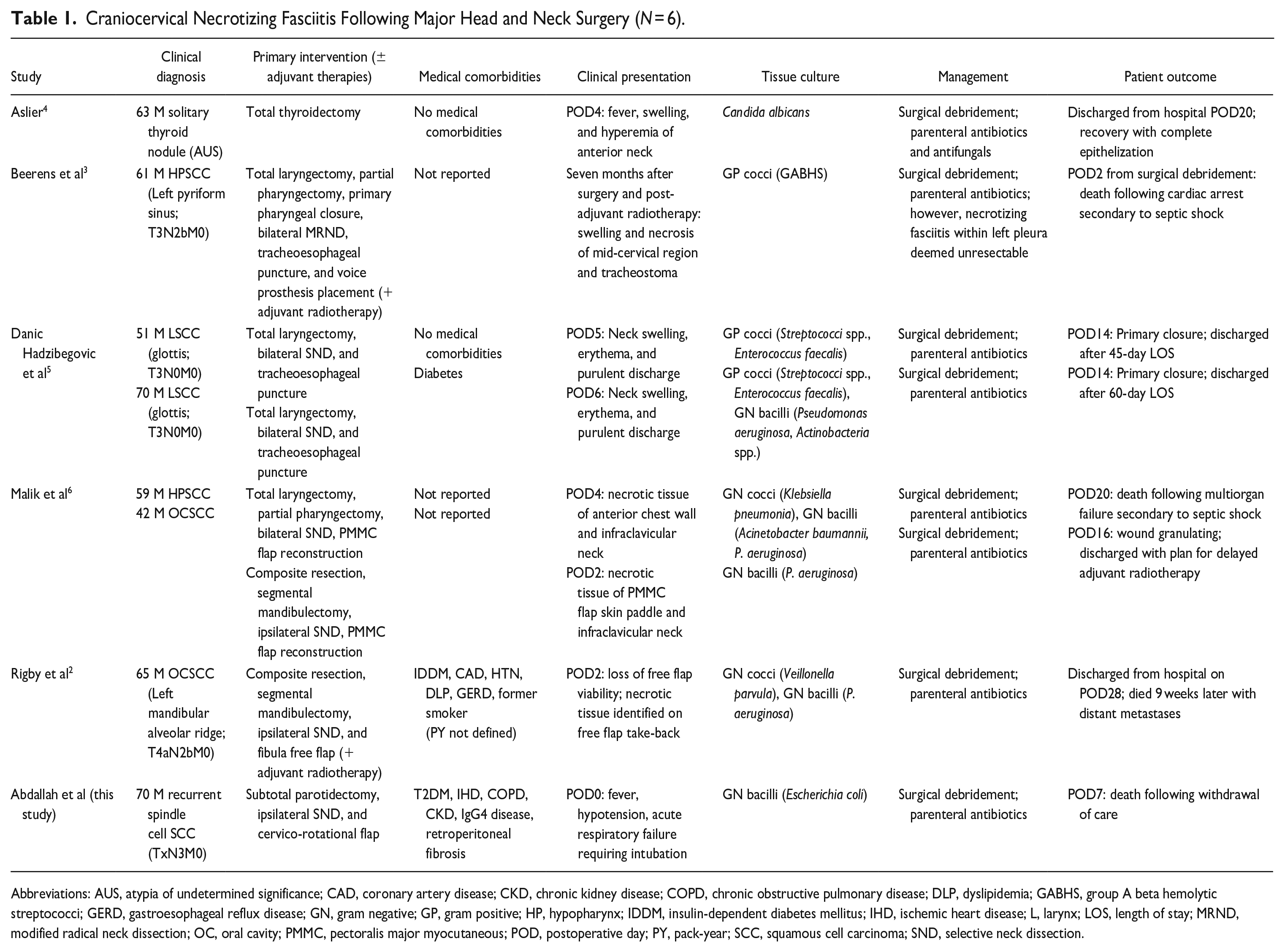
Abbreviations: AUS, atypia of undetermined significance; CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DLP, dyslipidemia; GABHS, group A beta hemolytic streptococci; GERD, gastroesophageal reflux disease; GN, gram negative; GP, gram positive; HP, hypopharynx; IDDM, insulin-dependent diabetes mellitus; IHD, ischemic heart disease; L, larynx; LOS, length of stay; MRND, modified radical neck dissection; OC, oral cavity; PMMC, pectoralis major myocutaneous; POD, postoperative day; PY, pack-year; SCC, squamous cell carcinoma; SND, selective neck dissection.
Our review demonstrates a mortality rate of 37.5% for CCNF following major head and neck surgery with most cases being secondary to polymicrobial infection, often including Streptococci spp., (Table 1). This is consistent with mortality in CCNF being upward of 50% due to the risk of mediastinal extension. 3 Here, E. coli was considered the primary pathogenic organism and is one of the most common isolates in necrotizing fasciitis of immunocompromised patients.7,8 The other isolated pathogen, C. perfringens, results in deadly clostridial myonecrosis, and accelerated clinical deterioration in immunocompromised patients, with a mortality rate up to 100% if surgical treatment is delayed.9 -11 Similar to C. perfringens, the overall reported incidence of E. coli-mediated NSTI is low, with rates from 0% to 10%. 12 These infections also vary geographically, with a predominance of reporting occurring in Asian countries.7,10,12 In our literature review, 57.1% (4/7) of patients received pre- or intraoperative antibiotics, but, in contrast to this case, all patients who received prophylactic antibiotics had recovered by the time of discharge.2,4,5 This NSTI, however, in addition to having a polymicrobial profile, was predominantly mediated by E. coli, which is associated with a NSTI mortality rate as high as 60%. 10 Currently, monobacterial necrotizing fasciitis caused by gram negative pathogens, such as E. coli, is not accounted for in any NF classification system. 8 This rare infection has been documented in case series as occurring more frequently in elderly patients with severe comorbidities such as liver cirrhosis or end-stage renal disease.8,12 Like this report, patients who were immunosuppressed or had recent surgery for underlying malignancy had worse outcomes. 8 Extraintestinal pathogenic E. Coli strain, which harbors virulence factors that can facilitate hematogenous spread, has been isolated from tissue samples of E. coli mediated NSTI.10,12 E. coli NSTI often presents initially as E. coli bacteremia that can subsequently develop septic shock.7,8,12 Controlled administration of E. coli toxin has led to dermal necrosis and accelerated death in rabbit models of NSTI. 12 In both this case and the current literature, the deadly nature of E. coli in NSTI was likely mediated by hematogenous spread, and a multifactorial interaction between pathogenic, clinical, and patient factors.
Preoperative antimicrobial practices can improve postoperative NSTI rates, but empiric antibiotics do not eliminate this risk.13,14 Despite using aggressive and sensitive antibiotic therapy, Bekal et al. 15 reported their patient’s death within 16 h of E. coli mediated NSTI onset following major gynecologic surgery. Cefazolin is bactericidal against both gram-positive cocci and gram-negative bacteria such as E. coli, but resistance rates do continue to increase, with rates as high as 34% in the United States. Yet, even when treated with sensitive antibiotic therapy, survival rates may be poor due to the presence of virulence factors that increase pathogenicity.8,10,16 Describing such a rare, but destructive, perioperative complication is important in raising surgeon awareness for NSTI after major head and neck surgery. Prevention, prompt diagnosis, and urgent surgical debridement are tenets in optimizing outcomes in NSTI. In major head and neck surgery, which is often a clean-contaminated field, perioperative antibiotics 24–48 h after surgery helps to prevent surgical site infection. 13 After NSTI diagnosis, prompt—often repeated—surgical debridement, empiric antibiotics, and close monitoring improves survival outcomes. In addition to these critical components in NSTI management, head and neck surgeons must promptly identify airway compromise and the potential need for prophylactic intubation or tracheostomy to help ensure airway securement.
Conclusions
In high-risk patients, life-threatening CCNF can develop within hours of major head and neck surgery. Hence, initiating perioperative antimicrobials and maintaining an index of suspicion for CCNF can help to ensure prompt airway management and urgent surgical debridement to optimize survival outcomes.
Footnotes
Appendix
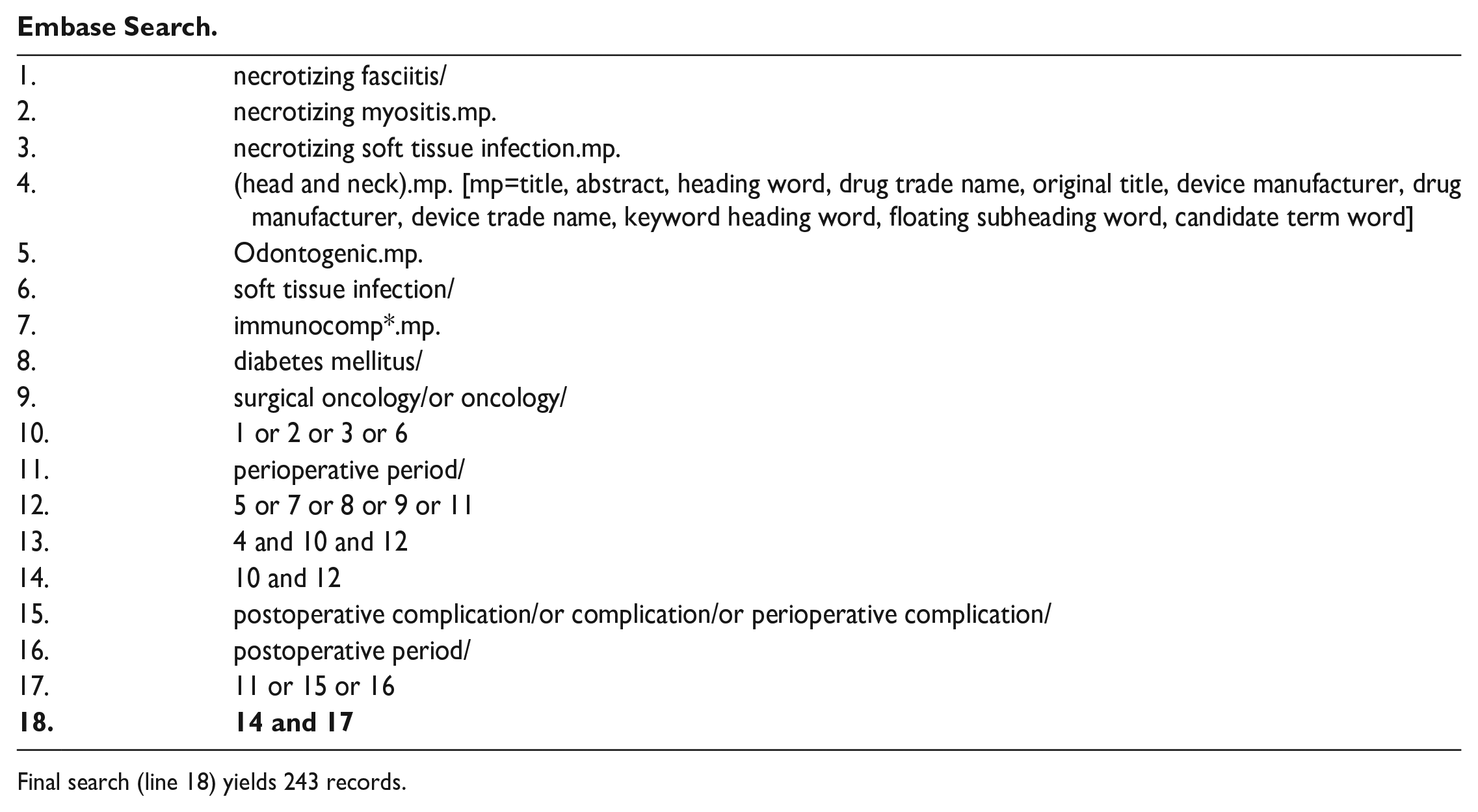
Embase Search.
| 1. | necrotizing fasciitis/ |
| 2. | necrotizing myositis.mp. |
| 3. | necrotizing soft tissue infection.mp. |
| 4. | (head and neck).mp. [mp=title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word] |
| 5. | Odontogenic.mp. |
| 6. | soft tissue infection/ |
| 7. | immunocomp*.mp. |
| 8. | diabetes mellitus/ |
| 9. | surgical oncology/or oncology/ |
| 10. | 1 or 2 or 3 or 6 |
| 11. | perioperative period/ |
| 12. | 5 or 7 or 8 or 9 or 11 |
| 13. | 4 and 10 and 12 |
| 14. | 10 and 12 |
| 15. | postoperative complication/or complication/or perioperative complication/ |
| 16. | postoperative period/ |
| 17. | 11 or 15 or 16 |
|
|
|
Final search (line 18) yields 243 records.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.